
Contents
- Translocation down syndrome
- What is chromosomal translocation?
- What is balanced translocation?
- Do people with balanced translocation have signs of Down syndrome?
- How does translocation Down syndrome occur?
- Is translocation Down syndrome inherited?
- Could I have another baby with Down syndrome?
- What is the chance of having another child with translocation Down syndrome?
- Is age a factor in translocation Down syndrome?
- What causes translocation Down syndrome?
- Translocation down syndrome symptoms
- How is translocation Down syndrome diagnosed?
- What is the treatment for translocation Down syndrome?
Translocation down syndrome
Translocation Down syndrome refers to the type of Down syndrome (trisomy 21) that occurs when a portion of chromosome 21 becomes attached (translocated) onto another chromosome, before or at conception. In translocation Down syndrome, there are still three chromosome 21 (trisomy 21), just like there are in regular Down syndrome, but one of the chromosome 21 is attached to another chromosome, instead of being separate. The extra copy of the chromosome 21 is what causes the health problems that are associated with Down syndrome. Translocation Down syndrome children have the usual two copies of chromosome 21, but they also have additional genetic material from chromosome 21 attached to another chromosome.
People with translocation Down syndrome still share the same health issues and learning problems with people with other types of Down syndrome. All people with Down syndrome have some learning problems. The specific location of extra genes generally does not help doctors predict how a child will develop.
Without doing a blood test, it is not possible to tell the difference between people with translocation Down syndrome and people with other types of Down Syndrome.
About 3 – 4% of people with Down syndrome (trisomy 21) have translocation Down syndrome. Translocation Down syndrome usually arises when the small arms (p arm) of chromosome 21 and another chromosome break, and the two remaining long arms (q arms) join together at their exposed ends. This process of chromosomes breaking and rejoining to other chromosomes is known as translocation (because the chromosome material has transferred its location).
In translocation Down syndrome, the extra chromosome 21 may be attached to the chromosome 14 or to other chromosome numbers like 13, 15, or 22. In some cases, two chromosome 21 can be attached to each other.
Whenever a translocation is found in a child, the parents’ chromosomes are studied to determine whether the translocation was inherited or not. If one parent has the translocation chromosome, then the doctor knows the baby inherited the translocation from that parent. When a person has a rearrangement of chromosome material, with no extra or missing chromosome material, he or she is said to have a “balanced translocation” or be a “balanced translocation carrier.”
Parents with balanced translocations may have fertility problems (trouble becoming pregnant), miscarriages, or have an increased chance of having a child with health problems. Although the parent can donate the proper amount of genetic material (23 chromosomes) to a pregnancy, he or she also has a risk of donating too much or too little genetic material to a pregnancy. This is not something the parent can control or predict. The chance depends on the type of chromosome rearrangement and which chromosomes are involved.
There is another important factor to remember when a parent is found to have a translocation. The parents’ relatives (brothers, sisters) may also have inherited the translocation and, therefore, may have the same risks for problems with a pregnancy. For these reasons, it is recommended that people with chromosome rearrangements share this information with their relatives so that they can have the option of having their chromosomes studied.
Genetic counselling should always be available to families with a child with Down’s syndrome. Even if parents do not intend to have more children, knowing that one of them is a carrier can be important for all their children or other relatives. Relatives of a person who carries a translocation have an increased chance of being translocation carriers.
