Contents
Vocal cord cysts
Vocal cord cysts sometimes referred to as vocal fold cysts are benign growths that have a sac around a fluid-filled or semisolid center. Vocal cord cysts are less common than vocal cord nodules and polyps. Vocal cord cysts are not typically associated with overuse of the voice or vocal fold trauma. Vocal cord cysts can also be caused by using the voice while one is sick with an upper respiratory infection or laryngitis.
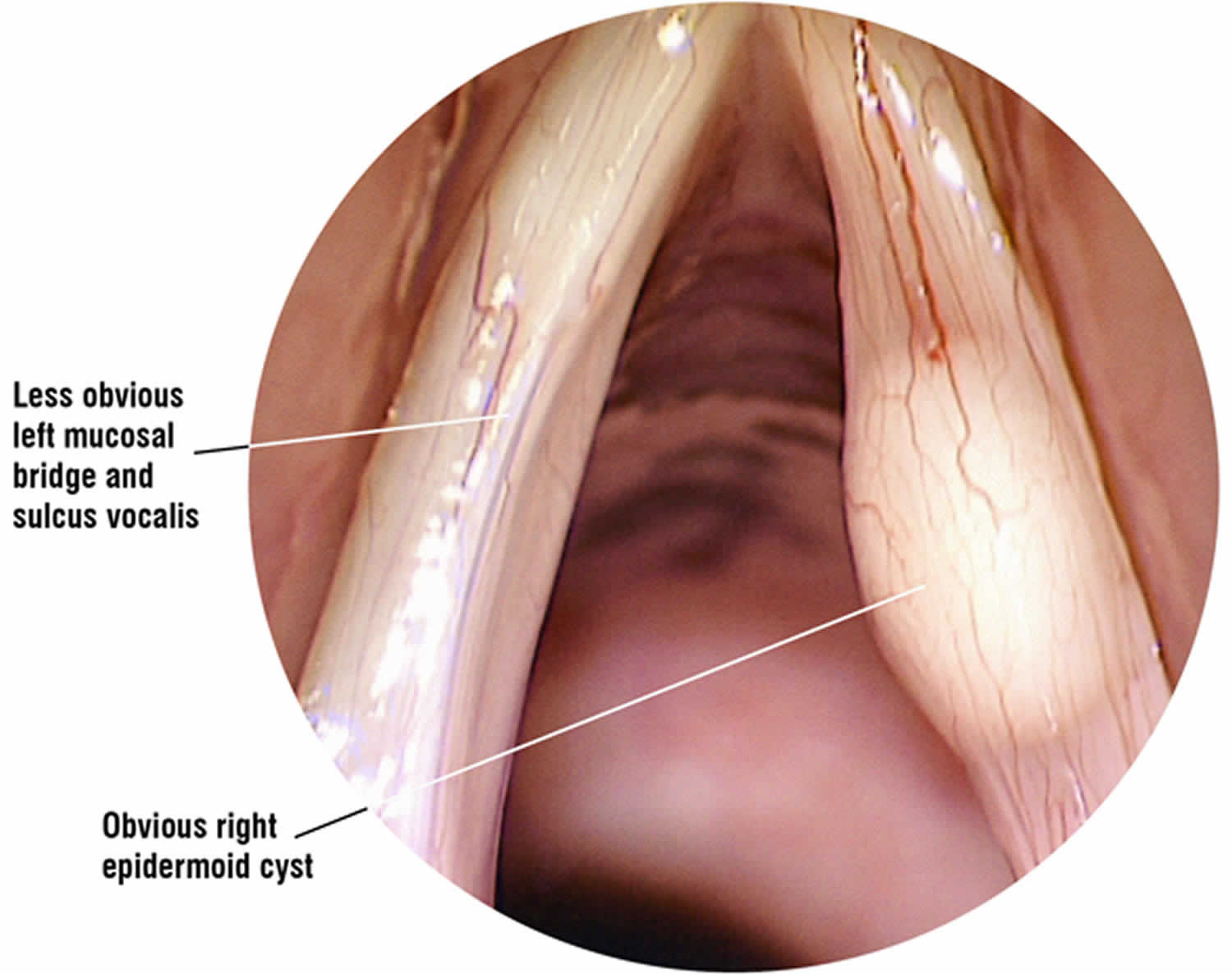
There are basically two types of cyst that can occur on the vocal folds or ‘vocal cords’. Probably the most common is the mucus retention cyst, which develops when the duct of a small mucus producing gland becomes blocked forming a closed sac that fills with fluid or a semi-solid material. The origins of other vocal cord cysts, known as epidermoid (or sebaceous) cysts, that appear inside the layers of the vocal fold are less well understood. They tend to be more solid in nature than retention cysts and they are usually long standing, possibly even congenital (present at birth). Often they are more difficult to spot without specialist equipment as they are not necessarily visible with routine examination techniques. Patients with epidermoid cysts often report that they have always had a deeper than average voice, even as a child. However, they may not be aware of any real vocal difficulties until the vocal load is increased should they, for example, become a singer, actor or teacher.
