
Contents
Sacrococcygeal teratoma
Sacrococcygeal teratoma also called fetal sacrococcygeal teratoma, is a non-cancerous (benign) tumor that develops before birth and grows from a baby’s tailbone (coccyx). Sacrococcygeal teratoma is the most common common congenital germ cell tumor found in newborns, occurring in 1 out of every 35,000 to 40,000 live births 1). This birth defect is more common in female than in male babies (female to male ratio 3:1-4:1) 2). Although these tumors can grow very large, they are usually not malignant (that is, cancerous), they may grow quite large and once diagnosed, always require surgical removal.
It is likely that all sacrococcygeal teratomas are present at birth (congenital) and most are discovered before birth by a routine prenatal ultrasound examination or an exam indicated for a uterus too large for dates. In rare cases, sacrococcygeal teratomas may be cancerous (malignant) at birth and many will become malignant if surgical resection is not performed. In extremely rare cases, sacrococcygeal tumors may be seen in adults. Most of these represent slow growing tumors that originated prenatally. In the majority of these cases, the tumor is benign, but may cause lower back pain and genitourinary and gastrointestinal symptoms. The cause of sacrococcygeal teratomas is unknown.
Sacrococcygeal teratomas are the most common solid tumor found in newborn babies (neonates). Sacrococcygeal teratomas affecting adults is extremely rare. Adults cases often represent tumors that were present at birth (congenital), but not detected until adulthood.
Sacrococcygeal teratoma tumor is usually covered with skin, but may be covered by a thin, transparent tissue called a membrane. Most tumors have many blood vessels coming through them. They come in many different sizes, and sometimes they may grow outward from the back or toward your child’s stomach.
Sacrococcygeal teratoma is usually discovered either because a blood test performed on the mother at 16 weeks shows a high alpha fetoprotein (AFP) amount, or because a sonogram is performed because the uterus is larger than it should be. The increased size of the uterus is often caused by extra amniotic fluid, called polyhydramnios. The diagnosis of sacrococcygeal teratoma can be made by an ultrasound examination.
When a prenatally diagnosed sacrococcygeal teratoma is associated with fetal hydrops, the tumor can become life-threatening to both mother and baby.
In severe cases, the tumor “steals” blood from fetal circulation, causing the heart to work extra hard and making cardiac failure possible. Cardiac failure exhibits as fetal hydrops, a massive accumulation of fluid in the body of the fetus. In our experience, fetal hydrops associated with sacrococcygeal teratoma is rapidly progressive and nearly always fatal.
For the mother, there is the risk of “maternal mirror syndrome” in which the mom’s condition parallels that of the sick fetus. When fetal hydrops is present, the mother may “mirror” the sick fetus, becoming ill with signs of preeclampsia. Preeclampsia, also called toxemia, is a condition characterized by pregnancy-induced high blood pressure, protein in the urine, and swelling due to fluid retention.
Sacrococcygeal teratoma can usually be cured by surgery after birth, but occasionally cause trouble before birth.
Patients in whom sacrococcygeal teratoma is diagnosed postnatally typically do well after early surgical resection, and the main cause of mortality in these patients (though rare) is attributed to malignancy. However, mortality associated with antenatally diagnosed sacrococcygeal teratoma is in the range of 30-50% 3) and is attributed to tumor morphology and vascularity. Whereas some fetuses are born without complications, others can develop high-output cardiac failure, nonimmune hydrops fetalis and, ultimately, fetal demise.
This wide disease spectrum has prompted several fetal treatment centers to identify ultrasound predictors of survival for fetuses with sacrococcygeal teratoma to help identify high-risk fetuses who may benefit from fetal intervention. The key to optimizing survival in these fetuses is intervention before the development of high-output cardiac failure, hydrops, and maternal mirror syndrome. Identifying fetuses at risk for hydrops and fetal demise isolates those who may be salvaged by reversing the pathophysiology—the premise behind fetal intervention 4).
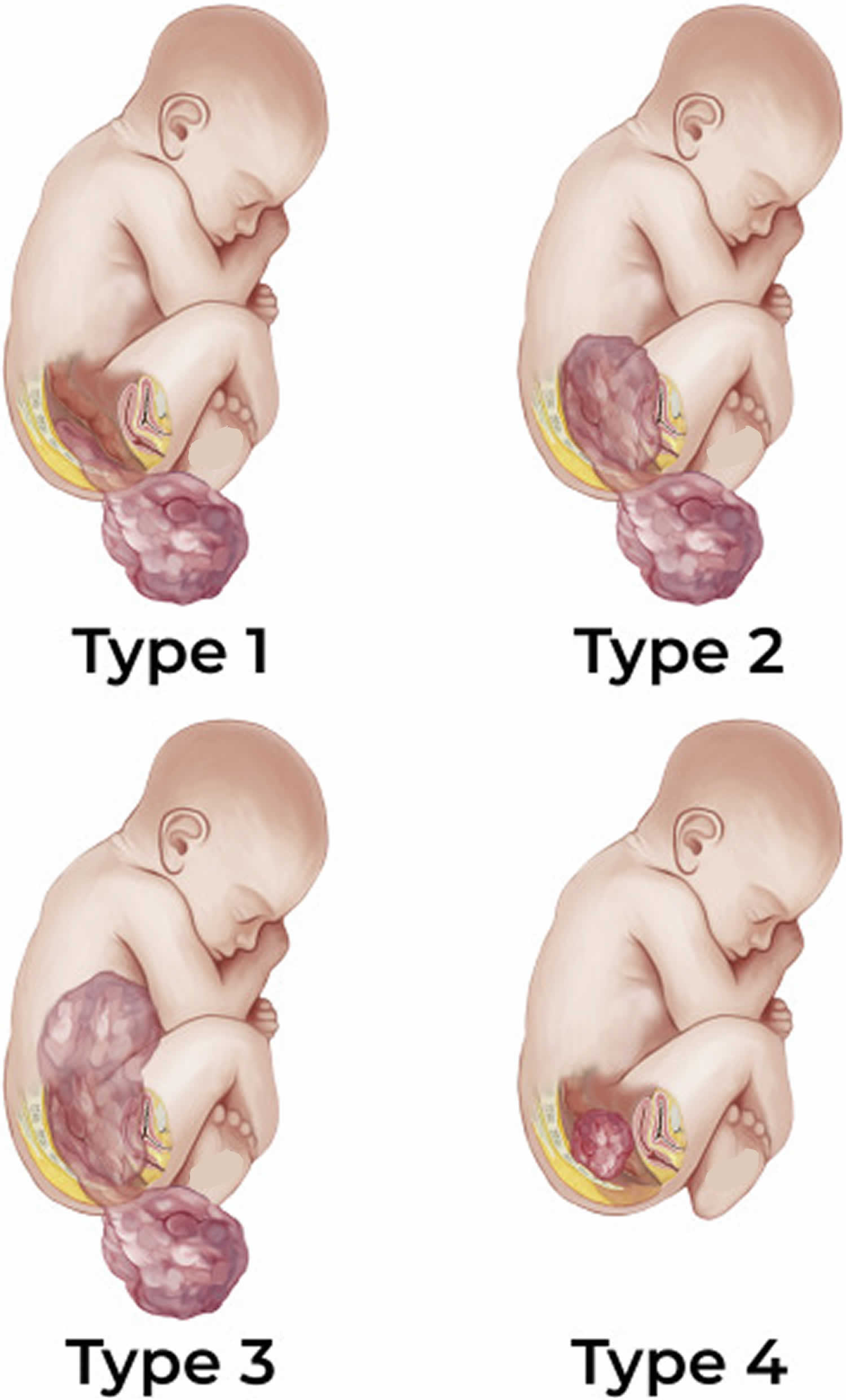
Figure 1. Sacrococcygeal teratoma types
How serious is my baby’s sacrococcygeal teratoma?
