






Dysmenorrhea
Dysmenorrhea is a medical term for painful periods or painful menstruation with either menstrual cramps with no visible cause (primary dysmenorrhea) or secondary to specific pelvic pathology (secondary dysmenorrhea) 1). Period pain is very common: most girls and women have pain of varying intensity at some point during their period. In 10 out of 100 women the pain is so bad that they’re unable to carry out their usual daily activities on one to three days every month. The pain is usually worse in women under the age of 20. It usually gets better or even goes away completely within a few years of their first period. In many women period pain becomes milder after the birth of their first child.
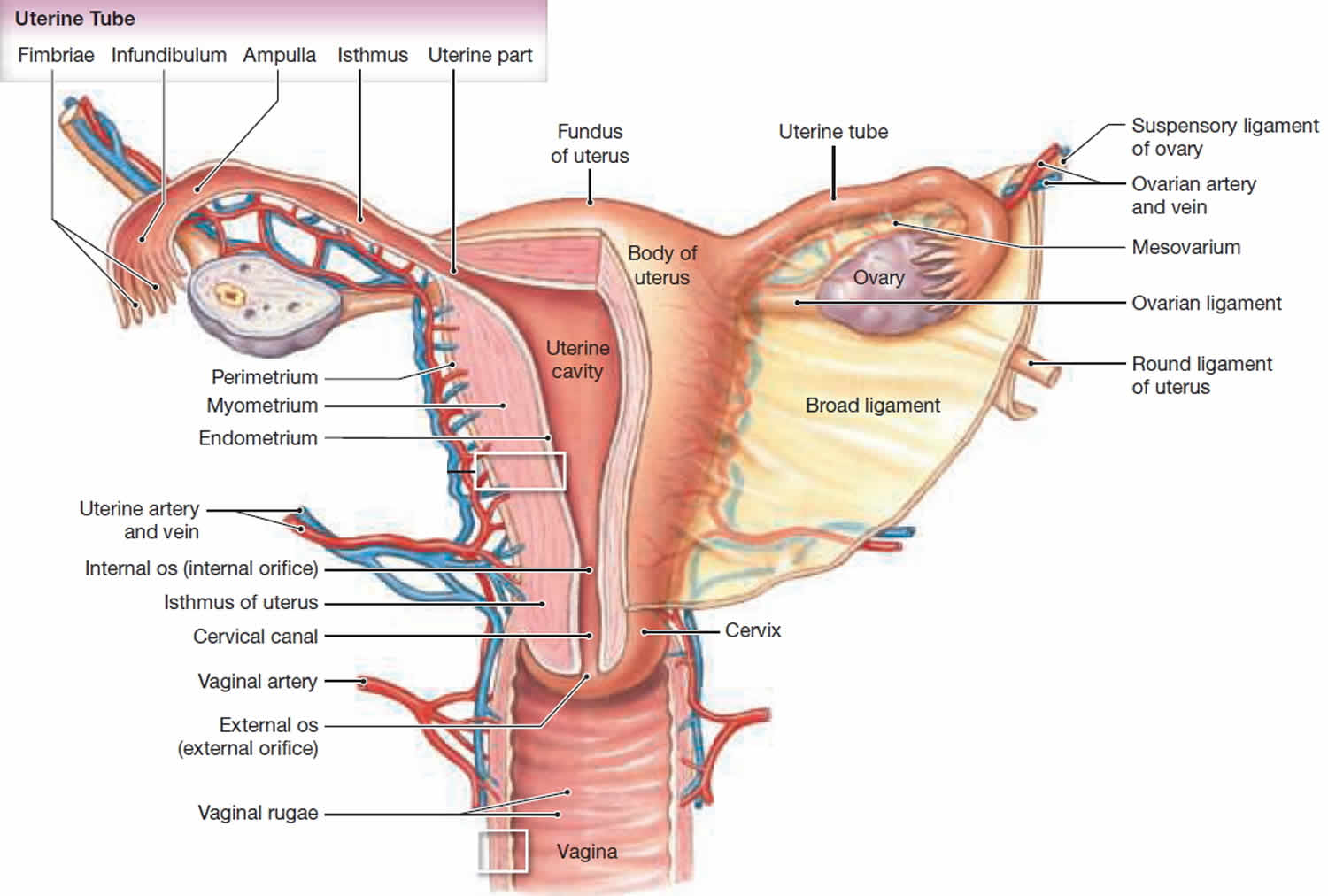
Primary dysmenorrhea occurs in as many as 50% of young women, only in ovulatory cycles, and usually limited to the first 48 or 72 hours of menstruation. Every month the lining of a woman’s womb builds up and is then shed again at the end of the menstrual cycle, when she has her period – unless you are pregnant. To shed the lining during the monthly period, the muscles of the womb tighten (contract) and relax in an irregular rhythm. This helps the tissue lining the womb to detach and flow out of the body, together with blood, through the neck of the womb (cervix) and the vagina. The muscle contractions are sometimes not noticeable or only cause mild discomfort, but they’re also sometimes felt as painful cramps. Period pain might only affect the lower abdomen, or it might be felt in the back or legs too. It can cause nausea, vomiting or diarrhea in some women, as well as headaches or general discomfort. Women who have heavier periods often have more intense pain too.
Secondary dysmenorrhea often first arises after a young woman has already been menstruating for several years. Here, women may also have pain at times of the month other than during menstruation. Secondary dysmenorrhea can be caused by any of a dozen or so disorders such as endometriosis, pelvic inflammatory disease (PID), intrauterine devices (IUDs), irregular cycles or infertility problems, ovarian cysts, adenomyosis, uterine myomas or polyps, intrauterine adhesions or cervical stenosis. Psychological factors are now known not to cause dysmenorrhea, only to add to the reactive component of the pain.
