Contents
Hyperparathyroidism in children
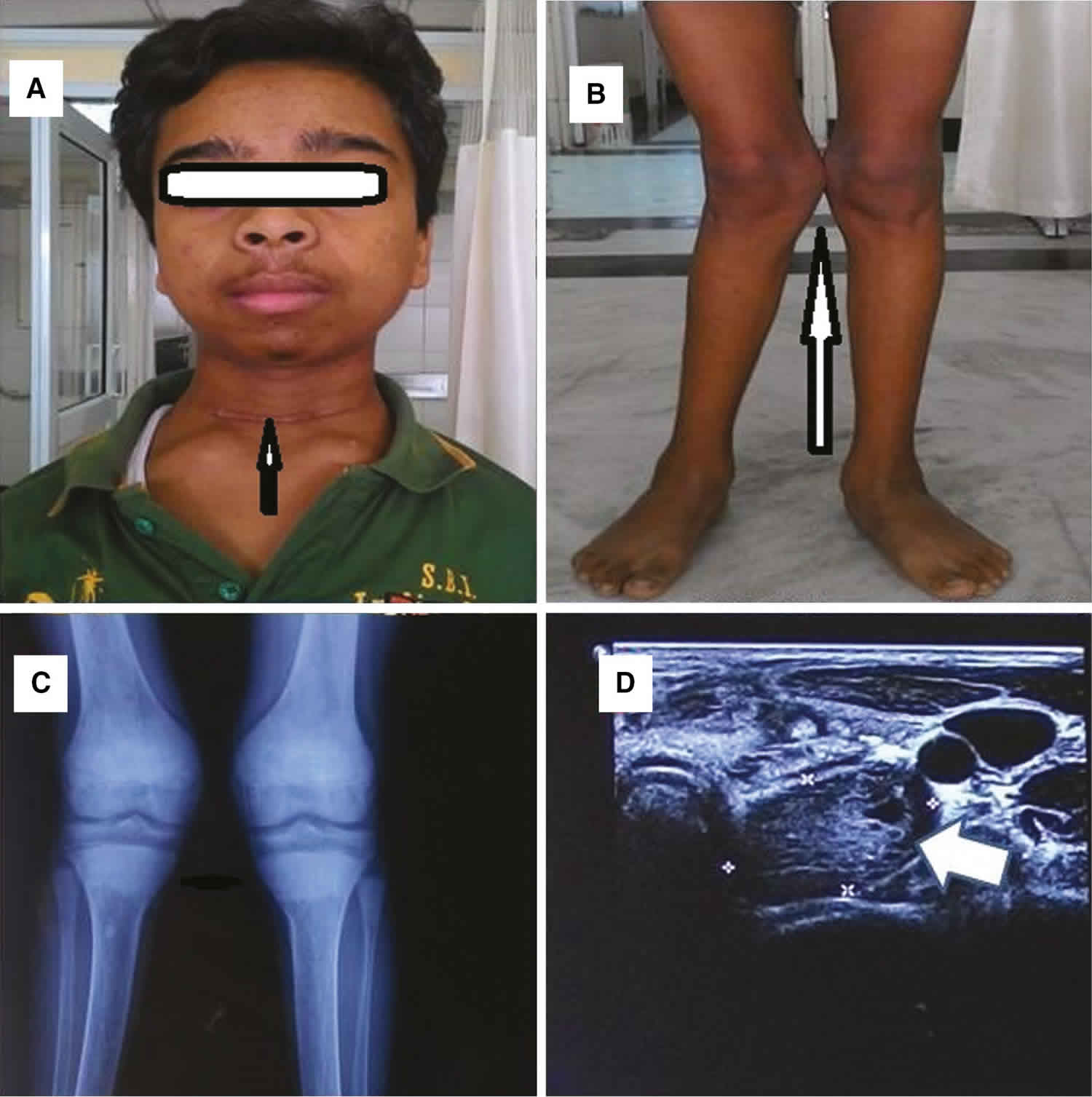
Hyperparathyroidism is caused by overactive parathyroid glands. Parathyroid glands are tiny glands located near the thyroid. Hyperparathyroidism is quite rare in children and usually presents with bone disease or kidney stones 1). Overactive parathyroid glands produce high levels of parathyroid hormone (PTH), which, in turn, results in increased levels of calcium in the bloodstream 2). The excess calcium released by the bones can lead to osteoporosis and osteomalacia (both bone-weakening diseases). Another result of hyperparathyroidism is kidney stones, because of high levels of calcium excreted into the urine by the kidneys.