In order to determine the severity of your fetus’s condition it is important to gather information from a variety of tests and determine if there are any additional problems. These tests along with expert guidance are important for you to make the best decision about the proper treatment.
This includes:
- The type of defect—distinguishing it from other similar appearing problems.
- The severity of the defect—is your fetus’s defect mild or severe.
- Associated defects—is there another problem or a cluster of problems (syndrome).
The severity of sacrococcygeal teratoma is directly related to the size of the tumor and the amount of blood flow to the tumor. Both the size and the blood flow can now be accurately assessed by sonography and echocardiography. Small or medium-sized tumors without excessive blood flow will not cause a problem for the fetus. These babies should be followed with serial ultrasounds to make sure the tumor does not enlarge or the blood flow does not increase. They can be then delivered vaginally near term, and the tumor removed after birth.
Very large tumors are prone to develop excessive blood flow, which causes heart failure in the fetus. Fortunately, this is easy to detect by ultrasound. These babies need to be closely followed for the development of excess fluid in the abdomen (ascites), in the chest (pleural effusion), around the heart (pericardial effusion), or under the skin (skin edema). It is the extra blood flowing to the tumor that strains the fetal heart enough to cause heart failure (hydrops).
What is maternal mirror syndrome?
In cases with extreme fetal hydrops, the mother may be at risk for maternal mirror syndrome, which is a condition where the mother’s condition mimics that of the sick fetus. Because of a hyperdynamic cardiovascular state, the mother develops symptoms that are similar to pre-eclampsia and may include vomiting, hypertension, peripheral edema (swelling of the hands and feet), proteinuria (protein in the urine), and pulmonary edema (fluid in the lungs). Despite resection of the fetal sacrococcygeal teratoma, maternal mirror syndrome may still occur.
What are my choices during pregnancy?
Most newborns with sacrococcygeal teratoma survive and do well. Malignant tumors are unusual. Fetuses with large cystic sacrococcygeal teratomas rarely develop hydrops and therefore are not usually candidates for fetal intervention/surgery. These cases are best handled with surgical removal of the tumor after delivery. A Cesarean-section (C-section) delivery of the baby may be necessary if the tumor is larger than 10 cm (4 inches).
Because all sacrococcygeal teratomas require complete surgical resection after birth, arrangements should be made for the infant to be born at a specialized hospital with pediatric surgery expertise. Fetuses with large mostly solid tumors need to be monitored frequently between 18 and 28 weeks of gestation for rapid growth of the tumor and the development of excessive blood flow and heart failure (hydrops). A small number of these fetuses with large solid tumors develop hydrops, due to extremely high blood flow through the tumor. These fetuses may be candidates for fetal intervention.
Fetal intervention
Fetal intervention is only offered to women in whom there is evidence of heart failure in the fetus. Women who have fetuses with advanced hydrops, placentomegaly or maternal pre-eclampsia (high blood pressure, protein in the urine) are not candidates for fetal intervention as we have found that these symptoms (the so-called “mirror syndrome”) indicate an irreversible situation.
If hydrops develops after the 32nd week of pregnancy, the fetus may be delivered for intensive management after birth. Before 32 weeks gestation, fetal intervention may be advised to reverse the otherwise fatal heart failure.
Two approaches towards fetal intervention are possible for fetuses with hydrops: minimally invasive surgery and open fetal surgery. Minimally invasive fetal surgery involves inserting a needle through the mother’s abdomen and uterine wall and into the blood vessels that feed the tumor. Radiofrequency waves are used to destroy the blood vessels and, without blood flow, the tumor does not grow and heart failure (hydrops) is reversed. However, damage caused by the probe itself may be difficult to control. Another method of cutting off blood flow to the tumor is injection of drugs (for example, alcohol) that cause blood to clot. None of these methods has so far proven effective in all cases.