Occasionally a vocal cord cyst will burst, discharging its contents but leaving a small strip of remnant mucous membrane (vocal fold lining) that was once part of the cyst roof. These are referred to as mucosal bridges. Unfortunately, beneath them usually lies the scarred floor of the cyst, which is deeply adherent to the underlying ligament, leaving an area of vocal fold that cannot vibrate.
Patients with identifiable vocal cord cysts or extensive scarring will usually require surgery with follow up speech therapy to try and reduce the chance of post operative scarring.
Recent advances in surgical technique (phonosurgery) mean that vocal cord cysts can be removed and scars can be modified, either resolving or improving the vocal symptoms. It is important to choose a voice specialist laryngologist who is familiar with phonosurgical techniques. Vocal cord cysts frequently respond well to surgical removal and the results are generally good. Occasionally they can recur, so it is important to attend a review appointment with your laryngologist and to return and see them again should your symptoms recur.
Your surgeon will explain your diagnosis and discuss, as honestly as they can, what they plan to do at surgery and the possible outcomes. Unfortunately, examination in the voice clinic, even with specialist equipment, may only tell the surgeon that there is an area of vocal fold stiffness. It will not necessarily determine what is causing it. The nature of the problem and its full extent may only be discovered at the time of surgery, making it very difficult for the surgeon to be accurate in either the outpatient diagnosis or outcome prognosis.
Many surgeons will refer you to speech therapy at the time you are placed on the waiting list for surgery. It is important that you make contact with the therapist as soon as you know your surgery date so that they can arrange a timely appointment for you. Usually, the sooner you receive therapy the faster you can begin to develop good vocal technique again. The aim of post operative voice therapy is to resolve any remaining compensatory muscle tension and to shake loose stiffness that is a normal part of post operative healing.
Figure 1. Vocal cord cyst