Most of the time, women do not need to see her doctor for menstrual cramps. This may be different if you have severe, lasting pain or pain that is new or different. In these cases, your doctor may want to do a physical exam, pelvic exam, or tests. These can help diagnose or rule out the cause of your pain. An ultrasound test lets your doctor see if you have ovarian cysts. A laparoscopy can check for endometriosis. In this minor surgery, the doctor makes a small cut in your low stomach. Then, they insert a thin tube to look inside your uterus.
Dysmenorrhea key points
- Dysmenorrhea may begin soon after the menarche (girl’s first period), where it often improves with age, or may originate later in life after the onset of an underlying causative condition.
- Dysmenorrhea is very common, and in up to 20% of women it may be severe enough to interfere with daily activities.
- Dysmenorrhea is more likely in women who smoke, and those with an earlier age at menarche or longer duration of menstruation.
- Nonsteroidal anti-inflammatory drugs (NSAIDs) (e.g., ibuprofen [Advil, Motrin IB, others] or naproxen sodium [Aleve]) reduce moderate to severe pain in women with primary dysmenorrhea compared with placebo, but doctors don’t know whether any one NSAID is superior to the others 2).
- Simple analgesics such as aspirin and paracetamol may reduce pain in the short term, although few studies have been of good quality.
- The herbal remedies toki-shakuyaku-san and Iranian herbal remedy (saffron, celery, and anise) may reduce pain compared with placebo. Doctors don’t know whether Chinese herbal remedies are beneficial compared with placebo, but they found limited evidence that they may be effective compared with other treatments for dysmenorrhea.
- Thiamine and vitamin E may reduce pain compared with placebo in young women with primary dysmenorrhea.
- Combined oral contraceptives may be more effective at reducing pain in women with primary dysmenorrhea compared with placebo; however, few trials have been of good quality.
- Topical heat (about 39 °C) may be as effective as ibuprofen and more effective than paracetamol at reducing pain.
- High-frequency transcutaneous electrical nerve stimulation (TENS) may reduce pain compared with sham TENS, but seems to be less effective than ibuprofen.
- Acupressure may be more effective than sham acupressure or no treatment at relieving dysmenorrhea.
- Spinal manipulation may be no more effective than placebo at reducing pain after 1 month in women with primary dysmenorrhea.