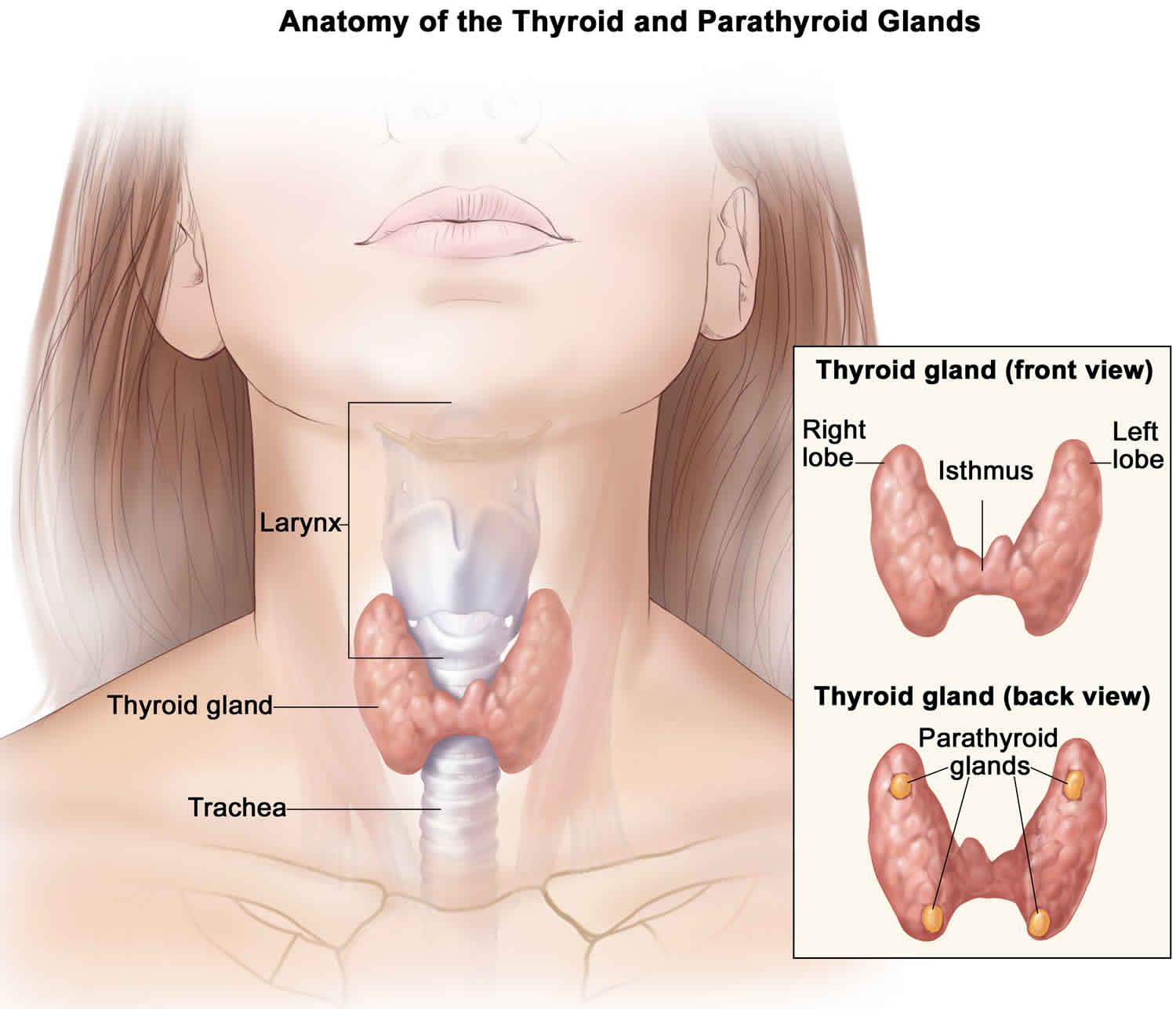
The parathyroid glands are 4 tiny glands that lie in your neck, just behind the butterfly shaped thyroid gland. Sometimes the parathyroid glands may also be found elsewhere in the body.
