
Contents
Shwachman Diamond syndrome
Shwachman-Diamond syndrome is an inherited condition that affects many parts of the body, particularly the bone marrow, pancreas, and skeletal system. Most cases of Shwachman-Diamond syndrome are caused by mutations in the SBDS gene 1). In cases where no SBDS mutation is found, the cause of Shwachman-Diamond syndrome is unknown. Shwachman-Diamond syndrome is inherited in an autosomal recessive manner. Researchers are not sure how common Shwachman-Diamond syndrome is. Several hundred cases have been reported in scientific studies.
The major function of bone marrow is to produce new blood cells. These include red blood cells, which carry oxygen to the body’s tissues; white blood cells, which fight infection; and platelets, which are blood cell fragments that are necessary for normal blood clotting. In Shwachman-Diamond syndrome, the bone marrow malfunctions and does not make some or all types of white blood cells. A shortage of neutrophils, the most common type of white blood cell, causes a condition called neutropenia. Most people with Shwachman-Diamond syndrome have at least occasional episodes of neutropenia, which makes them more vulnerable to infections such as pneumonia, recurrent ear infections (otitis media), and skin infections. Less commonly, bone marrow abnormalities lead to a shortage of red blood cells (anemia), which causes fatigue and weakness, or a reduction in the amount of platelets (thrombocytopenia), which can result in easy bruising and abnormal bleeding.
People with Shwachman-Diamond syndrome have an increased risk of several serious complications related to their malfunctioning bone marrow. Specifically, they have a higher-than-average chance of developing myelodysplastic syndrome and aplastic anemia, which are disorders that affect blood cell production, and a cancer of blood-forming tissue known as acute myeloid leukemia (AML).
Shwachman-Diamond syndrome also affects the pancreas, which is an organ that plays an essential role in digestion. One of this organ’s main functions is to produce enzymes that help break down and use the nutrients from food. In most infants with Shwachman-Diamond syndrome, the pancreas does not produce enough of these enzymes. This condition is known as pancreatic insufficiency. Infants with pancreatic insufficiency have trouble digesting food and absorbing nutrients that are needed for growth. As a result, they often have fatty, foul-smelling stools (steatorrhea); are slow to grow and gain weight (failure to thrive); and experience malnutrition. Pancreatic insufficiency often improves with age in people with Shwachman-Diamond syndrome.
Skeletal abnormalities are another common feature of Shwachman-Diamond syndrome. Many affected individuals have problems with bone formation and growth, most often affecting the hips and knees. Low bone density is also frequently associated with this condition. Some infants are born with a narrow rib cage and short ribs, which can cause life-threatening problems with breathing. The combination of skeletal abnormalities and slow growth results in short stature in most people with this disorder.
The complications of this condition can affect several other parts of the body, including the liver, heart, endocrine system (which produces hormones), eyes, teeth, and skin. Additionally, studies suggest that Shwachman-Diamond syndrome may be associated with delayed speech and the delayed development of motor skills such as sitting, standing, and walking.
There is no cure for Shwachman-Diamond syndrome. The treatment is directed to the symptoms or signals that the patient has. It is important to have several specialists taking care of the patients, like hematologists, gastroenterologists, geneticists, orthopedics, endocrinologists, immunologists or others, as needed. Treatment may include enzyme and vitamin supplementation, blood and/or platelet transfusion, administration of granulocyte-colony stimulating factor (G-CSF), and/or hematopoietic stem cell transplantation 2).
Shwachman-Diamond syndrome causes
Mutations in the SBDS gene have been identified in about 90 percent of people with the characteristic features of Shwachman-Diamond syndrome. This gene provides instructions for making a protein whose function is unknown, although it is active in cells throughout the body. Researchers suspect that the SBDS protein may play a role in processing RNA (a molecule that is a chemical cousin of DNA). This protein may also be involved in building ribosomes, which are cellular structures that process the cell’s genetic instructions to create proteins. It is unclear how SBDS mutations lead to the major signs and symptoms of Shwachman-Diamond syndrome.
In cases where no SBDS mutation is found, the cause of this disorder is unknown.
Shwachman Diamond syndrome inheritance pattern
Shwachman Diamond syndrome is inherited in an autosomal recessive pattern, which means both copies of the gene in each cell have mutations. The parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition.
It is rare to see any history of autosomal recessive conditions within a family because if someone is a carrier for one of these conditions, they would have to have a child with someone who is also a carrier for the same condition. Autosomal recessive conditions are individually pretty rare, so the chance that you and your partner are carriers for the same recessive genetic condition are likely low. Even if both partners are a carrier for the same condition, there is only a 25% chance that they will both pass down the non-working copy of the gene to the baby, thus causing a genetic condition. This chance is the same with each pregnancy, no matter how many children they have with or without the condition.