Open fetal surgery is an alternative option and has proven successful in a number of cases. In this case, the mother’s uterus is opened under general anesthesia and the fetus’s sacrococcygeal teratoma is surgically removed.
What will happen after birth?
All babies with sacrococcygeal teratoma should be delivered at a specialized hospital with pediatric surgery expertise. Tumors larger than 10 cm in diameter will require C-section delivery. The neonatologist will provide support in the intensive care nursery until the baby is stable enough for surgery. Surgical removal of small tumors is straightforward, but removal of large tumors can be very difficult and dangerous. The baby may require a blood transfusion(s) and intensive support for days or weeks after surgery. Most will get through this difficult period and enjoy a normal life. All babies should have yearly blood tests for elevated alpha feto-protein (AFP), which can signal recurrence of the tumor and possibly a malignancy. If the tumor is quite large and the surgeon performs an extensive complicated removal, there is an increased likelihood of long-term issues. A few babies may have difficulty with urination or stooling.
Sacrococcygeal teratoma types
Sacrococcygeal teratomas are categorized according to the classification developed by the American Academy of Pediatrics, Surgical Section 5).
Sacrococcygeal teratoma tumors are categorized according to their location and severity:
- Type 1 sacrococcygeal teratomas are external (outside the body) tumors and are attached to the tailbone.
- Type 2 sacrococcygeal teratomas have both internal (inside the body) and external parts.
- Type 3 sacrococcygeal teratomas can be seen from the outside, but most of the tumor is inside your child’s abdomen.
- Type 4 sacrococcygeal teratomas, the most serious tumors, can’t been seen from the outside. They are inside the body at the tailbone level. Type 4 has the highest rate of malignancy.
Whereas type 1 tumors, being primarily external to the fetus, are easily diagnosed prenatally and are amenable to fetal resection, type 4 tumors can be difficult to diagnose and are not amenable to fetal resection 6). The American Academy of Pediatrics, Surgical Section classification describes surgical anatomy and identifies tumors that are amenable to fetal resection, but it does not provide prognostic information, nor does it identify fetuses who would benefit from fetal intervention 7).
Sacrococcygeal teratoma cause
The cause of sacrococcygeal teratomas is unknown. Sacrococcygeal teratomas are germ cell tumors. Germ cells are the cells that develop into the embryo and later on become the cells that make up the reproductive system of men and women. Most germ cell tumors occur in the testes or ovaries (gonads) or the lower back. When these tumors occur outside of the gonads, they are known as extragonadal tumors. Researchers do not know how extragonadal germ cell tumors form. One theory suggests that germ cells accidentally migrate during to unusual locations early during the development of the embryo (embryogenesis). Normally, such misplaced germ cells degenerate and die, but in cases of extragonadal teratomas researchers speculate that these cells continue to undergo mitosis, the process where cells divide and multiply, eventually forming a teratoma.
Sacrococcygeal teratomas are thought to arise from an area under the coccyx called the “Henson’s Node”, which is located in the coccyx 8). Sacrococcygeal teratoma tumor arises from embryologically multipotent cells from the Hensen node. This is an area where primitive cells persist (germ cells) that can give rise to cells of the three major tissue layers of an embryo: ectoderm, endoderm, and mesoderm. These embryonic layers eventually give rise to the various cells and structures of the body. Sacrococcygeal teratomas can contain mature tissue that looks like any tissue in the body, or immature tissue resembling embryonic tissues.
Sacrococcygeal teratoma pathophysiology
The vascular supply to an sacrococcygeal teratoma commonly arises from the middle sacral artery, which can enlarge to the size of the common iliac artery and cause a vascular steal syndrome 9). These large vascular tumors can lead to high-output cardiac failure as a consequence of arteriovenous shunting through the tumor, resulting in placentomegaly, hydrops, and, ultimately, fetal demise 10).
Polyhydramnios is commonly seen because of increased fetal cardiac output, which often leads to preterm labor and premature rupture of membranes. Conversely, oligohydramnios can also occur if an intrapelvic portion of the tumor causes significant urinary obstruction 11).
In severe cases, maternal mirror syndrome, in which the mother develops symptoms that mimic those of the hydropic fetus, may develop. Mothers develop symptoms similar to those of severe preeclampsia, such as hypertension, emesis, peripheral edema, pulmonary edema, and proteinuria 12).
Fetal surgery is contraindicated after maternal mirror syndrome has developed; accordingly, prognostic indicators have been characterized so as to identify patients before terminal progression of this disease. Mothers who potentially have maternal mirror syndrome need to be very closely monitored and may require delivery or pregnancy termination for maternal safety.
Sacrococcygeal teratoma symptoms
The signs and symptoms of sacrococcygeal teratoma depend largely on the size and specific location of the tumor. Small tumors often do not cause any symptoms (asymptomatic) and can usually be removed surgically after birth without difficulty. However, larger sacrococcygeal tumors can cause a variety of complications before and after birth. Some tumors can be diagnosed by ultrasound before your child is born. An abnormally sized uterus is typically the first sign that your baby may have a tumor. The size discrepancy can be due to a massive tumor or to polyhydramnios (excess amniotic fluid). Less common presentations include maternal preeclampsia. Fetal sacrococcygeal teratoma may be cystic, solid or mixed in its sonographic appearance. The heterogeneous appearance of the mass may be due to mixed areas of tumor necrosis, cystic degeneration, hemorrhage or calcification.