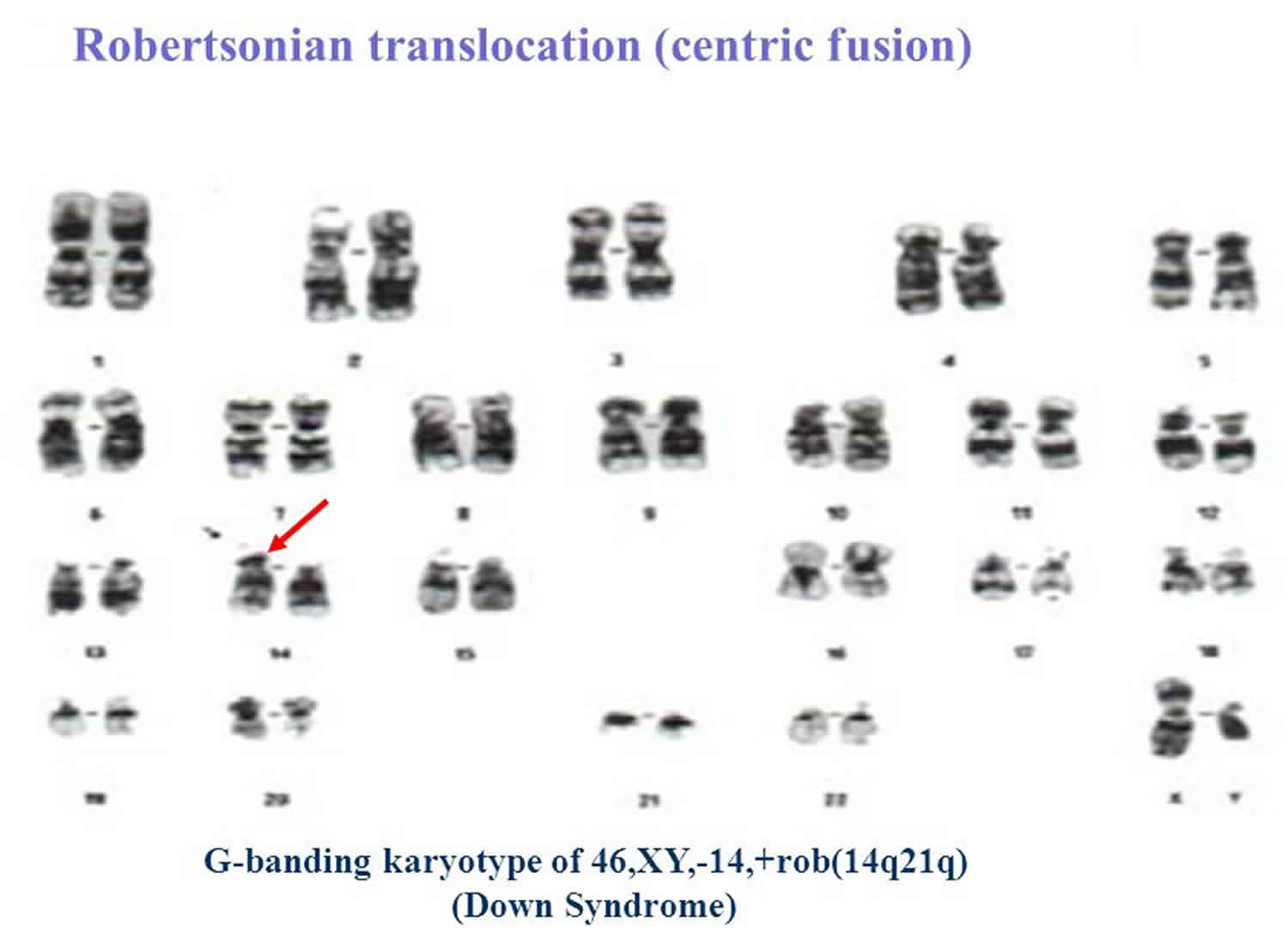
Figure 1. Translocation Down syndrome karyotype
What is chromosomal translocation?
Chromosomal translocation refers to exchange of chromosomal segments between chromosomes. Translocations are the most common type of structural chromosomal abnormalities seen in the general population, having a frequency of about 1/1000 live births 1). Two types of chromosomal translocations are described: Robertsonian translocations and reciprocal translocations 2).
In Robertsonian translocations, the breakpoints commonly occur in the short arms of two acrocentric chromosomes (homologous or nonhomologous) with subsequent fusion and formation of dicentric chromosomes 3). It is reported that either the inactivation of one centromere or the close proximity of the two functional centromeres in these dicentric chromosomes allows them to remain stable 4). Less frequent forms of Robertsonian translocations may be caused by breakage and fusion of centromeres (centric fusion) or from breakage and fusion of one short arm and one long arm of acrocentric chromosomes, resulting in monocentric rearrangements 5). In Robertsonian translocations, the loss of gene-poor short arms of the two acrocentric chromosomes usually does not produce any phenotypic effects. Most of these individuals remain undetected until they attempt to reproduce.
Reciprocal translocations result from breakage of two nonhomologous chromosomes, with at least one of them being a nonacrocentric chromosome, and interchange of chromosomal fragments between them. Consequently, two derivative chromosomes are formed with no loss or gain of genetic material. Unless one or both of the chromosomal breakpoints involve an important functional gene, these balanced chromosomal rearrangements would not produce a significant phenotypic effect either. However, the carriers of both Robertsonian and reciprocal translocations commonly present with reproductive problems, due to unbalanced chromosomal segregation in meiosis, which cause significant chromosomal imbalances (i.e., disomies and nullisomies) in their gametes with subsequent partial aneuploidies in the conceptuses. This can lead to infertility, recurrent miscarriages, or offspring with congenital anomalies due to the unbalanced translocations.