The parathyroid glands are not related to the thyroid except by name ( ‘para’ comes from the Greek for ‘near’) and they have a completely different function from the thyroid.
Most people have four tiny yellow glands which are about the size of a grain of rice. The job of the parathyroid glands is to continually adjust your calcium levels to keep them stable. Parathyroid hormone (PTH) is secreted by parathyroid glands and plays a role in calcium and skeletal metabolism 3). Parathyroid hormone (PTH) helps manage levels of calcium in your bloodstream. High levels of the parathyroid hormone (PTH) lead to high levels of calcium. This occurs because the hormone causes bones to start breaking down. Minerals from the bone are released into the blood. This causes high levels of calcium in the blood (hypercalcemia). The calcium is then processed by the kidneys. This process can cause thinning bones (osteoporosis) and kidney stones. Kidney stones are hard mineral crystals that get stuck in the urinary system. On the other hand, the secretion of parathyroid hormone (PTH) is reduced by 1,25 (OH)(2) vitamin D(3) 4).
Figure 1. Parathyroid glands
What do the parathyroid glands do?
The parathyroid glands’ only purpose is to make parathyroid hormone (PTH), which helps maintain the right balance of calcium in your body. Parathyroid hormone (PTH) raises blood calcium levels by:
- causing bone, where most of your body’s calcium is stored, to release calcium into the blood
- helping your intestines absorb calcium from food
- helping your kidneys hold on to calcium and return it to your blood instead of flushing it out in urine
When the level of calcium in your blood falls too low, the parathyroid glands release just enough parathyroid hormone (PTH) to bring your blood calcium levels back to normal.
You need calcium for good health. This mineral helps build bones and teeth and keep them strong. Calcium also helps your heart, muscles, and nerves work normally.
Although their names are similar, the parathyroid glands and the thyroid gland are not related.
Pediatric hyperparathyroidism causes
Causes of hyperparathyroidism include benign (noncancerous) tumors on the parathyroid glands or enlargement of the parathyroid glands.
Primary hyperparathyroidism
“Primary” means this disorder begins in the parathyroid glands, rather than resulting from another health problem such as kidney failure. In primary hyperparathyroidism, one or more of the parathyroid glands is overactive. As a result, the gland makes too much parathyroid hormone (PTH).
In primary hyperparathyroidism too much parathyroid hormone (PTH) is produced by one or more of the parathyroid glands because they have become enlarged or overactive. This in turn causes the body to release calcium from the bones into the blood and results in high calcium levels (hypercalcaemia).
Primary hyperparathyroidism causes 5):
- Single adenoma
- Multigland disease
- Familial causes of hyperparathyroidism
- Multiple endocrine neoplasia type 1 (MEN 1)
- Multiple endocrine neoplasia type 2A (MEN 2A)
- Familial hyperparathyroidism
- Hyperparathyroidism-jaw tumor syndrome
- Parathyroid carcinoma
In about 8 out of 10 people the most common cause of primary hyperparathyroidism is a parathyroid gland becoming enlarged due to the development of a benign (non-cancerous) tumor called an adenoma 6). The tumor causes the gland to become overactive. This is more commonly diagnosed in women, particularly postmenopausal women, but can affect both men and women and all ages, including, less commonly, children.
In most other cases, extra PTH comes from two or more adenomas or from hyperplasia, a condition in which all four parathyroid glands are enlarged. People with rare inherited conditions that affect the parathyroid glands, such as multiple endocrine neoplasia type 1 or familial hypocalciuric hypercalcemia are more likely to have more than one gland affected.
Sometimes all four parathyroid glands may become enlarged – this is called parathyroid hyperplasia. This may occur sporadically (without a family history) or as part of three familial (inherited) syndromes: multiple endocrine neoplasia type 1 (MEN 1) and multiple endocrine neoplasia type 2A (MEN 2A), and isolated familial hyperparathyroidism. In MEN 1, the problems in the parathyroid glands are associated with other tumors in the pituitary and the pancreas. In MEN 2A, overactivity of the parathyroid glands is associated with tumors in the adrenal gland or thyroid.