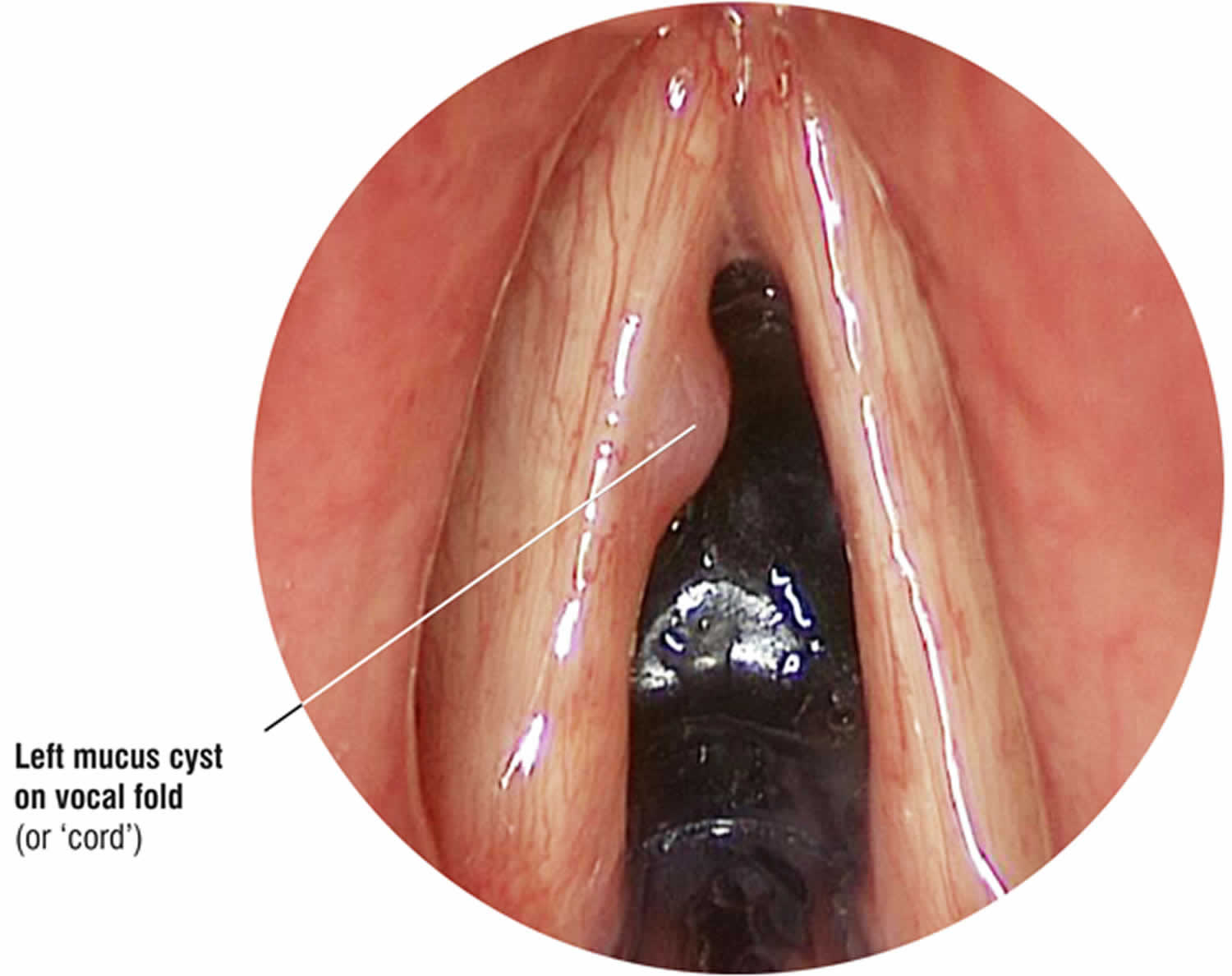
Figure 2. Vocal fold cyst (epidermoid cyst)
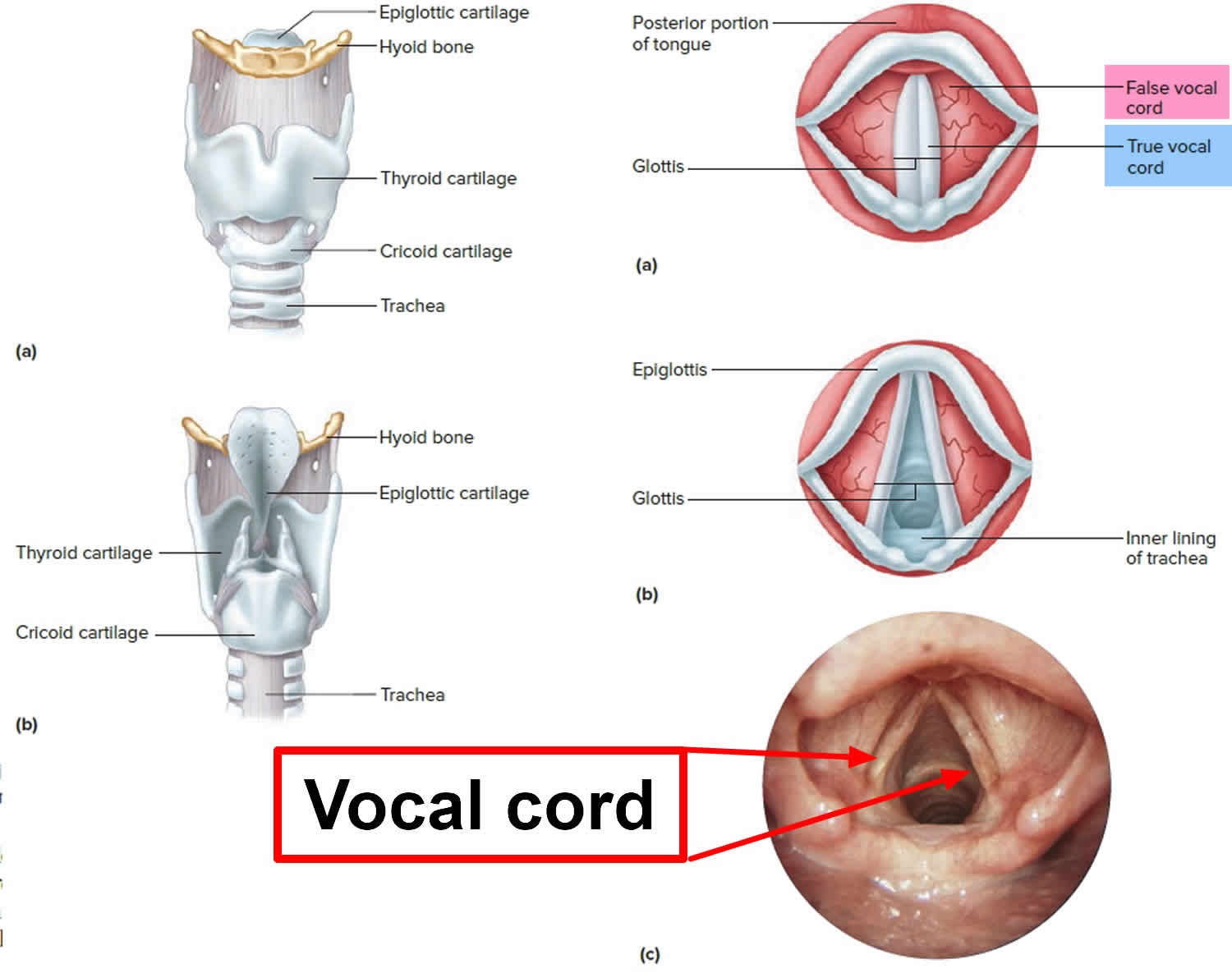
Vocal cord anatomy
The vocal fold is composed of a muscle covered by a free mucosal edge that vibrates and can be separated into discrete layers in which various types of pathology may develop. Each layer has distinct mechanical properties and can be differentiated by the concentration of elastin and collagen fibers in a 3-dimensional layered structure parallel to the leading edge.
Histologically, the vocal fold is a complex structure. The delicate arrangement of the extracellular matrix proteins within the lamina propria permits passive movement of the epithelium, or vocal cover, over the body, resulting in the formation of the mucosal wave as air is passed through the glottis as a release of building subglottic pressure. Most benign lesions occur in the superficial layer of the lamina propria; therefore, surgical approaches to benign lesions should ideally be confined to this layer. Benign lesions are usually superficial to the vocal ligament and the thyroarytenoid muscle.