- Relaxation may be better than no treatment at relieving dysmenorrhea.
- Scientists don’t know whether acupuncture, fish oil, vitamin B12 , magnets, or intrauterine progestogens reduce dysmenorrhea.
- Surgical interruption of pelvic nerve pathways is not beneficial in treating dysmenorrhea, and may be associated with adverse effects including constipation.
See your doctor if:
- Menstrual cramps disrupt your life every month
- Your symptoms progressively worsen
- You just started having severe menstrual cramps after age 25
- You have pain at times other than the first couple days of your period
- You have a fever and pelvic pain
- Sudden or severe pain, especially if your period is more than 1 week late and you have been sexually active.
- You have abnormal vaginal discharge or bleeding
- Increased or foul-smelling vaginal discharge.
- Your pain that doesn’t go away when you take medicine to relieve it.
Also see your doctor if:
- Treatments do not relieve your pain after 3 months.
- You have pain and had an intrauterine device (IUD) placed more than 3 months ago.
- You pass blood clots or have other symptoms with the pain.
- Your pain occurs at times other than menstruation, begins more than 5 days before your period, or continues after your period is over.
Dysmenorrhea causes
Doctors distinguish between two types of period pain, called primary and secondary dysmenorrhea, depending on the cause.
Painful menstrual periods fall into two groups, depending on the cause:
- Primary dysmenorrhea: Primary dysmenorrhea is menstrual pain that occurs around the time that menstrual periods first begin in otherwise healthy young women. In most cases, this pain is not related to a specific problem with the uterus or other pelvic organs. Increased activity of the hormone prostaglandin, which is produced in the uterus, is thought to play a role in this condition.
- Secondary dysmenorrhea: Period pain that is caused by something other than the muscle contractions is called secondary dysmenorrhea. Benign (non-cancerous) growths in the womb, such as fibroids or polyps, are often responsible for secondary dysmenorrhea. Severe period pain may also be caused by endometriosis. In endometriosis, the kind of tissue that lines the womb (endometrium) grows elsewhere in the abdomen too. Sometimes contraceptive coils (IUDs: intrauterine devices) used for birth control can also cause secondary dysmenorrhea.
During your menstrual period, your uterus contracts to help expel its lining. Hormone like substances (prostaglandins) involved in pain and inflammation trigger the uterine muscle contractions. Higher levels of prostaglandins are associated with more-severe menstrual cramps.
Primary dysmenorrhea
Primary dysmenorrhea is the most common kind of period pain. Primary dysmenorrhea is where the period pain is caused by the womb muscle contractions alone. Hormone-like substances called prostaglandins play an important role here. Prostaglandins influence the perception of pain and cause the muscles in your womb to tighten, helping to shed the lining of your womb. Primary dysmenorrhea is more common in women under the age of 30 and women with heavy periods. It can run in families, and stress can play a role too.
The pain can start a day or two before your period. It normally lasts for a few days, though in some women it can last longer.
You usually first start having period pain when you are younger, just after you begin getting periods. Often, as you get older, you have less pain. The pain may also get better after you have given birth.
Secondary dysmenorrhea
Secondary dysmenorrhea is menstrual pain that develops later in women who have had normal periods. Secondary dysmenorrhea is caused by conditions that affect your uterus or other reproductive organs, such as endometriosis and uterine fibroids. This kind of pain often gets worse over time. It may begin before your period starts, and continue after your period ends.
Secondary dysmenorrheais often related to problems in the uterus or other pelvic organs, such as:
- Endometriosis. The tissue that lines your uterus becomes implanted outside your uterus, most commonly on your fallopian tubes, ovaries or the tissue lining your pelvis.
- Uterine fibroids. These noncancerous growths in the wall of the uterus can cause pain.
- Adenomyosis. The tissue that lines your uterus begins to grow into the muscular walls of the uterus.
- Pelvic inflammatory disease (PID). This infection of the female reproductive organs is usually caused by sexually transmitted bacteria.
- Cervical stenosis. In some women, the opening of the cervix is small enough to impede menstrual flow, causing a painful increase of pressure within the uterus.