Sacrococcygeal teratomas can grow rapidly in the fetus and require very high blood flow resulting in fetal heart failure, a condition known as hydrops. This is manifest as dilation of the heart, and the collection of fluid in tissues of the body, including the skin and body cavities such as around the lungs (pleural effusion), around the heart (pericardial effusion), and/or in the abdominal cavity (ascites). If neglected, hydrops can also be dangerous for the mother resulting in similar symptoms of swelling, hypertension, and fluid on the lungs with shortness of breath. In addition to hydrops, which can occur in approximately 15% of very large fetal sacrococcygeal teratomas, these tumors can cause polyhydramnios (too much amniotic fluid), fetal urinary obstruction (hydronephrosis), bleeding into the tumor or rupture of the tumor with bleeding into the amniotic space, or dystocia (a condition where the fetus cannot be delivered due to the size of the tumor. It is very important to have very close monitoring during pregnancy to recognize these symptoms as early as possible.
In adults, sacrococcygeal teratomas may not cause symptoms (asymptomatic). In some cases, they may cause progressive lower back pain, weakness, and abnormalities due to obstruction of the genitourinary and gastrointestinal tracts. Such symptoms include constipation and increased frequency of stools or urinary tract infections. In rare cases, sacrococcygeal tumors cause partial paralysis (paresis) of the legs and tingling or numbness (paresthesia).
Sacrococcygeal teratoma diagnosis
Most sacrococcygeal teratomas are now diagnosed antenatally because of the widespread use of routine obstetric ultrasonography 13).
If your baby is prenatally diagnosed with fetal sacrococcygeal teratoma, your doctor will continue to monitor your pregnancy to watch for any growth of the tumor or changes in your baby’s condition that may require intervention. Your baby may need fetal surgery to remove the sacrococcygeal teratoma if the size and severity of the tumor cause complications such as fetal hydrops that put you or your baby at risk.
Other tumors may not be visible until after your baby is born. After delivery, your child may have symptoms that indicate a possible sacrococcygeal teratoma, such as being unable to urinate or have a bowel movement because the tumor is pressing on their bladder or rectum. Some children have no symptoms at all.
In most cases, sacrococcygeal teratomas are diagnosed at birth when a large tumor is detected protruding from the sacral region. Many sacrococcygeal teratomas are found incidentally on routine prenatal ultrasounds or they may be detected on an ultrasound that is obtained because the uterus is too large for the stage of pregnancy due to the bulk of the tumor, or accumulation of amniotic fluid. During an ultrasound, reflected sound waves create an image of the developing fetus. Even small sacrococcygeal teratomas may be visible on an ultrasound picture.
In some cases, a sample of the amniotic fluid or maternal serum may be taken and studied to determine the levels of alpha-fetoprotein (AFP). AFP is a normal fetal plasma protein that when elevated may indicate the presence of certain conditions such as a sacrococcygeal teratoma.
If a sacrococcygeal teratoma is diagnosed prenatally a careful examination is usually done to rule out other anomalies. In some institutions a fetal MRI scan is also performed to better delineate the anatomy of the tumor and displaced structures. For large sacrococcygeal teratomas, very frequent ultrasounds and echocardiograms (to measure the size of the cardiac chambers and blood flows) are required to monitor for signs of evolving hydrops. During an echocardiogram, reflected sound waves are used to take pictures of the heart. It is extremely important that a medical team experienced with large fetal sacrococcygeal teratoma follows the pregnancy. All fetuses with large sacrococcygeal teratomas need delivery by a “classical” cesarean section (large incision in the uterus) to avoid tumor rupture and hemorrhage at the time of delivery. Most fetuses with large tumors are born premature and need expert perinatal care from a multidisciplinary team.
In adults, a diagnosis of sacrococcygeal teratoma may be suspected during a routine pelvic or rectal examination that detects the presence of a mass or tumor. A diagnosis of sacrococcygeal teratoma may be confirmed by surgical removal and microscopic examination of affected tissue (biopsy). One procedure is known as fine needle aspiration, in which a thin, hollow needle is passed though the skin and inserted into the nodule or mass to withdraw small samples of tissue for study.
In addition to an ultrasound, other specialized imaging techniques may be used to diagnose a tumor as well as evaluate the size, placement, and extension of the tumor and to serve as an aid for future surgical procedures. After birth, such imaging techniques may include computerized tomography (CT) scanning and magnetic resonance imaging (MRI). During CT scanning, a computer and x-rays are used to create a film showing cross-sectional images of certain tissue structures. An MRI uses a magnetic field and radio waves to produce cross-sectional images of particular organs and bodily tissues. In cases of malignant sacrococcygeal teratomas, laboratory tests and specialized imaging tests may also be conducted to determine possible infiltration of regional lymph nodes and the presence of distant metastases.
Sacrococcygeal teratoma staging
When an individual is diagnosed with a sacrococcygeal teratoma, assessment is also required to determine the extent or “stage” of the disease. Staging is important to help characterize the potential disease course and determine appropriate treatment approaches. Certain of the same diagnostic tests described above may be used in staging.
Sacrococcygeal teratomas are classified according to the American Academy of Pediatrics Surgical Section 14):
- Type 1 – the tumor is predominantly external with a very minimal internal component. Type I is rarely associated with malignancy.
- Type 2 – the tumor is predominantly external but has some internal extension into the presacral space.
- Type 3 – the tumor is visible externally, but is predominantly located in the pelvic area with some extension into the abdomen.
- Type 4 – the tumor is not visible externally and is located in the presacral space. Type 4 has the highest rate of malignancy.