Although all human chromosomes are theoretically susceptible to chromosomal breakage leading to translocations, the frequency of chromosomal translocations shows a nonrandom distribution. Translocations between acrocentric chromosomes 13 and 14 and rob(13q14q) constitute the majority of balanced Robertsonian translocations, with Robertsonian translocations between chromosomes 21 and 14 rob(14q21q) being the second most common type 6). In a Sri Lankan study, Robertsonian translocations between chromosomes 21 and 14 or rob(14q21q) and chromosomes 21 and 21 or rob(21q21q) were commonly observed among children with Down syndrome were more frequent than rob(13q14q) 7). It was suggested that the presence of homologous pericentric regions in chromosomes 13, 14, and 21 contributes to the higher incidence of translocations between these chromosomes 8). Among the balanced reciprocal translocations, translocations involving chromosomes 11 and 22 are commonly described in the scientific literature 9). In a study of 269 balanced translocations among patients with recurrent miscarriages, there was a surplus of chromosomes 6, 7, and 22 in reciprocal translocations 10). Another study with similar design showed an excess of chromosome 7 and 4 in reciprocal translocations 11).
Unbalanced Robertsonian translocations involving chromosome 21 are by far the commonest type of structural abnormalities giving rise to translocation Down syndrome. Other types of homologous or heterologous Robertsonian translocations are comparatively rare 12). A large number of case reports describing children or fetuses with congenital malformations, dysmorphic features, impaired growth, and/or development due to unbalanced reciprocal translocations involving different chromosomes have been reported in the scientific literature. The phenotypic features observed in these cases were attributed to partial monosomy and/or partial trisomy of different chromosomal segments that frequently occurred due to unbalanced chromosomal segregation during meiosis in a parent who is a carrier of a balanced reciprocal translocation.
It is also known that chromosomal translocations are one of the commonest types of inherited chromosomal abnormalities leading to recurrent pregnancy loss 13). Cytogenetic studies on male infertility have also showed a higher frequency of chromosomal translocations among infertile men than in the general population 14). It has been reported that the presence of a chromosomal translocation causes partial or complete spermatogenic arrest, with consequential oligospermia or azoospermia. In contrast, in female carriers of these chromosomal translocations, oogenesis is known to progress without an arrest in meiosis, resulting in the production of abnormal oocytes with unbalanced chromosomal constitution and subsequent partial aneuploidies in the conceptus 15).
What is balanced translocation?
If the extra copy of chromosome 21 is inherited from a parent in the egg or sperm, it means that the parents “carry” this type of Down syndrome. These parents are said to have a “balanced translocation.” Balanced translocation happens when the correct amount of genetic material is present in the wrong location.
Do people with balanced translocation have signs of Down syndrome?
People with balanced translocations do not have any features of Down syndrome. However, it is possible that they may have trouble getting pregnant.
Even though carriers have the right amount of genes, the egg or sperm may have either too much or too few genes. This may cause an unexpected miscarriage.
How does translocation Down syndrome occur?
In two-thirds of people with Down syndrome due to a translocation, the translocation was an isolated event during the formation of the individual egg or sperm involved in their conception. As with regular trisomy 21, there is no known reason why this occurs. It cannot be predicted and it is not a result of anything the parents or other family members have done.
Because it is a new event, this is sometimes called a de novo translocation.
The egg or sperm contains the usual number of chromosomes (i.e. 23) but these include the translocated one. Thus there is one free, whole chromosome 21 and most of a second chromosome 21 attached to another chromosome. If this egg or sperm containing 23 chromosomes (+ translocated part) fuses with an ordinary sperm or egg, the fertilised egg, fetus and baby will have 46 single chromosomes, but one of the chromosomes will have an extra copy of most of the chromosome 21 material attached to it. The translocated chromosome acts like a single chromosome in cell division, and hence all the cells produced from this first cell will contain the extra chromosome 21 portion. This baby will therefore have Down’s syndrome.
In the other one third of people with the translocation type of Down’s syndrome, the translocation is inherited from one of the parents. This parent has two whole number 21 chromosomes in each cell but one of them is attached to another chromosome. As there is no loss or gain of any genetic material this is known as a balanced translocation and the parent is a carrier of the translocation. It is important to realise that because such parents have the usual amount of genetic material, they have no traces of the syndrome themselves and never will have. They cannot be expected to know they are carriers, as the only way of knowing is to study their chromosomes.