Figure 3. Larynx and pharynx anatomy
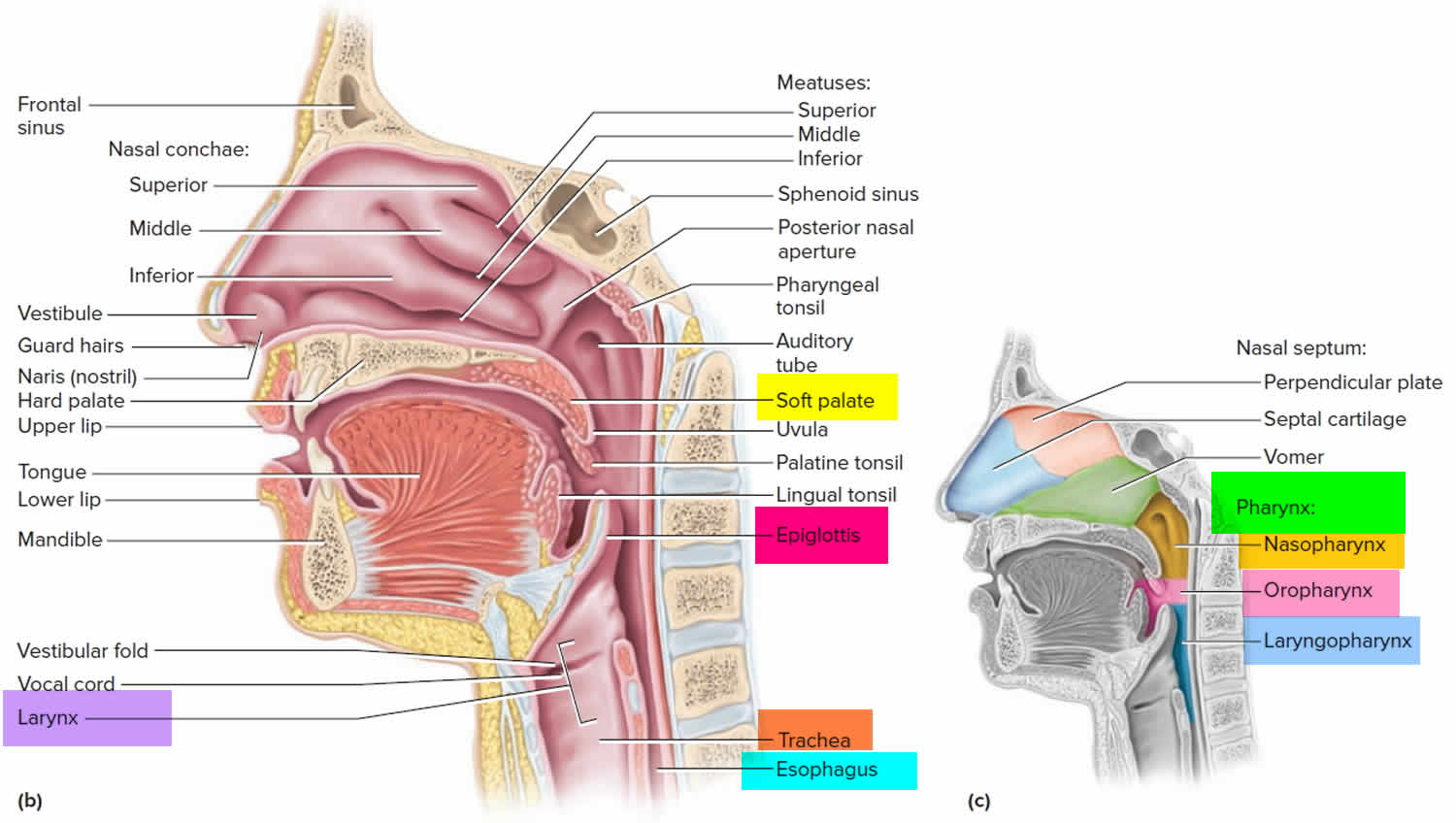
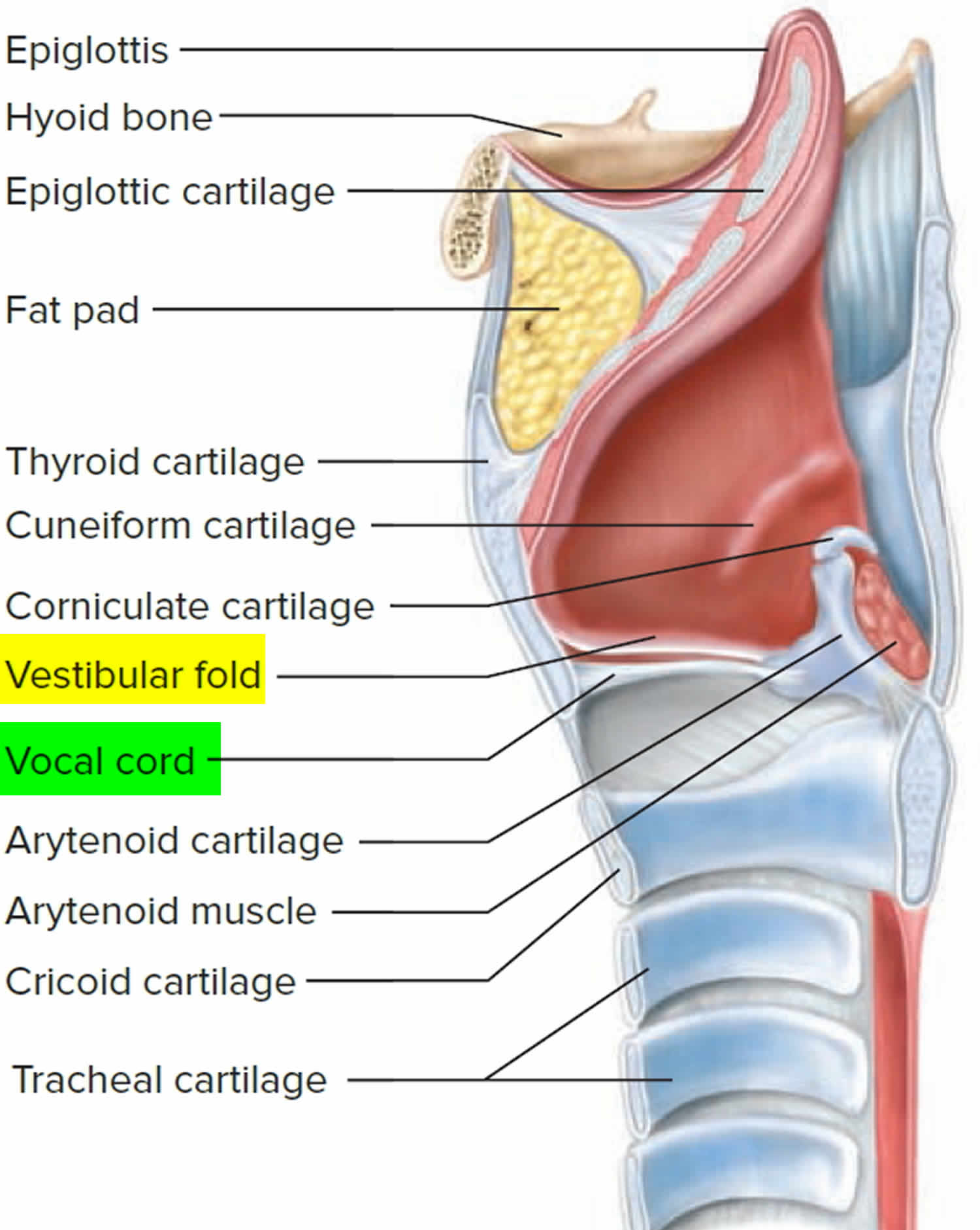
Figure 4. Vocal cord anatomy (vocal fold anatomy)
Vocal cord cyst causes
Vocal cord cysts can develop in several ways:
- In utero, while a baby’s vocal cords are developing
- From abuse or misuse of the voice (including straining, yelling and frequent singing)
- Mucous becomes trapped in the glands in the voice box (similar to a pimple)
Repeated trauma from vocal misuse or overuse may lead to the development of vocal fold nodules, polyps, or cysts. Mucus retention cysts may occur secondary to ductal obstruction, and epidermoid cysts may occur from congenital cell rests or from healing injured mucosa. A focal thickening may also form as a reaction to trauma caused by the cyst on the contralateral cord. Benign lesions are found within the lamina propria and cause dysphonia by disrupting the vibratory pattern and close approximation of the true vocal folds.
Epidermoid cysts may occur secondary to vocal abuse and overuse or may be secondary to a remnant of epithelium trapped within the lamina propria 1). Mucus retention cysts may occur spontaneously or may be associated with poor vocal hygiene. They are presumed to arise from an obstructed mucus-producing gland. As the cyst enlarges, it can start to significantly affect the vibratory region of the vocal fold.