Sacrococcygeal teratoma treatment
The initial management of a fetus with a sacrococcygeal teratoma requires the coordinated efforts of a perinatal team of medical professionals such as maternal fetal medicine physicians to deliver the infant, and pediatric surgeons and neonatologists to resect the tumor and manage the medical issues of the infant who can sometimes be critically ill. All prenatally diagnosed sacrococcygeal teratomas require surgery to remove the tumor during the neonatal period and if the tumor is large, as quickly as possible to avoid rupture of the sacrococcygeal teratoma. Resection always involves resection of the tumor along with the coccyx. Failure to resect the coccyx is associated with a 30% local recurrence rate of the sacrococcygeal teratoma tumor. This can usually be done from the back of the neonate but for some tumors with extensive extension into the pelvis and abdomen, an abdominal incision must also be performed. Most children that undergo early resection of sacrococcygeal teratomas ultimately do well with a very low incidence of malignant or benign tumor recurrance, and normal urogenital, bowel, and lower extremity neurologic function. These children are usually followed by the pediatric surgeon by rectal examinations and interval serum AFP levels to monitor for recurrence for 3 years before they are considered cured with no possibility of tumor recurrence.
In rare instances where malignancy is diagnosed by the pathologist after resection a team of medical professionals who specialize in the diagnosis and treatment of cancer (medical oncologists) will need to be consulted. Specific therapeutic procedures and interventions may vary, depending upon numerous factors, such as primary tumor location and corresponding complications; extent of the primary tumor (stage); whether it has spread to lymph nodes or distant sites; an individual’s age and general health; and/or other elements. Decisions concerning the use of particular interventions should be made by physicians and other members of the health care team in careful consultation with the patient or parents, based upon the specifics of the case; a thorough discussion of the potential benefits and risks; and other appropriate factors.
In rare cases, complications resulting from a sacrococcygeal teratoma may necessitate intervention before birth (prenatally). Interventions such as tapping the amniotic fluid (amniocentesis) to reduce the volume and delay the onset of preterm labor may be required. If the tumor has hemorrhaged and the fetus is anemic, a fetal blood transfusion may be helpful. Occasionally, an obstructed fetal urinary tract will need to be treated by a vesicoamniotic shunt (a catheter between the bladder and amniotic fluid) to relieve the obstruction and prevent damage to the kidneys. In rare cases when the fetus is documented to be in the early stages of hydrops, open fetal surgery may be required (surgery on the fetus in the womb) to “debulk” the tumor and reduce the demand for blood flow. After removal of the bulk of the tumor, the fetus is returned to the womb so that the hydrops can improve prior to birth. Although this has been successful about 50% of the time, it is a major undertaking and extensive consideration of the risks to the mother is appropriate. Although radio frequency ablation (a technique where a needle is inserted into the tumor and radiofrequency energy is applied to the tumor to destroy blood flow) has been reported, all survivors have had complications of damage to the genitourinary system so this approach is considered highly experimental.
In adults, surgical removal of the entire tumor and the tailbone (coccyx) is the main treatment option. Removal of the coccyx lowers the chance of recurrence. For benign tumors surgical removal of the tumor is usually sufficient. However, for malignant tumors, affected individuals should receive additional treatment with chemotherapy and radiation therapy.
Because malignant sacrococcygeal teratomas are extremely rare, especially in adults, no standard chemotherapeutic regimen or radiation therapy has been established.
Monitoring and delivery
If your baby’s condition is stable with no high output cardiac failure (fetal hydrops), your pregnancy will be followed with regular ultrasound monitoring. If the sacrococcygeal teratoma is small, a vaginal delivery at term may be planned.
If the sacrococcygeal teratoma is large or if there is an excess of amniotic fluid (polyhydramnios), an early cesarean section is planned to avoid tumor rupture as well as the risks of preterm labor and premature delivery.
If fetal hydrops develops, you may be a candidate for fetal surgery.
Sacrococcygeal teratoma surgery
Fetuses with sacrococcygeal teratoma are considered for fetal surgery to remove the tumor or fetal intervention only in extreme cases on an individual basis. Depending on the diagnosis and severity of your child’s sacrococcygeal teratoma, they may undergo fetal surgery to remove the sacrococcygeal teratoma before birth, or they may have tumor resection surgery after they’re born.
Fetal surgery is only indicated when fetal hydrops is present, putting your child’s life at risk.
Small tumors without significant vascularity are unlikely to affect the fetus significantly 15). These fetuses are unlikely to develop high-output cardiac failure or hydrops and can be monitored throughout gestation with serial ultrasound. Those with signs of placentomegaly and hydrops after lung maturity (usually after 32 weeks’ gestation) are delivered on an emergency basis. Only fetuses of less than 32 weeks’ gestation with signs of impending hydrops that have tumors amenable to surgical resection are considered for fetal intervention 16).
As with all invasive procedures, the risks and benefits of fetal intervention must be considered for each patient. However, consideration for the risk to and safety of the pregnant mother are unique to fetal surgery. Before fetal intervention is considered, a multidisciplinary team should counsel and evaluate each family. The evaluation should include the following 17):
- Detailed ultrasound to confirm the diagnosis and to detect any other anatomic abnormalities
- Fetal magnetic resonance imaging (MRI) for additional anatomic information
- Fetal echocardiography to rule out congenital heart disease and to assess fetal cardiac function
- Amniocentesis for fetal karyotyping
In 2009, Wilson et al 18) proposed the following criteria for surgical resection of sacrococcygeal teratoma:
- No maternal contraindications to fetal surgery (medical or surgical issues, body mass index [BMI] < 36, anesthesia risks)
- Fetal gestational age of 20-30 weeks
- A favorable American Academy of Pediatrics Surgical Section stage and no additional anomalies
- Impending hydrops (evidence of ascites, pleural effusion, and subcutaneous edema)
- Normal fetal karyotype
- Fetal cardiac output greater than 600-900 mL/kg/min (adjusted for gestational age)
Contraindications
Contraindications for fetal intervention for sacrococcygeal teratoma include the following 19):
- Significant placentomegaly (placental thickness at cord insertion >35-45 mm with a gestational age < 30 weeks)
- Maternal mirror syndrome
- Multiple gestation
- Chromosomal abnormality
- Other fetal anatomic abnormalities
Ex-Utero Intrapartum Treatment (EXIT) Procedure
In some cases, early delivery of the fetus without sacrococcygeal teratoma resection has led to adverse events between delivery and neonatal resection (eg, tumor hemorrhage and fetal exsanguination). In cases where delivery and tumor resection may lead to hemodynamic instability, the ex-utero intrapartum treatment (EXIT) procedure may be considered. EXIT to resection of fetal sacrococcygeal teratoma may be considered for a fetus of 27-32 weeks’ gestation with a large vascular type 1 or 2 tumor requiring early delivery but in the absence of maternal contraindications 20).