- Intrauterine device (IUD) made of copper
- Premenstrual syndrome (PMS). Besides dysmenorrhea, patients with premenstrual dysphoric disorder (formerly premenstrual syndrome) may have bloating, body aches, migraine headaches, breast tenderness, and emotional complaints. The effects of these symptoms are occasionally debilitating. Aside from possible vaginal brownish discharge or bleeding, pelvic examination findings are normal. It is the emergency physician’s responsibility to ensure adequate analgesia and appropriate follow-up with a gynecologist.
- Sexually transmitted infection (STD or STI)
- Stress and anxiety.
Risk factors for menstrual cramps
You might be at risk of menstrual cramps if:
- You’re younger than age 30
- You started puberty early, at age 11 or younger
- Early age at menarche (< 12 years)
- You bleed heavily during periods (menorrhagia)
- You have irregular menstrual bleeding (metrorrhagia)
- You have a family history of menstrual cramps (dysmenorrhea)
- You smoke
- Nulliparity (woman who has never borne a child)
- Obesity
Can dysmenorrhea be prevented or avoided?
Menstrual cramps and pain cannot be prevented or avoided.
Various measures have been used to manage dysmenorrhea in the outpatient setting, including the following:
- Lifestyle modification seems to be helpful
- Smoking cessation should be encouraged, in that smoking may be a risk factor for dysmenorrhea 3)
- Exercise has been shown to alleviate symptoms of dysmenorrhea, though the mechanism is not well understood 4)
A Cochrane review of 5 randomized controlled trials showed that certain behavioral interventions may be effective at treating primary and secondary dysmenorrhea 5).
Dysmenorrhea symptoms
Menstrual cramps can feel like a dull ache or a shooting pain. They most often occur in your low stomach. You may also feel them in your low back, hips, or thighs. The pain may start before your period or when your period begins. Menstrual cramps last about 1 to 3 days. The pain may be bad enough to keep you from normal activities.
Primary dysmenorrhea should be distinguished from secondary dysmenorrhea on the basis of clinical features. Clinical features of primary dysmenorrhea include the following 6):
- Onset shortly after menarche (typically within 6 months)
- Usual duration of 48-72 hours (often starting several hours before or just after the menstrual flow)
- Cramping or laborlike pain
- Background of constant lower abdominal pain, radiating to the back or the anterior or medial thigh
- Often unremarkable pelvic examination findings (including rectal)
Associated general symptoms, such as malaise, fatigue (85%), nausea and vomiting (89%), diarrhea (60%), lower backache (60%), and headache (45%), may be present with primary dysmenorrhea. Dizziness, nervousness, and even collapse are also associated with dysmenorrhea.
A different pattern of pain is observed with secondary dysmenorrhea that is not limited to the onset of menses; this is usually associated with abdominal bloating, pelvic heaviness, and back pain. Typically, the pain progressively increases during the luteal phase until it peaks around the onset of menstruation.
The following may indicate secondary dysmenorrhea 7):
- Dysmenorrhea beginning in the 20s or 30s, after relatively painless menstrual cycles in the past
- Heavy menstrual flow or irregular bleeding
- Dysmenorrhea occurring during the first or second cycles after menarche, which may indicate congenital outflow obstruction
- Pelvic abnormality with physical examination (consider endometriosis, pelvic inflammatory disease [PID], pelvic adhesions, and adenomyosis)
- Little or no response to nonsteroidal anti-inflammatory drugs (NSAIDs) or oral contraceptives
- Infertility
- Dyspareunia
- Vaginal discharge
Dysmenorrhea complications
Menstrual cramps don’t cause other medical complications, but they can interfere with school, work and social activities.
Certain conditions associated with menstrual cramps can have complications, though. For example, endometriosis can cause fertility problems. Pelvic inflammatory disease can scar your fallopian tubes, increasing the risk of a fertilized egg implanting outside of your uterus (ectopic pregnancy).
Dysmenorrhea diagnosis
Your doctor will review your medical history and perform a physical exam, including a pelvic exam. During the pelvic exam, your doctor will check for abnormalities in your reproductive organs and look for signs of infection.