- If both partners are carriers of the same abnormal gene, they may pass on either their normal gene or their abnormal gene to their child. This occurs randomly.
- Each child of parents who both carry the same abnormal gene therefore has a 25% (1 in 4) chance of inheriting a abnormal gene from both parents and being affected by the condition.
- This also means that there is a 75% ( 3 in 4) chance that a child will not be affected by the condition. This chance remains the same in every pregnancy and is the same for boys or girls.
- There is also a 50% (2 in 4) chance that the child will inherit just one copy of the abnormal gene from a parent. If this happens, then they will be healthy carriers like their parents.
- Lastly, there is a 25% (1 in 4) chance that the child will inherit both normal copies of the gene. In this case the child will not have the condition, and will not be a carrier.
These possible outcomes occur randomly. The chance remains the same in every pregnancy and is the same for boys and girls.
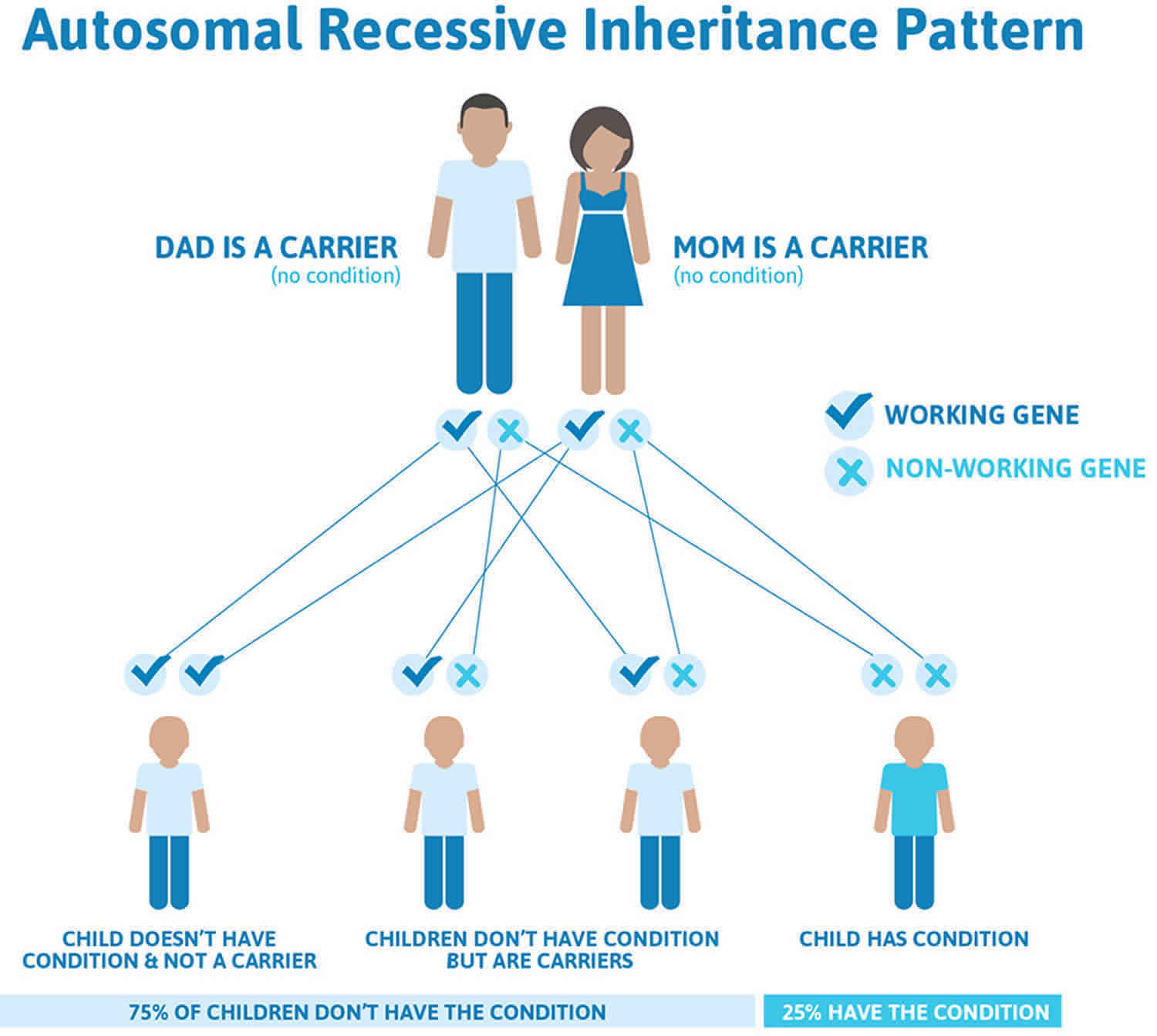
Figure 1 illustrates autosomal recessive inheritance. The example below shows what happens when both dad and mum is a carrier of the abnormal gene, there is only a 25% chance that they will both pass down the abnormal gene to the baby, thus causing a genetic condition.
