Contents
Van der Woude syndrome
Van der Woude syndrome is a rare inherited condition that affects the development of the face 1). Many people with Van der Woude syndrome are born with a cleft lip, a cleft palate (an opening in the roof of the mouth), or both. Affected individuals usually have depressions (pits) near the center of the lower lip, which may appear moist due to the presence of salivary and mucous glands in the pits. Small mounds of tissue on the lower lip may also occur. In some cases, people with van der Woude syndrome have missing teeth.
Van der Woude syndrome represents the mild end of the spectrum of disorders known as IRF6-related disorders. At the more severe end of the spectrum is popliteal pterygium syndrome 2).
People with van der Woude syndrome who have cleft lip and/or palate, like other individuals with these facial conditions, have an increased risk of delayed language development, learning disabilities, or other mild cognitive problems. The average IQ of individuals with van der Woude syndrome is not significantly different from that of the general population.
Van der Woude syndrome is believed to occur in 1 in 35,000 to 1 in 100,000 people and without gender predilection, based on data from Europe and Asia 3). Van der Woude syndrome is the most common cause of cleft lip and palate resulting from variations in a single gene, and Van der Woude syndrome accounts for approximately 1 in 50 such cases.
The indication for surgical treatment of congenital lip sinuses is primarily cosmetic, although recurrent inflammation is also considered 4).
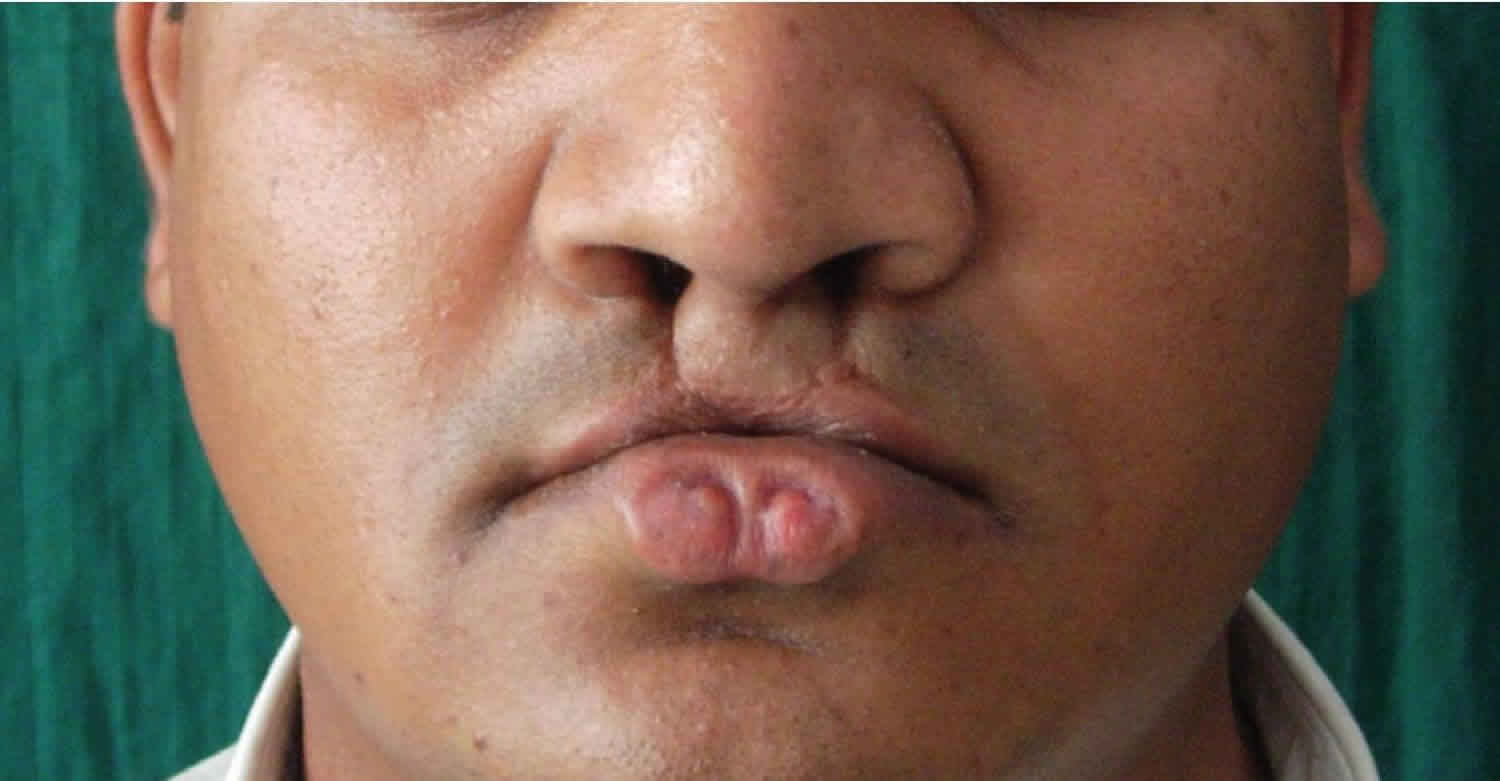
Figure 1. Van der Woude syndrome lip pits

Van der Woude syndrome causes
Mutations in the IRF6 gene cause van der Woude syndrome. The IRF6 gene provides instructions for making a protein that plays an important role in early development. This protein is a transcription factor, which means that it attaches (binds) to specific regions of DNA and helps control the activity of particular genes.