When people who carry a translocation produce an egg or sperm, it is possible for them to pass on both the translocated chromosome and the free chromosome 21 in the egg or sperm. This will result in a fertilised egg with two free 21 chromosomes and a translocated chromosome. The baby will therefore have Down’s syndrome.
As 4% of people with Down’s syndrome have the translocation type, and one third of this group have inherited it, only about 1% of people with Down’s syndrome have inherited the condition.
Is translocation Down syndrome inherited?
Yes, translocation Down syndrome can be inherited. An unaffected person can carry a rearrangement of genetic material between chromosome 21 and another chromosome. This rearrangement is called a balanced translocation because there is no extra material from chromosome 21. Although they do not have signs of Down syndrome, people who carry this type of balanced translocation are at an increased risk of having children with the condition.
Could I have another baby with Down syndrome?
Yes. Translocation Down syndrome is the only type of Down Syndrome that can be passed down from a parent who does not have features of Down syndrome.
- If a parent has balanced translocation, there is an up to 15% chance of having another child with Down syndrome.
- A genetic counselor or doctor who is a Down Syndrome expert would be happy to discuss this with you before any future pregnancies.
- These counselors or doctors can also discuss which other family members have a chance of carrying the balanced translocation, such as brothers or sisters.
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
What is the chance of having another child with translocation Down syndrome?
The recurrence risk depends on the type of translocation. When neither of the parents is a carrier, the translocation was an isolated event with only a small chance of its happening again (geneticists quote less than 1%). In most cases, the recurrence risk for de novo translocations is similar to that of the general population but may be slightly higher in some situations; it is estimated to be 2-3% 16).
Translocation carriers can have children who are carriers, children whose chromosomes show no rearrangement at all, or children with Down syndrome. For translocations involving chromosomes 21 and any other chromosome, the chance of another child with Down syndrome being born is about one in six if the mother is the carrier and about one in twenty if the father is the carrier. A few people are carriers for a translocation between two chromosomes 21; in these people, who are quite ordinary themselves, the only possible outcome is a child with Down’s syndrome.
The theoretic recurrence risk for a Robertsonian carrier parent to have a liveborn offspring with Down syndrome is 1 in 3. However, only 10-15% of the progeny of carrier mothers and only 2-3% of the progeny of carrier fathers have Down syndrome. The reason for this difference is not clear. In a carrier parent with a 21q21q translocation or isochromosome, the recurrence risk is 100%.
In any trisomy 21 patient with a translocation, karyotype testing must be recommended to both parents to look for a translocation. If a translocation is found in one of the parents, the recurrence risk is significantly higher, and further genetic counseling is crucial.
Is age a factor in translocation Down syndrome?
No. unlike regular trisomy 21, translocation Down syndrome occurs equally frequently whatever the age of the parents.
What causes translocation Down syndrome?
Translocation Down syndrome can happen one of two ways:
- It can be caused by extra genes in the egg or sperm of one of the parents.
- It can happen by chance.
Translocation down syndrome symptoms
People with translocation Down syndrome still have an extra copy of a large part of chromosome 21. Their clinical features or ability levels of translocation Down syndrome are no different from those in a child with regular trisomy 21. The only way of knowing what type of Down syndrome a person has, is by taking a blood sample and looking at the chromosomes.
A very few children with translocation have partial trisomy 21 – where only a part of chromosome 21 is present in 3 copies. These children may have fewer characteristics of Down syndrome. Like the more usual type of translocation described above, this type may arise de novo, or a parent may carry it.
As one third of people with translocation Down syndrome have inherited the condition, their parents have a high chance of having another affected child and may wish to know whether this is so. To identify these parents, chromosome tests are done on all new babies with Down syndrome. Blood samples can then be taken from parents of babies with translocations, to find out whether one of the parents carries the translocation.
Down syndrome symptoms
Each person with Down syndrome is an individual — intellectual and developmental problems may be mild, moderate or severe. Some people are healthy while others have significant health problems such as serious heart defects.
Children and adults with Down syndrome have distinct facial features. Though not all people with Down syndrome have the same features, some of the more common features include:
- Flattened face
- Small head
- Short neck
- Protruding tongue
- Upward slanting eye lids (palpebral fissures)
- Unusually shaped or small ears
- Poor muscle tone
- Broad, short hands with a single crease in the palm
- Relatively short fingers and small hands and feet
- Excessive flexibility
- Tiny white spots on the colored part (iris) of the eye called Brushfield’s spots
- Short height
Infants with Down syndrome may be average size, but typically they grow slowly and remain shorter than other children the same age.
Intellectual disabilities
Most children with Down syndrome have mild to moderate cognitive impairment. Language is delayed, and both short and long-term memory is affected.