The EXIT procedure, originally developed to establish an airway in a fetus with airway compromise while the fetus was still connected to placental circulation for oxygenation, has been adapted to resuscitate fetuses with other anomalies who may experience instability during birth 21). For fetuses with sacrococcygeal teratoma, the EXIT procedure allows tumor debulking to interrupt the vascular steal phenomenon, which minimizes preoperative manipulation and trauma to the tumor 22). The infant can be stabilized before definitive oncologic resection.
The EXIT procedure is performed with the mother under general anesthesia 23) to maximize uterine relaxation and uteroplacental blood flow. The hysterotomy, fetal monitoring, and IV access are performed as described for open fetal surgery.
After debulking of the tumor, the fetus is intubated and given surfactant before the umbilical cord is clamped. The hysterotomy, fascial, and skin closure are performed in the same fashion as the open fetal sacrococcygeal teratoma resection.
Roybal et al 24) reported one survivor using this technique, with neurologic complications due to tumor invasion into the spinal canal. Surgeons at the University of California San Francisco 25), have treated two fetuses with EXIT to sacrococcygeal teratoma resection, with a survival of 50%; one patient died of necrotizing enterocolitis and sepsis.
Open fetal surgery
Fetal exposure for sacrococcygeal teratoma resection is similar to what has been reported for other open fetal surgical procedures 26).
The uterus is exposed through a Pfannenstiel incision. If the placenta is located posteriorly, the superior and anterior skin and subcutaneous tissue flaps are created, and a midline fascial incision is then created to expose the uterus.
An anterior hysterotomy is performed while the uterus remains in the abdomen. However, if the placenta is located anteriorly, the rectus muscles will have to be divided in order to prevent uterine vascular compromise as the uterus is lifted out of the abdomen to perform a posterior hysterotomy.
A large ring retractor is used to maintain exposure 27).
Intraoperative sterile ultrasonography is used to delineate the position of the fetus and the placenta, and continuous echocardiography is used to monitor fetal well-being throughout the operative procedure.
If the pregnancy is complicated by polyhydramnios and placentomegaly, the true edge of the placenta is not always appreciated on ultrasonography, and the hysterotomy should be planned even farther away from this edge.
Stay sutures are placed on the uterus, and a small hysterotomy is made, which is then extended with a stapler designed especially to be used on the uterus 28). This hemostatic stapler is used to secure the membranes to the uterine wall to prevent separation of membranes. The fetus is positioned so that the tumor is exposed through the hysterotomy.
A ”fetal cocktail,” which consists of a paralytic agent (either pancuronium or rocuronium) and fentanyl, is administered to the fetus with an intramuscular injection. A pulse oximeter is placed on the fetus to monitor fetal well-being (see the first image below). Intravenous (IV) access is obtained for administration of fluids, blood, or medication. Use of this strategy of fetal monitoring during open fetal surgery allows administration of fluids in response to changes in preload during the resection and may improve fetal survival 29).
The fetus is kept buoyant and warm in the uterus with continuous infusion of warmed lactated Ringer solution into the uterus.
After the sacrococcygeal teratoma is resected, a two-layer uterine closure is performed. However, before the uterus is completely closed, lactated Ringer solution is instilled into the uterus until ultrasound shows that normal amniotic fluid volume has been restored.
An omental flap can be secured over the hysterotomy, and the fascia, subcutaneous tissue, and skin are closed.
Radiofrequency ablation
Several centers have described salvage of hydropic fetuses with sacrococcygeal teratoma with open fetal resection. However, preterm labor remains the Achilles heel of fetal surgery. To circumvent preterm labor and to decrease maternal morbidity associated with fetal intervention for sacrococcygeal teratoma, minimally invasive techniques, such as radiofrequency ablation (RFA), have been described 30).
This technique employs US guidance to target the vessels feeding the sacrococcygeal teratoma to reduce tumor vascularity. An eight-prong LeVeen radiofrequency probe is deployed through a 15-gauge needle into an umbrellalike configuration to a diameter of 20-35 mm 31). It delivers energy in a spherical volume to cause tissue and tumor necrosis.
Radiofrequency ablation for sacrococcygeal teratoma has been controversial. The potential risks of this procedure include gas embolization due to microbubbles, hyperkalemia caused by tissue necrosis, perineal damage, and hemorrhage.
In a report of four fetuses with sacrococcygeal teratoma, radiofrequency ablation successfully reduced tumor vascularity in all cases 32). However, intrauterine fetal demise due to hemorrhage into the tumor occurred in one case, and another fetus underwent termination after postoperative MRI showed fetal brain damage. The two remaining fetuses survived but had evidence of perineal damage at birth.
Lam et al reported using radiofrequency ablation to treat sacrococcygeal teratoma in an 18-week-old fetus, but the fetus died 2 days postoperatively 33). Ibrahim et al 34) reported a fetus born with sciatic nerve injury and malformation of the acetabulum and femoral head after radiofrequency ablation for sacrococcygeal teratoma. A study from Korea 35) reported six cases of fetal sacrococcygeal teratoma treated with radiofrequency ablation; five of the six patients survived, and one patient had left-leg palsy and fecal and urinary incontinence.