The IRF6 protein is active in cells that give rise to tissues in the head and face. It is also involved in the development of other parts of the body, including the skin and genitals.
Mutations in the IRF6 gene that cause van der Woude syndrome prevent one copy of the gene in each cell from making any functional protein. A shortage of the IRF6 protein affects the development and maturation of tissues in the face, resulting in the signs and symptoms of van der Woude syndrome.
Van der Woude syndrome inheritance pattern
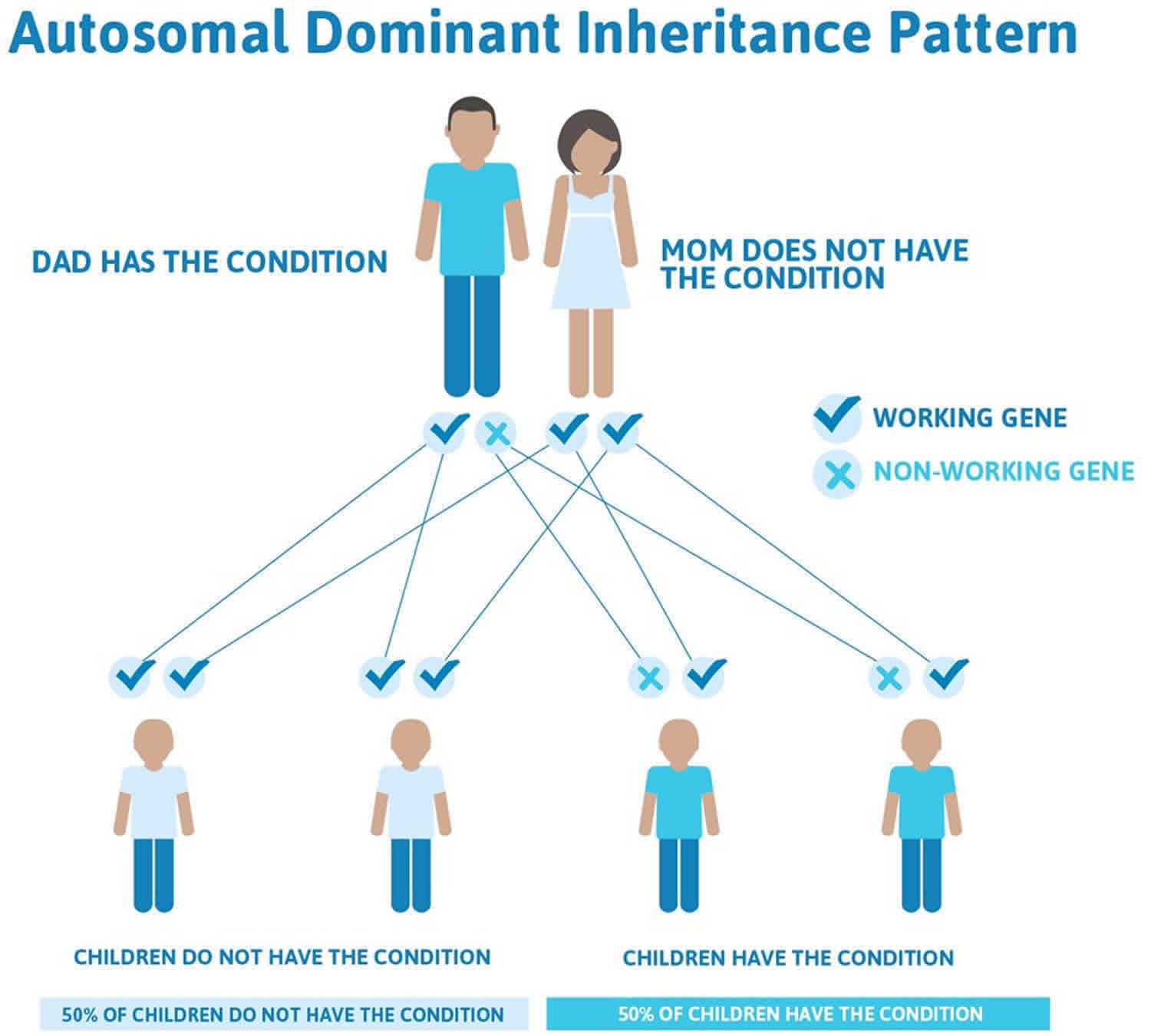
Van der Woude syndrome is inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder. In most cases, an affected person has one parent with the condition. Occasionally, an individual who has a copy of the altered gene does not show any signs or symptoms of the disorder.