Radiotherapy treatment to your head or neck may increase the risk of developing a parathyroid adenoma or carcinoma (cancer). Only in extremely rare cases will the tumor be due to parathyroid cancer (parathyroid carcinoma).
How common is primary hyperparathyroidism?
In the United States, about 100,000 people develop primary hyperparathyroidism each year 7). Primary hyperparathyroidism is one of the most common hormonal disorders.
Who is more likely to develop primary hyperparathyroidism?
Primary hyperparathyroidism most often affects people between age 50 and 60. Women are affected 3 to 4 times more often than men 8). The disorder was more common in African Americans, followed by Caucasians, in one large study performed in North America 9).
Pediatric hyperparathyroidism symptoms
Most people with primary hyperparathyroidism have no symptoms. When symptoms appear, they’re often mild and similar to those of many other disorders.
The following are the most common symptoms of hyperparathyroidism in children. However, each child may experience symptoms differently. Symptoms may include:
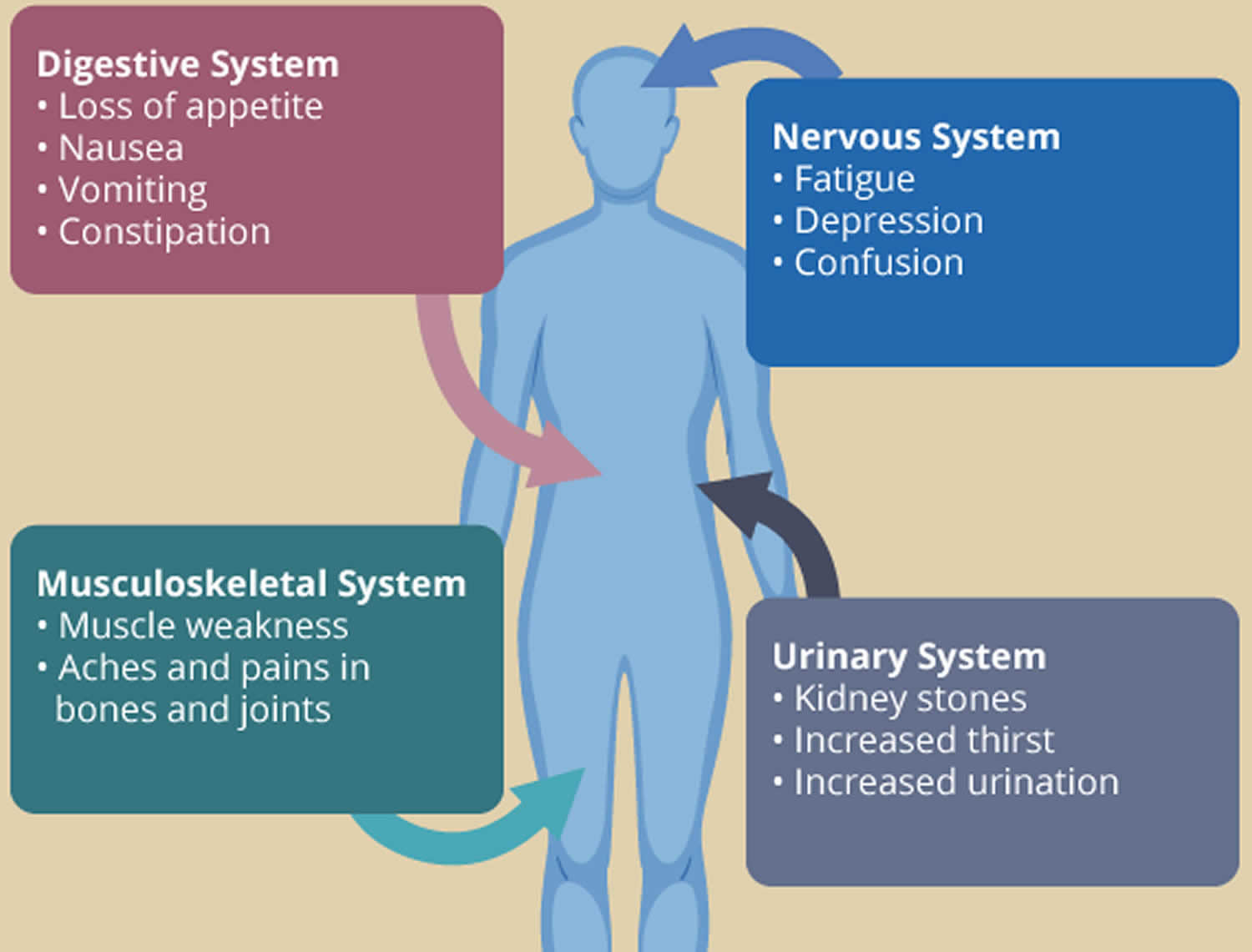
- Kidney pain (due to the presence of kidney stones)
- Diminished bone density that causes bone pain
- Joint aches and pains
- Abdominal pain
- Nausea
- Vomiting
- Fatigue
- Excessive urination
- Confusion
- Muscle weakness
- Fractures
- Weight loss
- Diarrhea
- Depression
- Headache
Figure 2. Primary hyperparathyroidism symptoms
If left untreated, symptoms can become much worse.
