Contents
Megaureter
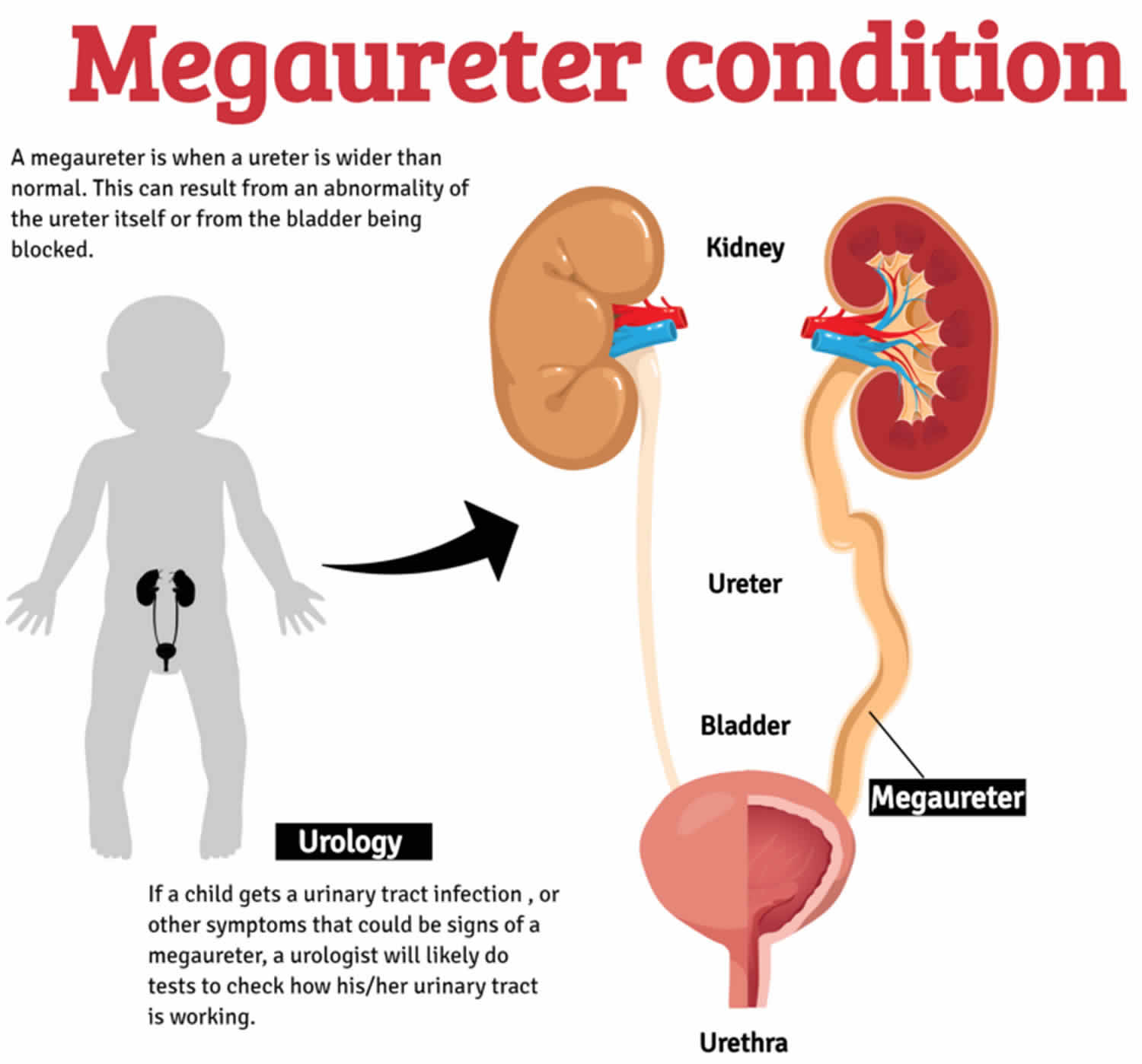
Megaureter is a descriptive term for dilated ureter or “large ureter”, which is an expanded or widening of one or both of the ureters of a child that does not function normally. Ureters are the two funnel-shaped tubes that carry urine from the kidneys to the bladder (Figure 1). Whereas a normal ureter is about 3-5 mm, the size of a megaureter is usually greater than 10 millimeters (three-eighths of an inch) in diameter. This can result from an abnormality of the ureter itself (primary megaureter) or from the bladder being blocked (secondary megaureter). The different types of megaureters are described below.