Figure 1. Shwachman Diamond syndrome autosomal recessive inheritance pattern
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
Can the brother or sister of a carrier of Shwachman-Diamond syndrome also be a carrier?
Each brother or sister of a carrier of Shwachman-Diamond syndrome has a 50% chance of being a carrier (having the gene mutation) and a 50% chance of not being a carrier.
If a relative is known to carry an SBDS gene mutation, other family members can consider genetic testing to determine whether they are carriers. Meeting with a genetics professional can help determine what, if any, genetic testing is appropriate.
Shwachman-Diamond syndrome symptoms
Shwachman-Diamond syndrome is typically characterized by signs of insufficient absorption (malabsorption) of fats and other nutrients due to abnormal development of the pancreas (pancreatic insufficiency) and impaired functioning of the bone marrow, resulting in low levels of circulating blood cells (hematologic abnormalities). Additional characteristic findings may include short stature; abnormal bone development affecting the rib cage and/or bones in the arms and/or legs (metaphyseal dysostosis); recurrent infections; and/or liver dysfunction.
In addition to short stature, skeletal abnormalities in an individual with Shwachman Diamond syndrome may include the following:
- Clinodactyly (curvature of a finger or toe)
- Syndactyly (webbed fingers or toes)
- Supernumerary metatarsals
- Coxa vara deformity
- Genu and cubitus valgus
- Tooth enamel defects (dental dysplasia) 3)
Along with eczema, dermatologic manifestations in patients with Shwachman Diamond syndrome include ichthyosis and petechiae.
As a result of the bone marrow dysfunction, individuals with Shwachman-Diamond syndrome have a higher-than-average chance of developing myelodysplastic syndrome and aplastic anemia, which are disorders that affect blood cell production, and a cancer of blood-forming tissue known as acute myeloid leukemia (AML).
Less frequently reported conditions include cardiac lesions, developmental and intellectual delays, behavior and eating problems, lung disease, renal tubular malfunction, abnormal pulmonary function tests, testicular fibrosis, dental problems, diabetes mellitus and pubertal delays.
Shwachman-Diamond syndrome diagnosis
The diagnosis of Shwachman-Diamond syndrome relies on clinical findings, including pancreatic dysfunction and characteristic hematologic abnormalities. Variation in severity and clinical findings may complicate the ability to establish a definitive diagnosis. Genetic testing may be used to confirm the diagnosis 4).
Genetic testing is available for SBDS gene, the gene known to cause most cases of Shwachman-Diamond syndrome 5). Carrier testing for at-risk relatives and prenatal testing are possible if both disease-causing changes (mutations) in the family are known. In less than 10% of people with Shwachman Diamond syndrome, no mutation in the SBDS gene is identified 6). The exact underlying cause of the condition in these cases is unknown. Genetic testing is not an option for these families.
In addition to a complete history and physical examination, other diagnostic tests may be used to aid in the diagnosis of Shwachman-Diamond syndrome. Blood work may be performed to evaluate the white blood cells, red blood cells, and platelets under a microscope. Blood testing may also evaluate the function of the kidney, liver, and pancreas. Studies such as pancreatic stimulation testing and stool collection may also be performed. A skeletal survey may be done to evaluate the bones of the body. In addition, samples of bone marrow may be taken to examine blood cell lines (red cells, white cells, and platelets), genetic make up of the bone marrow, and the physical architecture of the bone marrow 7).
Evaluations following initial diagnosis
To establish the extent of disease and needs of an individual following the initial diagnosis of Shwachman-Diamond syndrome, current consensus practice typically recommends the following evaluations to assess the status of the pancreas, liver, bone marrow, and skeleton 8).