A study by Hanshew et al 2) suggested that Streptococcus pseudopneumoniae and, possibly, Pseudomonas, may play a role in the etiology of benign vocal fold lesions, such as cysts, nodules, polyps, and Reinke edema. The investigators found the bacterial communities of 31 out of 44 such lesions to be dominated by Streptococcus pseudopneumoniae, unlike the microbiota found in healthy saliva and throat samples. Twelve of the remaining 13 lesions contained Pseudomonas, which was not seen in the healthy samples.
Vocal cord cyst symptoms
The symptoms of a vocal cord cyst include hoarseness, straining, breathiness, pitch limitations, multiple tones, loss of vocal range, vocal fatigue or loss of voice and sometimes pain when trying to speak or sing. Gastroesophageal reflux disease (GERD) can worsen symptoms.
Singers commonly report abrupt loss of voice or break at a certain pitch. Generally, patients with intracordal lesions have dysphonia that becomes more severe with use. They may also describe periods of aphonia following vocal overuse. Sometimes a vocal fold cyst can affect only the singing voice and not the speaking voice or have little or no effect on voice quality. In the latter situation, no indication exists for treatment. However, for a patient to have a normal speaking and singing voice is not unusual, and a patient may be able to perform. When a patient reports complete aphonia, a significant functional component can be expected. Cysts rarely cause symptoms of stridor, aspiration, globus sensation, or dysphagia.
Vocal cord cyst diagnosis
The diagnosis of vocal cord cysts is made by laryngoscopy or stroboscopy, tests that examine the voice box.
- Laryngoscopy: A doctor will place a spaghetti-like camera in your child’s nose and down the throat. This allows our team to look at your child’s voice box, or larynx.
- Stroboscopy: A small, thin, flexible endoscope with a camera is gently inserted through the nose to the area in the back of the throat above the vocal cords. The study evaluates the motion of your child’s vocal cords when there are concerns regarding the strength, pitch and quality of his voice. If there is decreased vibration (stiffness) and a lesion is seen on the vocal cord, it is suggestive of a cyst. Despite the excellent visualization provided by videostroboscopy, it cannot replace direct laryngoscopy and palpation of the lesion as the criterion standard in diagnosis and should not be considered a substitute, especially in patients in whom a neoplastic process is possible.
Most of the time, these exams can be done while your child is awake and in an office setting.
Occasionally, when not obviously noted in the office, cysts may be diagnosed by microlaryngoscopy and/or a vocal cord palpating tool while under anesthesia in the operating room.
Vocal cord cyst treatment
Vocal cord cysts are usually treated by complete surgical excision. Unlike vocal cord nodules, vocal cord cysts will not go away with conservative methods (such as voice therapy) but the voice can be improved somewhat using these methods, delaying the need for surgery.
Medical management of possible reflux and allergies, as well as proper use of the voice are important as they can reduce reactive damage to the opposite vocal fold, and may help prevent future lesions by minimizing voice abuse.
In singers, surgery is indicated when the accustomed performance style or required schedule cannot be maintained, for recurrent disabling periods of dysphonia, or for intolerable vocal strain and fatigue. These requirements must be assessed on an individual basis since some performers are able to sing infrequently enough to prevent significant problems.
Vocal cord cyst surgery
Although nodules and polyps may respond to conservative management, vocal cysts typically do not. Delay in surgical treatment and continued trauma can potentially lead to progression of cyst formation and intracordal scarring.
The goal of surgical excision is preservation of the mucosal cover with minimal disruption of the underlying tissue. In addition, the deep layers of the lamina propria harbor fibroblasts that produce extracellular proteins. Avoid this layer to prevent scarring along the vocal ligament and tethering of the mucosal cover. The microflap approach to the excision of benign laryngeal lesions was developed with these goals in mind.
A study by Jensen and Rasmussen 3) indicated that microscopic phonosurgery is an effective treatment for benign vocal fold lesions, including cysts. The study included 97 patients who underwent the surgery for vocal fold polyps, cysts, nodules, or edema, with data from postoperative clinical evaluation available for 89 of these individuals. In 85% of the patients, postoperative voice quality was reported to be unaffected, while in 13% of patients, voice quality was improved but moderately affected, and in one patient, with a cyst and sulcus vocalis, voice quality was severely affected.