Often autosomal dominant conditions can be seen in multiple generations within the family. If one looks back through their family history they notice their mother, grandfather, aunt/uncle, etc., all had the same condition. In cases where the autosomal dominant condition does run in the family, the chance for an affected person to have a child with the same condition is 50% regardless of whether it is a boy or a girl. These possible outcomes occur randomly. The chance remains the same in every pregnancy and is the same for boys and girls.
- When one parent has the abnormal gene, they will pass on either their normal gene or their abnormal gene to their child. Each of their children therefore has a 50% (1 in 2) chance of inheriting the changed gene and being affected by the condition.
- There is also a 50% (1 in 2) chance that a child will inherit the normal copy of the gene. If this happens the child will not be affected by the disorder and cannot pass it on to any of his or her children.
Figure 2 illustrates autosomal dominant inheritance. The example below shows what happens when dad has the condition, but the chances of having a child with the condition would be the same if mom had the condition.
Figure 2. Van der Woude syndrome autosomal dominant inheritance pattern
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
Van der Woude syndrome symptoms
The most prominent and consistent features of van der Woude syndrome are orofacial anomalies caused by an abnormal fusion of the palate and lips at 30-50 days postconception. Many people with Van der Woude syndrome are born with a cleft lip, a cleft palate (an opening in the roof of the mouth), or both. Affected individuals usually have depressions (pits) near the center of the lower lip, which may appear moist due to the presence of salivary and mucous glands in the pits. Small mounds of tissue on the lower lip may also occur. In some cases, people with van der Woude syndrome have missing teeth.
Intelligence and cognitive testing may demonstrate abnormalities; these have been shown in one study to affect males more than females 5). People with van der Woude syndrome like other individuals with these facial conditions, have an increased risk of delayed language development, learning disabilities, or other mild cognitive problems. However, the average IQ of individuals with van der Woude syndrome is not significantly different from that of the general population.
Orofacial manifestations
- van der Woude syndrome is characterized by cleft lip and/or cleft palate and distinctive lower lip pits. This combination is present in approximately 70% of overtly affected individuals but is present in less than one half of those who carry the gene.
- Severity may widely vary, even in members of the same family.
Cleft lip and cleft palate
- The cleft lip and cleft palate may be isolated.
- The severity of these anomalies widely varies and may be unilateral or bilateral.
- Submucous cleft palate is common and may be easily missed during physical examination.
- Hypernasal voice and cleft or bifid uvula may be present. A bifid uvula is also a possible isolated finding in certain individuals with van der Woude syndrome.
Lip pits
- Lower lip pits are fairly distinctive. The pits are usually medial, often (but not always) on the vermilion portion of the lower lip. They tend to be centered on small elevations in infancy but become simple depressions by adulthood; however, the presentation varies. They are usually bilateral but are occasionally median or paramedian or unilateral and are most often found on the left side.
- Visible or expressible saliva may be present in the lip pits because of an association with the accessory salivary glands. Pits may lead to tracts that are surprisingly long, making surgical removal challenging.
- Lip pits may be the only abnormality.
Teeth
Hypodontia may be observed and most commonly presents as missing maxillary or mandibular second premolars or maxillary lateral incisors. This may be the only symptom. An association of van der Woude syndrome and taurodontism (teeth with greatly enlarged pulp chambers) has been reported 6). Dental fusion has also been reported 7).
Other oral manifestations
Although infrequently reported, other symptoms include syngnathia (congenital adhesion of the jaws); narrow, high, arched palate; and ankyloglossia (short glossal frenulum or tongue-tie). A patient without lip pits, oral clefts, or hypodontia but with a heart-shaped mass of the lower lip has been described 8).
Extraoral manifestations
- Extraoral manifestations are rare but include limb anomalies, popliteal webs, and brain abnormalities.