- Assessment of growth: height, weight in relation to age
- Assessment of nutritional status to determine if supplementation with pancreatic enzymes is necessary and/or effective:
- Measurement of fat-soluble vitamins (vitamin A, 25-OH-vitamin D, and vitamin E) or their related metabolites
- Measurement of prothrombin time (to detect vitamin K deficiency)
- Assessment of serum concentration of the digestive enzyme cationic trypsinogen and, if sufficiency is observed, subsequent confirmation with a 72-hour fecal fat balance study (with discontinuation of enzyme supplementation for at least a 24-hour period)
- Pancreatic imaging by ultrasound
- Complete blood count with white cell differential and platelet count
- Measurement of iron, folate, and B12
- Bone marrow examination with biopsy and cytogenetic studies at initial assessment
- Immunoglobulins and lymphocyte subpopulations
- Skeletal survey with radiographs of at least the hips and lower limbs
- Bone densitometry as clinically indicated
- Assessment of serum aminotransferase levels
- Assessment of developmental milestones (including pubertal development) with neuropsychological evaluation
- Consultation with a clinical geneticist and/or genetic counselor
Shwachman-Diamond syndrome treatment
Patients with Shwachman-Diamond syndrome usually require care from specialists in hematology, gastroenterology, clinical genetics, orthopedics, endocrinology, immunology, dentistry, child development, psychology, and social work as needed 9).
Treatment of Shwachman Diamond syndrome includes:
- Oral pancreatic enzyme replacement with meals in those who are pancreatic insufficient – to help break food down into smaller, more absorbable nutrients.
- Supplementation with fat-soluble vitamins (A, D, E, and K) and a low fat diet is recommended.
- Blood and/or platelet transfusions may be done if the patient is anemic or have low white cell counts in the blood.
- Intravenous antibiotics and granulocyte-colony stimulation factor (G-CSF) to stimulate the bone marrow to make more white blood cells, if there are infections and the white cell blood count are low (500/mm³ or less).
- Hematopoietic stem cell transplantation, which are cells that are isolated from the blood or bone marrow and can renew themselves, in cases of severe pancytopenia (low of all blood cells), myelodysplastic syndrome, or acute myelogenous leukemia (AML).
- Use of medicines to treat cancer (chemotherapy) before doing the hematopoietic stem cell transplantation when the patient have acute myelogenous leukemia (AML).
- Growth hormone has been used to treat children with Shwachman-Diamond syndrome who have growth hormone deficiency.
- Orthopedic surgery – depending on specific skeletal problems
- Blood transfusion – for children at high risk of anemia and/or bleeding
- Ongoing regular dental care
Bone marrow abnormalities are not treated unless there is severe aplasia or myelodysplastic changes, or acute myelogenous leukemia (AML). Some children who have bone abnormalities may need surgery if they have respiratory problems (rib problems resulting in asphyxiating thoracic dystrophy), asymmetric growth or joint problems. It is recommended to have consultation with an endocrinologist if the child is having poor growth and delayed puberty, as well as frequent visits to the dentist to reduce the chances of having mouth wounds (ulcers) and gingivitis 10).
Surveillance
The following are recommended given the intermittent nature of some features of Shwachman Diamond syndrome and the evolution of the phenotype over time 11):
- Complete blood counts with white blood cell differential and platelet counts at least every three to six months, or more frequently if peripheral blood counts are changing or infections are recurrent and debilitating
- Bone marrow examinations every one to three years following the baseline examination, and more frequently if changes in bone marrow function or cellularity are observed
- Assessment of nutritional status every six months and measurement of serum concentration of vitamins to evaluate effectiveness of or need for pancreatic enzyme therapy
- Monitoring for orthopedic complications with x-rays of hips and knees during the most rapid growth stages
- Bone densitometry before puberty, during puberty, and thereafter based on individual findings. Results must be interpreted in the context of stature and pubertal status.
- Developmental assessment every six months from birth to age six years and growth every six months
- Neuropsychological screening in children age 6-8 years, 11-13 years, and 15-17 years
Agents and circumstances to avoid
Prolonged use of cytokine and hematopoietic growth factors (e.g., G-CSF) should be considered with caution in view of their potential contribution to leukemic transformation 12). Some drugs used in standard hematopoietic stem cell transplantation preparative regimens (e.g., cyclophosphamide and busulfan) may not be suitable because of possible cardiac toxicity 13).
Shwachman-Diamond syndrome prognosis
With modern treatment options and ongoing management, most children with Shwachman-Diamond syndrome lead normal lives, although continued medications and regular monitoring through hospital visits are usually required. These are typically annual visits for children without any major problems or more frequently for those with complications.
Children with Shwachman-Diamond syndrome have a small but significant chance of developing blood disorders such as myelodysplastic syndrome or leukemia. Nearly 5 percent of children with the condition will develop leukemia, with the risk rising to 25 percent by adulthood.
In addition, recurring infections, including pneumonia, ear and skin infections, are common. Many children with SDS also have growth problems and vitamin A, D, E and K deficiencies.
References [ + ]





{kind=link}