In severe cases, extremely high levels of calcium (hypercalcemia) can cause:
- vomiting
- drowsiness
- dehydration
- confusion – difficulty thinking and speaking clearly
- agitation
- muscle spasms, tremors.
- bone fractures
- irregular heart beat
- high blood pressure
- loss of consciousness
- coma and, very rarely, if not treated, death
Hypercalcemia can be a life threatening condition if it is not treated.
Compared to adults, children more commonly have symptoms and involvement of other parts of the bodies, such as kidney, pancreas, and bones, at diagnosis. Additionally, hyperparathyroidism in children is more commonly part of a syndrome, such as multiple endocrine neoplasia (MEN).
The symptoms of hyperparathyroidism may resemble other conditions or medical problems. Always consult your child’s doctor for a diagnosis.
Long term effects
If primary hyperparathyroidism goes undiagnosed, further complications, can develop. Primary hyperparathyroidism most often affects the bones and kidneys, although it also may play a part in other health problems.
High blood calcium levels might play a part in other problems, such as heart disease, high blood pressure, and trouble concentrating. However, more research is needed to better understand how primary hyperparathyroidism affects the heart, blood vessels, and brain.
These are common complications of primary hyperparathyroidism:
Kidney stones
The small intestine may absorb more calcium from food, adding to high levels of calcium in your blood. Extra calcium that isn’t used by your bones and muscles goes to your kidneys and is flushed out in urine. The kidneys play an important role in regulating the blood calcium levels and operate to restore the correct levels by removing excess calcium from the blood. Over a prolonged period of time excess calcium can accumulate and form kidney stones. Small stones may be passed in the urine without you noticing but larger stones may get stuck. These can cause pain in your loin area that radiates to your groin. You may also notice blood in your urine. Kidney stones can be very painful. Continual high levels of calcium in your blood can damage your kidneys and eventually can cause kidney failure.
Weakened bones
Increased parathyroid hormone (PTH) in your blood causes too much calcium to be released from your bones, which can lead to weakness and bone pain. This can eventually cause osteopenia and osteoporosis. It also makes the bones more susceptible to fractures. If bones break after a low impact fall it may be indicative of primary hyperparathyroidism.
Left untreated, many patients with primary hyperparathyroidism have progressive loss of cortical bone while successful surgery leads to a substantial increase in bone mineral density, an effect that can persist for up to 15 years 10).
Eyes
Calcium can be collect in the cornea of your eye (corneal calcifications) but this doesn’t usually cause any symptoms.
Pancreas
Although it is rare, high calcium can cause inflammation of your pancreas and this causes upper abdominal pain (pancreatitis).
Stomach
High calcium levels can stimulate the production of excess acid in your stomach and lead to peptic stomach ulceration.
Brain
Calcium plays an important role in the normal working of the brain and spinal cord. Patients whose primary hyperparathyroidism goes undiagnosed for a long time and who therefore suffer from hypercalcemia over a long period of time, may develop some of the following symptoms: fits, uncoordinated muscles (affecting walking, talking and eating), changes in personality and/or hallucinations.