If your doctor suspects that a disorder is causing your menstrual cramps, he or she may recommend other tests, such as:
- Ultrasound. This test uses sound waves to create an image of your uterus, cervix, fallopian tubes and ovaries.
- Other imaging tests. A CT scan or MRI scan provides more detail than an ultrasound and can help your doctor diagnose underlying conditions. CT combines X-ray images taken from many angles to produce cross-sectional images of bones, organs and other soft tissues inside your body. MRI uses radio waves and a powerful magnetic field to produce detailed images of internal structures. Both tests are noninvasive and painless.
- Laparoscopy. Although not usually necessary to diagnosis menstrual cramps, laparoscopy can help detect an underlying condition, such as endometriosis, adhesions, fibroids, ovarian cysts and ectopic pregnancy. During this outpatient surgery, your doctor views your abdominal cavity and reproductive organs by making tiny incisions in your abdomen and inserting a fiber-optic tube with a small camera lens.
Dysmenorrhea treatment
The primary dysmenorrhea pain is due to uterine cramps, hypoxia or ischemia, due to overproduction of prostaglandins, leukotrienes or vasopressin.
Treatment of secondary dysmenorrhea involves correction of the underlying organic cause. Specific measures (medical or surgical) may be required to treat pelvic pathologic conditions (eg, endometriosis) and to ameliorate the associated dysmenorrhea. Periodic use of analgesic agents as adjunctive therapy may be beneficial.
To ease your menstrual cramps, your doctor might recommend:
- Pain relievers. Over-the-counter pain relievers, such as ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve), at regular doses starting the day before you expect your period to begin can help control the pain of cramps. Prescription nonsteroidal anti-inflammatory drugs also are available. Start taking the pain reliever at the beginning of your period, or as soon as you feel symptoms, and continue taking the medicine as directed for two to three days, or until your symptoms are gone.
- Hormonal birth control. Oral birth control pills contain hormones that prevent ovulation and reduce the severity of menstrual cramps. These hormones can also be delivered in several other forms: an injection, a skin patch, an implant placed under the skin of your arm, a flexible ring that you insert into your vagina, or an intrauterine device (IUD).
- Surgery. If your menstrual cramps are caused by a disorder such as endometriosis or fibroids, surgery to correct the problem might help your symptoms. Surgical removal of the uterus also might be an option if other approaches fail to ease your symptoms and if you’re not planning to have children.
Medicine for periods cramps
Non-steroidal anti-inflammatory drugs (NSAIDs) are the competitive inhibitors of cyclooxygenase (COX), the enzyme which mediates the bioconversion of arachidonic acid to inflammatory prostaglandins. The NSAIDs specifically approved by the US Food and Drug Administration (FDA) for treatment of dysmenorrhea are as follows:
- Diclofenac
- Ibuprofen
- Ketoprofen
- Meclofenamate
- Mefenamic acid
- Naproxen
Aspirin may not be as effective as these NSAIDs, and acetaminophen may be a useful adjunct for alleviating only mild menstrual cramping pain 8).
NSAIDs that achieve peak serum concentrations within 30-60 minutes and have a faster onset of action (eg, ibuprofen, naproxen, and meclofenamate) may be preferred. However, individual patient response varies, and patients may need to try several agents before finding one that works. Some NSAIDs (eg, indomethacin) should be avoided, because they have a higher incidence of adverse effects.
Cyclooxygenase [COX]-2 specific inhibitors have also proven effective in relieving menstrual pain. Their selectivity reduces the gastrointestinal symptoms caused by inhibition of the COX-1 receptor. Despite some preliminary data suggesting efficacy in patients with primary dysmenorrhea, COX-2 inhibitors have not been demonstrably superior to conventional NSAIDs 9).
However, these agents may be used in patients who cannot tolerate other NSAIDS or in whom these agents are contraindicated. COX-2–derived prostanoids nonetheless appear to be involved in the pathophysiology of primary dysmenorrhea 10).