In summary, although radiofrequency ablation has been used as salvage therapy in fetuses who would have otherwise died, many of these patients were born with complications. The keys to successful treatment with radiofrequency ablation may be (1) limiting the extent of coagulation in any single attempt to prevent massive hemorrhage or perineal necrosis and (2) performing a series of limited ablations 36). Radiofrequency ablation as a treatment modality for fetal sacrococcygeal teratoma remains limited and problematic, and more studies are necessary to determine whether and how this technique should be used.
Laser ablation
Laser ablation for sacrococcygeal teratoma was first described in 1996 at 20 weeks’ gestation 37). The pregnancy was complicated by polyhydramnios but not by placentomegaly or hydrops. Two unsuccessful attempts were made at 20 weeks’ and 26 weeks’ gestation to ablate the main vessels feeding the sacrococcygeal teratoma, but the infant survived.
In this technique, local anesthesia is infiltrated into the skin and subcutaneous tissues 38). Cordocentesis is performed to deliver fetal anesthesia with fentanyl (15 µg/kg) and pancuronium (2 mg/kg) 39). This can also be delivered intramuscularly to the fetus. Under US guidance, a 1.9-mm 60° fetoscope is introduced into the amniotic cavity percutaneously through a sheath, and a 0.4-mm neodymium-doped yttrium-aluminum-garnet (Nd:YAG) laser fiber is used to coagulate the vessels 40).
In a retrospective study of 12 patients undergoing fetal intervention for sacrococcygeal teratoma, four patients underwent laser ablation, but only one patient survived 41). In a case report, a 24-week-old hydropic fetus underwent percutaneous laser ablation for sacrococcygeal teratoma but died 2 days after fetal intervention 42). In another study, a 22-week-old fetus underwent percutaneous laser ablation of tumor vessels and survived.
An additional retrospective multicenter study identified five fetuses that underwent minimally invasive fetal intervetion for hydrops or cardiac insufficiency as a result of sacrococcygeal teratoma 43). Four of these five fetuses underwent laser ablation, and three of them were targeted vascular ablations. Survival for the fetuses that underwent fetal intervention was 40%, but many patients required multiple procedures because of the recurrence of hydrops, cardiac insufficiency, or both.
Laser ablation for sacrococcygeal teratoma, like radiofrequency ablation for sacrococcygeal teratoma, represents the movement in fetal surgery toward minimally invasive techniques. However, the outcomes vary, and current experience is too limited to determine whether laser ablation will be effective in reducing mortality in fetuses with sacrococcygeal teratoma.
Sacrococcygeal teratoma prognosis
Most fetal sacrococcygeal teratomas are generally not malignant and the prognosis tends to be good after resection. Several institutions have reported outcomes with and without fetal intervention for antenatally diagnosed sacrococcygeal teratoma 44). Among patients with antenatally diagnosed sacrococcygeal teratoma, 36-41% require fetal intervention 45).
Most fetuses with sacrococcygeal teratoma do well with surgical treatment after birth. Babies with small tumors that can be removed along with the coccyx bone after birth can be expected to live normal lives. They will need to be born in a hospital with pediatric surgeons and a specialized nursery. After hospital discharge, it is our practice to follow children who have had an sacrococcygeal teratoma resection closely. Experts recommend follow-up with a pediatric surgeon and pediatric oncologist with blood testing of alpha-fetoprotein (AFP) throughout childhood.
Fetuses with larger tumors or tumors that go up inside the baby’s abdomen will require more complex surgery after birth, but in general do well. Again, they will have to be followed by an oncology service with blood tests for several years. Fetuses with very large tumors, which can reach the size of the fetus itself, can pose a difficult problem both before and after birth.
Experts have found that those sacrococcygeal teratomas that are largely cystic (fluid-filled) generally do not cause a problem for the fetus before birth. However, when the sacrococcygeal teratoma is made up of mostly solid tissue, with a lot of blood flow, the fetus can suffer adverse effects. This is because the fetus’s heart has to pump not only to circulate blood to its body, but also to all the blood vessels of the tumor, which can be as big as the fetus. In essence, the heart is performing twice its normal amount of work. The amount of work the heart is doing can be measured by fetal echocardiography. This sensitive test can determine how hard the heart is working when the fetus is approaching hydrops, or heart failure. If hydrops does develop, usually in rapidly growing solid tumors, the fetus usually will not survive without immediate intervention before birth. These fetuses must be followed very closely, and may benefit from fetal surgery.
If hydrops does not develop, these babies may require Cesarean-section delivery and an extensive operation after birth. Most babies will do well once the tumor is completely removed. Long-term consequences include the recurrence of the tumor or difficulty with bowel and/or bladder control as a consequence of the surgical procedure. Your child should be followed by an oncologist and pediatric surgeon throughout childhood.
Mortality due to sacrococcygeal teratoma is mainly attributed to tumor morphology; small cystic sacrococcygeal teratomas rarely cause problems in utero. Rapid growth of large vascular tumors can rupture and hemorrhage during delivery, and this is usually fatal 46).
The overall survival rate of antenatally diagnosed sacrococcygeal teratoma is 47-83% 47), but the survival rate after fetal surgery is 50-75% 48). It is important to note that survival after fetal intervention should be compared with survival for the subgroup of patients with hydrops and no intervention, in whom the survival rate approaches 0% 49).
About 40-50% of survivors with antenatally diagnosed sacrococcygeal teratoma have long-term morbidity, which may include obstructive uropathy, bowel and bladder incontinence caused by damage to the sacral nerves due to the tumor or damage during sacrococcygeal teratoma resection, and dissatisfaction with cosmetic outcomes 50).
Prognostic indicators
Placentomegaly and hydrops are harbingers of fetal demise in sacrococcygeal teratoma 51).