Diagnostic direct microlaryngoscopy should be considered when the diagnosis of vocal fold cyst is uncertain or when a neoplastic process cannot be excluded.
A retrospective study by Tibbetts et al 4) found that in patients who underwent microflap excision of vocal fold cysts—including 19 with mucus retention cysts and two with epidermal inclusion cysts—improvement in Voice Handicap Index–10 scores did not differ significantly between individuals who were treated with postoperative voice therapy and patients who were not.
Intraoperative details
The lateral microflap is used when the lesion is adherent to the vocal ligament and the overlying mucosa is normal. The advantage of the lateral microflap is that the incision and the subsequent scar are lateral to the medial surface of the vocal fold. In addition, the uninvolved portion of the vocal ligament may be used to orient the flap, and dissection may proceed from known to unknown. The medial microflap is indicated for lesions that involve a discrete portion of the vocal fold and appear to separate easily from the underlying vocal ligament on palpation. This approach allows for a shorter flap and can be used to treat redundant or adherent mucosa overlying a lesion. At the conclusion of the procedure, a solution of triamcinolone acetate may be injected into the flap. This is thought to further minimize scar formation. With both techniques, most patients experience return of mucosal wave and are satisfied with voice quality.
Results with the microflap have been excellent, with return of good-to-excellent voice and mucosal wave in most patients. Use of the laser in the surgical treatment of benign nodules, polyps, or cysts to minimize scar formation is minimal.
Postoperative details
Place the patient on strict voice rest for 2 weeks after microflap surgery. Patients with more extensive dissections may be placed on a short course of corticosteroids. Administer a 7-day course of antibiotics and a mild narcotic for pain relief to all patients. Treat patients with symptoms or findings of laryngopharyngeal reflux with a proton-pump–inhibiting agent.
Complications
Complications are related either to laryngoscopy or to vocal fold mucosal injury. Pressure effects from suspension laryngoscopy may result in tongue numbness, altered taste, and oropharyngeal, mucosal, and dental injuries. Deep-plane dissection or exposure of the vocal ligament can result in scarring and fibrosis of the mucosa with loss of mucosal wave and glottal insufficiency. Injudicious use of the laser can result in a wide zone of thermal damage with mucosal scarring and fibrosis, unintended burn injuries, and endotracheal tube fires. The best way to treat scarring is to prevent it. Use of microflap techniques avoids a raw mucosal surface that heals by secondary intention. Avoidance of the deeper layers of the lamina propria and vocal ligament minimizes the fibroblastic response.
Follow-up care
If voice therapy is recommended, the initial follow-up will be about three months after beginning the therapy in order to assess progress and response. If reflux management is recommended, then a three-month follow-up in clinic may be recommended as well. If there is no response to voice therapy and/or medical therapy, then a surgical intervention may be recommended. The follow-up after surgery will include voice therapy with your child’s speech pathologist, return to clinic about one month post-surgery and then about three months, six months and 12 months later.
At the 2-week postoperative visit, perform videostroboscopy and have the patient resume therapy with the speech pathologist. A gradual return to voice use occurs over the first few weeks, increasing by 5-minute intervals twice daily. Singers may begin to work with the vocal pedagogue (ie, singing teacher) at 1 month, but they are cautioned to decrease vocal work if they feel any discomfort or strain. Most patients can expect 90% of their functional surgical result at approximately 3 months.
Vocal cord cyst prognosis
When a vocal cord cyst is completely removed, the outlook is good, as long as the voice is cared for with voice therapy and proper use of the voice. Scarring from surgical removal of the cyst is a risk, and while unusual, it can cause persistent voice problems.
There is a risk of cysts rupturing on their own if they are not removed, which can also lead to scarring.
Courey et al 5) found that 85% of patients with an absent wave preoperatively regained their mucosal wave, while 97% percent of patients with an intact preoperative wave retained this important parameter. Blinded comparison of preoperative and postoperative voice samples from this series showed that the postoperative voice was rated as better in 100% (48 of 48) of patients. Although long-term results in these patients remain excellent, continued emphasis should be placed on the prevention of pathology (eg, voice training, good vocal hygiene, maintenance of systemic health).
References [ + ]





{kind=link}