Other analgesic agents
In an emergency setting, patients who do not respond to NSAIDs may require treatment with narcotics for pain control. Patients whose symptoms are not relieved by NSAIDs are very likely to have an underlying pelvic condition (eg, endometriosis).
In a study comparing montelukast, a leukotriene-receptor antagonist, with placebo in patients with dysmenorrhea, montelukast was effective in reducing pain 11). Clinicians may consider this agent as an alternative to hormonal therapy or in lieu of NSAIDs.
Simple analgesics, such as aspirin and acetaminophen, may also be useful, especially when NSAIDs are contraindicated.
Oral contraceptives
Oral contraceptives, which block monthly ovulation and may decrease menstrual flow, may also relieve symptoms. An update of a Cochrane review showed some evidence of symptomatic benefit in patients with primary dysmenorrhea, though no specific preparation showed superiority over any other 12).In some patients, oral contraceptives can prevent dysmenorrhea altogether, even though these agents are not approved by the FDA for this indication.
Oral contraceptives may be an appropriate choice for patients who do not wish to conceive. Combination oral contraceptives suppress the hypothalamic-pituitary-ovarian axis, thereby inhibiting ovulation and preventing prostaglandin production in the late luteal phase. This generally reduces the amount of menstrual flow and alleviates primary dysmenorrhea in most patients. Use of oral contraceptives in a manner that reduces the number of menstrual cycles may be beneficial for some patients 13).
Combination oral contraceptives, the levonorgestrel intrauterine device, and depot medroxyprogesterone acetate 14) provide effective pain relief and are associated with reduced menstrual flow. It may be necessary to add an NSAID to the oral contraceptive, especially during the first few cycles after initiation of the oral contraceptive. The ethinyl estradiol dose should generally be less than 50 µg; a monophasic oral contraceptive containing 30 µg is a reasonable choice. To date, studies comparing the efficacy of various oral contraceptive formulations in the management of dysmenorrhea have not been performed.
In a study of women with primary dysmenorrhea, Petraglia et al 15) found that estradiol valerate plus dienogest and ethinyl estradiol plus levonorgestrel were comparably effective in relieving dysmenorrheic pain. Each of the treatments was taken orally by over 200 women daily for three 28-day cycles, with the number of days of pain and the degree of pain being evaluated. Based on the patients’ self-assessments, the investigators determined that pain was reduced by both treatments by approximately the same number of days (by 4.6 days for estradiol valerate plus dienogest, by 4.2 days for ethinyl estradiol plus levonorgestrel).
Lifestyle and home remedies
At-home treatment is available for women who have menstrual cramps. The goal is to relieve symptoms. Over-the-counter (OTC) medicines can reduce pain. These include ibuprofen (brand names: Advil and Motrin) and naproxen (brand name: Aleve). These medicines belong to a group of medications known as non-steroidal anti-inflammatory drugs (NSAIDs). They can relieve period pain by reducing the production of prostaglandins. Start taking it the day before your period is expected to start and continue taking it regularly for the first few days of your period. Although NSAIDs are usually well tolerated, they sometimes have side effects, especially stomach-related problems.
Other medicines are Midol, Pamprin, and Premsyn PMS.
You also can try using heating pads or taking a warm bath. Some evidence suggests that applying warmth, for instance with heat packs, can relieve period pain. A few studies have also suggested that physical activity such as jogging, yoga and exercises can help.
Talk to your doctor if these don’t help. They may suggest a stronger pain reliever. They may want you to try using birth control pills or a birth control shot. These can help make your periods less painful. The birth control pill can relieve period pain because it prevents ovulation. This reduces the production of prostaglandins. It also means that the lining of your womb doesn’t become as thick as usual, and you have a lighter period. The birth control pill can have side effects too, such as headaches and nausea. It also increases the risk of thrombosis.
Other treatments – like acupuncture, dietary supplements or herbal products – haven’t been proven to help. Although these approaches have been tested in a number of studies, the study results were contradictory or the studies weren’t done properly.
The following steps may help you to avoid prescription medicines:
- Get enough sleep and rest
- Exercise regularly. Physical activity, including sex, helps ease menstrual cramps for some women.