Pediatric hyperparathyroidism diagnosis
The subtle nature of the symptoms of hyperparathyroidism can result in the condition going undiagnosed for some time, although the diagnosis of hyperparathyroidism is generally clear once appropriate tests are done.
The key to diagnosis is to check the level of calcium in the blood and at the same time to measure the levels of parathyroid hormone (PTH) and vitamin D. These three elements interact with each other and it is the relationship between them that is important in reaching a diagnosis.
Blood tests
- total calcium
- parathyroid hormone (PTH)
- vitamin D (25 OH cholecalciferol)
In a straightforward case, blood tests will show a high level of calcium, a high level of parathyroid hormone (PTH) and often (though not always) a low level of vitamin D in your blood. Phosphate levels may also be low. Elevated PTH is the only source in primary hyperparathyroidism.
Once doctors diagnose hyperparathyroidism, a 24-hour urine collection can help find the cause. This test measures certain chemicals, such as calcium and creatinine, a waste product that healthy kidneys remove. You will collect your urine over a 24-hour period and your health care professional will send it to a lab for analysis. Results of the test may help tell primary hyperparathyroidism from hyperparathyroidism caused by a kidney disorder. The test can also rule out familial hypocalciuric hypercalcemia, a rare genetic disorder, as a cause.
However, sometimes diagnosis is more difficult. Your tests may be normal (within the reference range) or levels not especially high, but you may still be experiencing symptoms. This can lead to a doctor determining you to be a ‘mild case’ and deciding to monitor you for a while – the practice of ‘watch and wait’ that some doctors adopt can lead to much distress.
In addition to a complete medical history and physical examination, diagnostic procedures for hyperparathyroidism may include:
- Bone X-rays. A diagnostic test that uses invisible electromagnetic energy beams to produce images of internal tissues, bones, and organs onto film.
- Laboratory tests. The tests will measure calcium, phosphorus, magnesium, and hormone levels.
- Ultrasonography. A procedure that evaluates the structure of the parathyroid gland using sound waves recorded on an electronic sensor.
- Nuclear medicine tests. These include Sestamibi and other scans that use small amounts of radioactive materials to evaluate how a parathyroid gland is functioning and to help diagnose problems.
- Computed tomography scan (also called a CT or CAT scan). A diagnostic imaging procedure that uses a combination of X-rays and computer technology to produce horizontal, or axial, images (often called slices) of the body. A CT scan shows detailed images of any part of the body, including the bones, muscles, fat, and organs. CT scans are more detailed than general X-rays.
- Magnetic resonance imaging (MRI). A diagnostic procedure that uses a combination of large magnets, radiofrequencies, and a computer to produce detailed images of organs and structures within the body.
Pediatric hyperparathyroidism treatment
Specific treatment for hyperparathyroidism will be determined by your child’s doctor in consultation with you.
Considerations include:
- Your child’s current health status and past health history
- Severity of the condition
- Your child’s ability to take medications and tolerate medical procedures
- Expectations for the course of the disease
- Your beliefs and concerns
Treatment often includes surgery to remove the parathyroid tissue, but sometimes your child may be monitored or offered medical treatment, depending on your child’s circumstances. Medical treatment with bisphosphonates or cinacalcet can be useful in selected patients 11). The decision whether to recommend surgery is based on age, the degree of hypercalcemia, and the presence or absence of complications due to hyperparathyroidism.
Some patients who are not surgical candidates may benefit from medical management of primary hyperparathyroidism.
- Bisphosphonates can increase bone mineral density in those with osteoporosis or osteopenia.
- Agonists to the calcium-sensing receptor, such as cinacalcet will lower PTH and calcium levels. Cinacalcet is a medicine that decreases the amount of PTH the parathyroid glands make and lowers calcium levels in the blood. Doctors may prescribe cinacalcet to treat very high calcium levels in people with primary hyperparathyroidism who can’t have surgery. However, they do not increase bone density 12). If you have bone loss, your doctor may prescribe alendronate or other medications to help increase bone density.