A retrospective review of 17 fetuses with antenatally diagnosed sacrococcygeal teratoma treated at the University of California, San Francisco 52), between 1986 and 1998 evaluated the factors associated with hydrops. There was a significant difference in tumor morphology (solid vs cystic) and vascularity in fetuses who developed hydrops compared with those without hydrops. In addition, fetuses who developed hydrops were diagnosed at an earlier gestational age (19 vs 25 weeks) and were delivered at an earlier gestational age (28 vs 38 weeks).
In this series, 12 fetuses developed hydrops, four of whom survived 53). Of the four survivors, three underwent fetal intervention because they developed hydrops before viability, and one patient developed hydrops at 32 weeks’ gestation and was delivered immediately. All fetuses who did not develop hydrops survived.
This study showed that fetuses with predominantly solid and highly vascular tumors were at high risk for developing hydrops. These patients should undergo close follow-up throughout gestation with serial US and echocardiography and may be considered for fetal intervention upon signs of impending hydrops.
A retrospective review of 23 patients evaluated at the Children’s Hospital of Philadelphia 54) between 2003 and 2006 with antenatally diagnosed sacrococcygeal teratoma showed that sacrococcygeal teratomas with a growth rate exceeding 150 cm³/week are associated with increased perinatal mortality.
In a study from University of California San Francisco that retrospectively reviewed 28 fetuses with antenatally diagnosed sacrococcygeal teratoma between 1991 and 2005, solid tumor volume–to–head volume ratio (STV/HV) on ultrasound was identified as a predictor of poor outcomes 55). All patients with an solid tumor volume–to–head volume ratio (STV/HV) lower than 1 survived, whereas 61% of fetuses with an solid tumor volume–to–head volume ratio (STV/HV) higher than 1 died.
In addition, the study determined that 97.3% of fetuses with an solid tumor volume–to–head volume ratio (STV/HV) higher than 1 were associated with one or more abnormal US findings, such as polyhydramnios, hepatomegaly, placentomegaly, cardiomegaly, ascites, pericardial effusion, or integumentary edema 56). With serial ultrasound , increases in the STV/HV ratio can guide management in fetal sacrococcygeal teratoma so that fetal intervention or early delivery can be performed before hydrops develops 57).
In a study from the Fetal Center at Texas Children’s Hospital 58), tumor volume–to–fetal weight ratio (TFR) was a marker of poor outcome in 12 fetuses with sacrococcygeal teratoma between 2004 and 2009. With MRI or US, tumor volume was determined by the prolate ellipsoid formula and fetal weight by the Hadlock formula. A tumor volume–to–fetal weight ratio (TFR) higher than 0.12 before 24 weeks’ gestation predicted poor outcomes (fetal hydrops, demise, or neonatal death) with 100% sensitivity, 83% specificity, a negative predictive value of 100%, and a positive predictive value of 80%.
Of the 12 fetuses with sacrococcygeal teratoma in this series, 33% (4/12) developed hydrops 59). All fetuses who developed hydrops had a tumor volume–to–fetal weight ratio (TFR) higher than 0.12 by 24 weeks’ gestation, and three fetuses died. One patient underwent fetal intervention after hydrops developed and survived. Thus, tumor volume–to–fetal weight ratio (TFR) may be used to identify fetuses with sacrococcygeal teratoma who are at risk for poor outcomes before 24 weeks’ gestation and who may benefit from fetal intervention.
Tumor volume–to–fetal weight ratio (TFR) higher than 0.12 in combination with tumor morphology was further validated as a sonographic predictor of poor prognosis in a subsequent retrospective study from University of California San Francisco 60).
In a review of 79 fetuses with antenatally diagnosed sacrococcygeal teratoma at three fetal centers from 1986 to 2011, receiver operating characteristic (ROC) analysis revealed that a tumor volume–to–fetal weight ratio (TFR) higher than 0.12 before 24 weeks’ gestation was predictive of a poor prognosis, as was solid tumor morphology and the presence of hydrops 61). However, none of these factors were found to be independent predictors of a poor prognosis on multivariate analysis.
In a retrospective review 62) of 28 pathology-confirmed isolated sacrococcygeal teratoma patients evaluated with at least two documented ultrasound scans and followed through hospital discharge between 2005 and 2012, a faster sacrococcygeal teratoma growth rate—calculated as the difference between tumor volumes on a late-gestation sonogram and an early-gestation sonogram divided by the difference in time—was associated with adverse outcomes (death, high-output cardiac failure, hydrops, and preterm delivery).
Sacrococcygeal teratoma can create a low-resistance large arteriovenous shunt, which can progressively increase preload and afterload on the fetal heart, leading to volume overload, ventricular dilation, ventricular hypertrophy, and high-output cardiac failure 63). A 10-year retrospective review 64) of seven fetuses showed that the most important prognostic criteria for maternal and fetal complications due to antenatally diagnosed sacrococcygeal teratoma included cardiomegaly, hydrops, and increased preload indexes of the fetal venous system.
Studies on fetuses with sacrococcygeal teratoma show that combined cardiac output increases dramatically before the development of hydrops 65). Fetuses with combined cardiac output that exceeded 700-800 mL/kg/min died in utero 66). Rychik et al 67) analyzed the acute cardiovascular effects of fetal surgery in four patients with sacrococcygeal teratoma and saw a significant decrease in combined cardiac output (690 ± 181 mL/kg/min vs 252 ± 82 mL/kg/min) after fetal resection of sacrococcygeal teratoma.
In a retrospective review 68) of 11 fetuses with sacrococcygeal teratoma, those with poor outcomes (ie hydrops, fetal demise, neonatal death) had a cardiothoracic ratio higher than 0.5, a combined ventricular output exceeding 550 mL/kg/min, tricuspid or mitral valve regurgitation, or a mitral valve Z-score higher than 2. Identifying these cardiovascular indicators of poor outcome helps identify patients at high risk for fetal demise and can prompt fetal surgical intervention before the development of hydrops.
References [ + ]





{kind=link}