- Use heat. Soaking in a hot bath or using a heating pad, hot water bottle or heat patch on your lower abdomen (below your belly button) might ease menstrual cramps. Never fall asleep with the heating pad on.
- Take warm showers or baths.
- Try dietary supplements. A number of studies have indicated that vitamin E, omega-3 fatty acids, vitamin B-1 (thiamin), vitamin B-6, calcium, and magnesium supplements might reduce menstrual cramps.
- Reduce stress. Psychological stress might increase your risk of menstrual cramps and their severity.
- Practice relaxation techniques such as meditation or yoga.
- Lose weight if you are overweight. Get regular, aerobic exercise.
- Do light circular massage with your fingertips around your lower belly area.
- Drink warm beverages.
- Eat light but frequent meals.
- Keep your legs raised while lying down or lie on your side with your knees bent.
Sometimes the pain is so bad that psychological treatment is considered. This may include things like talks with a psychotherapist and learning techniques that can reduce pain (such as relaxation and mindfulness exercises).
If these self-care measures do not work, your health care provider may offer you treatment such as:
- Birth control pills
- Mirena IUD
- Prescription anti-inflammatory medicines
- Prescription pain relievers (including narcotics, for brief periods)
- Antidepressants
- Antibiotics
- Pelvic ultrasound
- Suggest surgery (laparoscopy) to rule out endometriosis or other pelvic disease
Alternative medicine
Most alternative therapies for treating menstrual cramps haven’t been studied enough for experts to recommend them. However, some alternative treatments might help, including:
- Acupuncture. Acupuncture involves inserting extremely thin needles through your skin at strategic points on your body. Some studies have found that acupuncture helps relieve menstrual cramps.
- Transcutaneous electrical nerve stimulation (TENS). A TENS device connects to the skin using adhesive patches with electrodes in them. The electrodes deliver a varying level of electric current to stimulate nerves. TENS might work by raising the threshold for pain signals and stimulating the release of your body’s natural painkillers (endorphins). In studies, TENS was more effective than a placebo in relieving menstrual cramp pain.
- Herbal medicine. Some herbal products, such as pycnogenol, fennel or combination products, might provide some relief from menstrual cramps.
- Acupressure. Like acupuncture, acupressure also involves stimulating certain points on the body, but with gentle pressure on the skin instead of needles. Although research on acupressure and menstrual cramps is limited, it appears that acupressure may be more effective than a placebo in easing menstrual cramps.
Living with dysmenorrhea
Menstrual cramps are painful but can be managed with treatment. Primary dysmenorrhea can be treated with oral contraceptives if the women wishes to take pills for contraception and they are not contraindicated, or with Nonsteroidal anti-inflammatory drugs (NSAIDs) for the full 72 hours after pain begins. Calcium channel-blockers are also used on a research basis; transcutaneous electrical nerve stimulation (TENS) is sometimes effective. If these treatments are not effective, investigation for causes of secondary dysmenorrhea is indicated, preferably using laparoscopy.
Dysmenorrhea prognosis
With the use of NSAIDs, the prognosis for primary dysmenorrhea is excellent. The prognosis for secondary dysmenorrhea varies, depending on the underlying disease process. If a diagnosis of secondary dysmenorrhea is missed, the underlying pathology may lead to increased morbidity, including difficulty conceiving 16).
Although dysmenorrhea itself is not life-threatening, it can have a profound negative impact on a woman’s day-to-day life. Besides missing work or school, she may be unable to participate in sports or other activities and thus experience additional emotional distress. Some 10% of dysmenorrheal women have severe pain that can be incapacitating. Dysmenorrhea is a public health problem associated with substantial economic loss related to work absences (an estimated 600 million work hours and 2 billion dollars in the United States) 17).
A cross sectional study that included 897 adolescent girls reported that those in the dysmenorrhea group had significantly higher depression, aggression, insomnia, daytime sleepiness and sleep apnea scores compared to the control and the premenstrual syndrome groups 18).
References [ + ]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}