For patients where observation is the selected course of action, periodic monitoring with measurement of serum and urine calcium, renal function, and bone densitometry is required. If there is worsening hypercalcemia or development of complications, then surgery should be recommended 13).
Surgery
Surgery is the treatment of choice for those with recurrent kidney stones.
The only cure for primary hyperparathyroidism is surgery to remove the affected parathyroid gland(s) and usually brings about a permanent cure. This operation is called a parathyroidectomy. In the hands of an experienced surgeon the success rates are high, particularly if the affected gland(s) can be located by preoperative scans. However, very often scans are negative or inconclusive. A skilled surgeon will not necessarily regard this as an obstacle to going ahead with surgery.
The current guidelines state that surgery should be recommended for asymptomatic primary hyperparathyroidism when 14):
- Serum calcium is more than 1 mg/dL greater than the upper limit of normal
- Age younger than 50 years
- Osteoporosis
- GFR less than 60 mL/min
- Urine calcium greater than 400 mg/24 hours
- Evidence of renal calcification or stones
Most commonly one, or at most two, parathyroid adenomas are removed. However, all abnormal parathyroid glands may need to be removed if all four parathyroid glands are overactive, as in the rarer condition of parathyroid hyperplasia. In this case it may be possible to leave half a parathyroid gland in situ to avoid developing hypoparathyroidism, a lifelong condition, but this is not always possible. It is essential to discuss your treatment plan with your surgeon.
Parathyroid surgery is normally a straightforward procedure most often requiring an overnight hospital stay for recovery. For removal of a single adenoma, most surgeons are able to perform minimally invasive surgery via a small incision which, after healing, leaves a barely visible scar.
Surgeons often use imaging tests before surgery to locate the overactive gland or glands to be removed. The tests used most often are sestamibi, ultrasound, and CT scans. In a sestamibi scan, you will get an injection, or shot, of a small amount of radioactive dye in your vein. The overactive parathyroid gland or glands then absorb the dye. The surgeon can see where the dye has been absorbed by using a special camera.
Surgeons use two main types of operations to remove the overactive parathyroid gland or glands:
- Minimally invasive parathyroidectomy. Also called focused parathyroidectomy, surgeons use this type of surgery when they think only one of the parathyroid glands is overactive. Guided by a tumor-imaging test, your surgeon will make a small incision, or cut, in your neck to remove the gland. The small incision means you will probably have less pain and a faster recovery than people who have more invasive surgery. You can go home the same day. Your doctor may use regional or general anesthesia during the surgery.
- Bilateral neck exploration. This type of surgery uses a larger incision that lets the surgeon find and look at all four parathyroid glands and remove the overactive ones. If you have bilateral neck exploration, you will probably have general anesthesia and may need to stay in the hospital overnight.
Parathyroid surgery is safe. Rarely, problems can occur after surgery. In about 1 out of every 100 people, the nerves controlling the vocal cords are damaged during surgery, which most often results in hoarseness 15). This condition usually gets better on its own.
Low calcium levels in the blood may occur after surgery but usually return to normal in a few days or weeks. On rare occasions, not enough parathyroid tissue is left to make PTH, which can result in hypoparathyroidism.
Should I change my diet if I have primary hyperparathyroidism?
You don’t need to change your diet or limit the amount of calcium you get from food and beverages. You will need to take a vitamin D supplement if your vitamin D levels are low. Talk with your health care professional about how much vitamin D you should take.
If you lose all your healthy parathyroid tissue and develop lasting low-calcium levels, you’ll need to take both calcium and vitamin D for life.
Monitoring
Some people who have mild primary hyperparathyroidism may not need surgery right away, or even any surgery, and can be safely monitored.
You may want to talk with your doctor about long-term monitoring if you
- don’t have symptoms
- have only slightly high blood calcium levels
- have normal kidneys and bone density
Long-term monitoring should include regular doctor visits, a yearly blood test to measure calcium levels and check your kidney function, and a bone density test every 1 to 2 years.
If you and your doctor choose long-term monitoring, you should
- drink plenty of water so you don’t get dehydrated
- get regular physical activity to help keep your bones strong
- avoid certain diuretics, such as thiazides
References [ + ]





{kind=link}