- Accessory nipples, congenital heart defects, and Hirschsprung disease have been reported.
- Extraoral manifestations may be unassociated additional anomalies or infrequently expressed aspects of van der Woude syndrome.
- Signs of van der Woude syndrome have been seen in individuals with popliteal pterygium syndrome, which has also been linked to mutations in the same gene. These 2 entities are believed to be allelic variants of the same condition; some have described these entities as being part of a van der Woude syndrome–popliteal pterygium syndrome spectrum 9).
Clinical features of Van der Woude syndrome
The main clinical feature of Van der Woude syndrome is lip pits and/or sinuses of the lower lip associated with cleft lip and /or palate and occasionally hypodontia (developmental absence of one or more teeth) 10). These pits are depressions of the lower lip that represent blind sinuses or fistulas that may extend deep into the orbicularis muscle 11). Sometimes these pits may communicate with the underlying minor salivary gland thereby discharging saliva. These pits are situated usually on the border between vermilion and mucosa. The depth of these pits is between 5mm to 25mm 12). They usually occur on either side of the midline of the lower lip (Figure 1) and are generally bilateral 13). Clinically these pits appear as asymptomatic with only small depression on the vermilion border or fistula that penetrates into the adjacent minor salivary gland discharging saliva.
Most of the times the lip pits are asymptomatic; the only symptom might be the continuous or intermittent drainage of watery or salivary secretion. In the present review, mucous type of secretion was noted in most reports 14). Rizos and Spyropoulos 15) in their review observed that there are rapid accumulation of mucous secretion on mastication and fear of apprehension, before or during mealtime. It was also reported that the secretion worsened during winter seasons in some patients.
Van der Woude syndrome diagnosis
Van der Woude syndrome should be considered in every child born with a cleft lip and/or palate. A clinical evaluation by a medical geneticist is generally performed to document all relevant clinical findings. In addition, the parents should be examined for isolated lip pits, cleft palate, and hypodontia (missing teeth). To make a clinical diagnosis of Van der Woude syndrome, at least one of the following findings must be present 16):
- Lip pits and cleft lip and/or palate. Lip pits must be paramedian on the lower lip, and can include mounds with a sinus tract leading from a mucous gland of the lip.
- Lip pits alone and a first-degree relative with cleft lip and/or palate
- Cleft lip and/or palate and a first-degree relative with lip pits
Genetic testing for mutations in the IRF6 gene can also be used to diagnose this condition 17). Genetic Testing Registry lists the names of laboratories that are performing genetic testing for Van der Woude syndrome. Please note: Most of the laboratories listed through this resource do not accept direct contact from patients and their families; therefore, if you are interested in learning more, you will need to work with a health care provider or a genetics professional.
If someone with cleft lip and lip pits tests negative for Van der Woude syndrome, could this test be incorrect?
Sequence analysis of the IRF6 gene, which is the genetic test most commonly performed, should be performed first. If no mutation is identified, deletion/duplication analysis can be considered. Sequence analysis detects mutations in approximately 72% of individuals with Van der Woude syndrome. Whole gene deletions of the IRF6 gene have been found in fewer than 2% of families with this condition. In many cases, a clinical diagnosis may be more definitive than diagnosing someone through genetic testing 18).
If a person tests negative for Van der Woude syndrome after having sequence analysis, there are two possible explanations 19):
- The person does not have a mutation in the IRF6 gene and does not have Van der Woude syndrome
- The person has a mutation that cannot be detected by sequence analysis but may still have Van der Woude syndrome
- The person has a mutation in a different gene that is causing clinical features similar to Van der Woude syndrome
Van der Woude syndrome treatment
Examination and genetic counseling by a pediatric geneticist (dysmorphologist) is suggested for families that may be affected by van der Woude syndrome. This should include an examination of as many potentially affected family members as possible. Genetic counseling is recommended.
Surgical repair of cleft lip and cleft palate or other anomalies may be required. Indications for surgical intervention of congenital lip sinus are treatment of the associated cosmetic deformity and recurrent inflammation 20).
Reconstruction of the lower lip may involve dermal allograft reconstruction 21).
Even in less severely affected individuals, surgical excision of lip pits is often performed, either to alleviate discomfort or for cosmetic reasons (eg, improving the appearance of lip pits or reducing mucous discharge) 22). Surgical removal of salivary tracts associated with lip pits may be challenging because they may be quite long, extending into other oral structures 23). Recurrent mucocoele formation is common complication noted following excision
Infectious complications of cleft repairs are reportedly more common in patients with van der Woude syndrome than with other children undergoing similar surgery 24).
References [ + ]





{kind=link}