Down syndrome complications
People with Down syndrome can have a variety of complications, some of which become more prominent as they get older. These complications can include:
- Heart defects. About half the children with Down syndrome are born with some type of congenital heart defect. These heart problems can be life-threatening and may require surgery in early infancy.
- Gastrointestinal defects. Gastrointestinal abnormalities occur in some children with Down syndrome and may include abnormalities of the intestines, esophagus, trachea and anus. The risk of developing digestive problems, such as gastrointestinal blockage, heartburn (gastroesophageal reflux) or celiac disease, may be increased.
- Immune disorders. Because of abnormalities in their immune systems, people with Down syndrome are at increased risk of developing autoimmune disorders, some forms of cancer, and infectious diseases, such as pneumonia.
- Sleep apnea. Because of soft tissue and skeletal changes that lead to the obstruction of their airways, children and adults with Down syndrome are at greater risk of obstructive sleep apnea.
- Obesity. People with Down syndrome have a greater tendency to be obese compared with the general population.
- Spinal problems. Some people with Down syndrome may have a misalignment of the top two vertebrae in the neck (atlantoaxial instability). This condition puts them at risk of serious injury to the spinal cord from overextension of the neck.
- Leukemia. Young children with Down syndrome have an increased risk of leukemia.
- Dementia. People with Down syndrome have a greatly increased risk of dementia — signs and symptoms may begin around age 50. Having Down syndrome also increases the risk of developing Alzheimer’s disease.
- Other problems. Down syndrome may also be associated with other health conditions, including endocrine problems, dental problems, seizures, ear infections, and hearing and vision problems.
For people with Down syndrome, getting routine medical care and treating issues when needed can help with maintaining a healthy lifestyle.
Down syndrome life expectancy
Life spans have increased dramatically for people with Down syndrome. Today, someone with Down syndrome can expect to live more than 60 years, depending on the severity of health problems.
How is translocation Down syndrome diagnosed?
Translocation Down syndrome can only be diagnosed with a blood test, because it is not possible to tell the difference between people with translocation Down syndrome and people with other types of Down syndrome.
When Down syndrome is suspected in a person, a genetic test called a chromosome analysis is performed on a blood or skin sample to look for an extra chromosome 21 (trisomy 21). Trisomy 21 means that each cell in the body has three copies of chromosome 21 instead of the usual two copies.
A small number of individuals have Down syndrome because part of chromosome 21 becomes attached (translocated) to another chromosome before or at the time of conception. These individuals have two copies of chromosome 21, and additional material from chromosome 21 that is attached to another chromosome. The chromosomes of parents of a child with Down Syndrome caused by a translocation are studied to see whether the translocation was inherited.
What is the treatment for translocation Down syndrome?
Treatment for Down syndrome is based on the person’s physical problems and intellectual challenges. Many babies who have Down syndrome do not have good muscle tone, which makes it harder for them to roll over and walk. Physical therapy can help with these problems.
About 40 – 60 percent of babies born with Down syndrome have a heart defect. Therefore, all newborns with Down syndrome have their heart checked with an electrocardiogram and an echocardiogram. When there is a heart defect present in an infant with Down syndrome, the infant is referred to a pediatric cardiologist for medical management or to a pediatric cardiac surgeon for early surgical repair.
Some infants with Down syndrome have difficulties with swallowing or they may have blockages in their bowels. Surgery can be performed to correct these problems. Once corrected, they usually cause no further health issues.
Children with Down syndrome may have frequent colds and sinus and ear infections. These are treated early and aggressively to prevent hearing loss and chronic infections.
Low thyroid levels are more common in infants who have Down syndrome. It is recommended that thyroid level testing be performed at least yearly.
Some infants with Down syndrome have eye problems such as cataracts (cloudy lenses) or crossed eyes (strabismus). Surgery can help with these problems.
Sucking problems related to low muscle tone or heart problems may make breast feeding difficult initially. Occupational therapists, speech therapists, breast feeding consultants and support groups usually have specific resources for the mothers of infants with Down syndrome.
Intelligence in individuals with Down syndrome ranges from low normal to very slow to learn. At birth it is not possible to tell the level of intelligence a baby with Down syndrome will have. All areas of development including motor skills, language, intellectual abilities, and social and adaptive skills are followed closely in children with Down syndrome. Early referral, beginning at birth, to an early intervention program will help enhance development. Preschool programs for children with Down syndrome include physical, occupational, speech and educational therapies.
Many adults with Down syndrome have jobs and live independently.
References [ + ]





{kind=link}