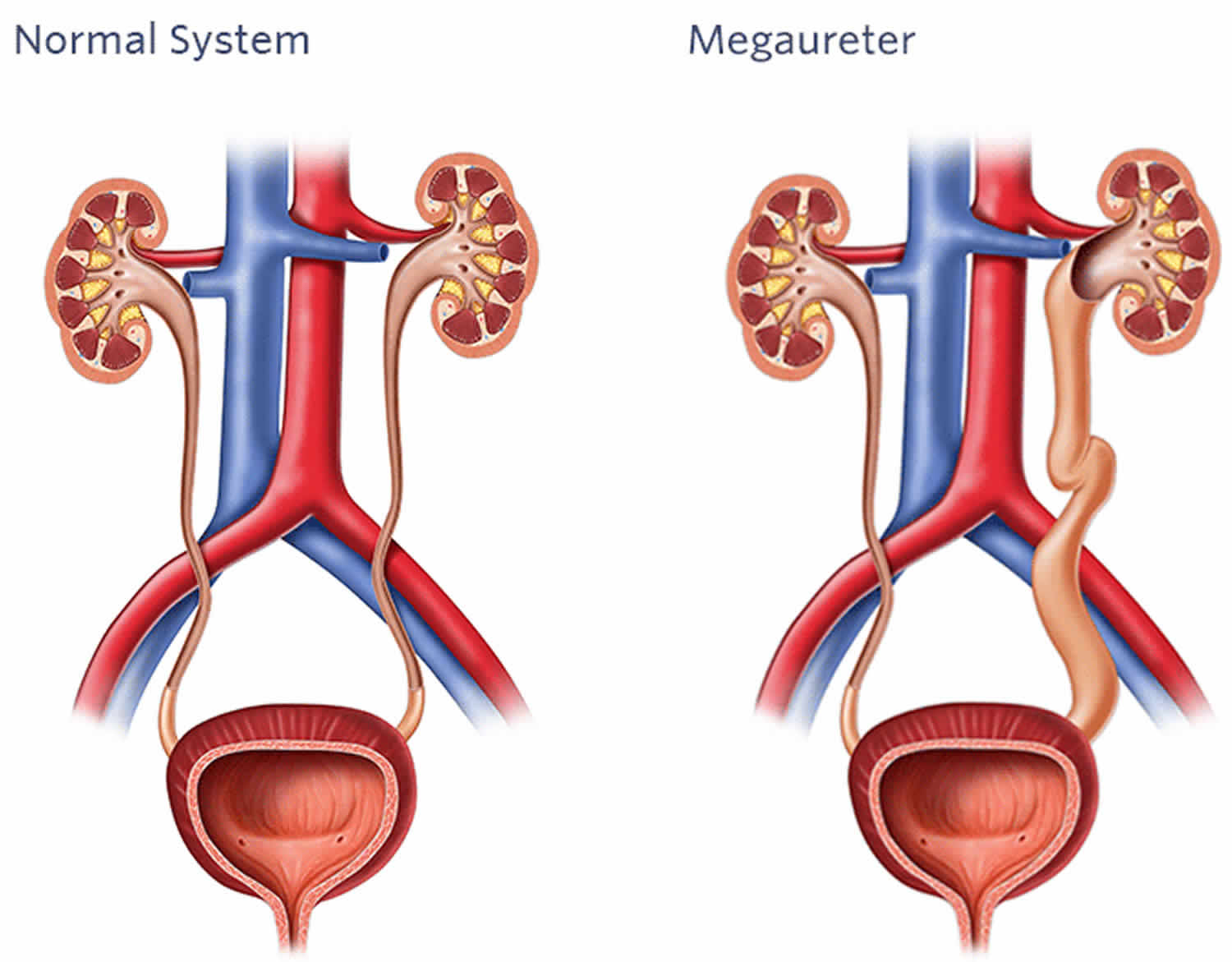
The two important questions about megaureter are whether there is reflux (backwash) of urine causing the megaureter or whether there is blockage at the ureterovesical junction causing megaureter (Figure 2). If there is reflux, the diagnosis is “refluxing megaureter” or “megaureter from reflux”. If there is obstruction, the diagnosis is “obstructed megaureter” or “primary obstructed megaureter”. If there is neither reflux or obstruction, then the diagnosis is “primary non-obstructed megaureter”. In very rare circumstances, there can be reflux and obstruction and the diagnosis is “refluxing obstructed megaureter”. The two most common types of megaureter by far are the “primary non-obstructed megaureter” and the “refluxing megaureter”.
Complications associated with megaureter include reverse flow (or reflux) of urine into the kidneys and pooling of urine inside the ureter that does not drain due to blockage. The pooling can cause a child to develop a urinary tract infection. In some children, complications from megaureter can cause kidney damage and failure.
Despite worldwide availability of prenatal ultrasound, many patients with a congenital megaureter are not diagnosed until adulthood 1). Adult primary obstructive megaureter is usually a symptomatic condition and is related to high complication rates, including infections, stone formation, and renal failure 2). Spontaneous resolution is rare and prompt surgical management is advocated 3).
Megaureters are treated differently based on their cause. If there is reflux causing the megaureter, then it is treated with prophylactic antibiotics and occasionally endoscopic or open surgery as appropriate (please see section on vesicoureteral reflux).
If there is obstruction or partial obstruction causing the megaureter at the ureterovesical junction then several factors are considered when recommending treatment. If the kidney with the obstructed or partially obstructed megaureter has decreased function, or there are recurrent urinary tract infections, then a ureteral reimplant (see section on ureteral reimplantation) with removal of the blockage (Figure 1) is recommended. However, if the obstructed or partially obstructed megaureter is not causing symptoms and the kidney is functioning fine, then surgery can often be avoided since the obstruction may resolve over time and the megaureter may go away.
If there is no obstruction and no reflux, the vast majority of these types of megaureters resolve with time and only periodic ultrasounds are performed to assess kidney growth.
Most patients with megaureter will receive prophylactic antibiotics until the megaureter goes away on its own, potty training is completed, or in the cases where surgery is performed, after the surgery is completed.
Figure 1. Ureter
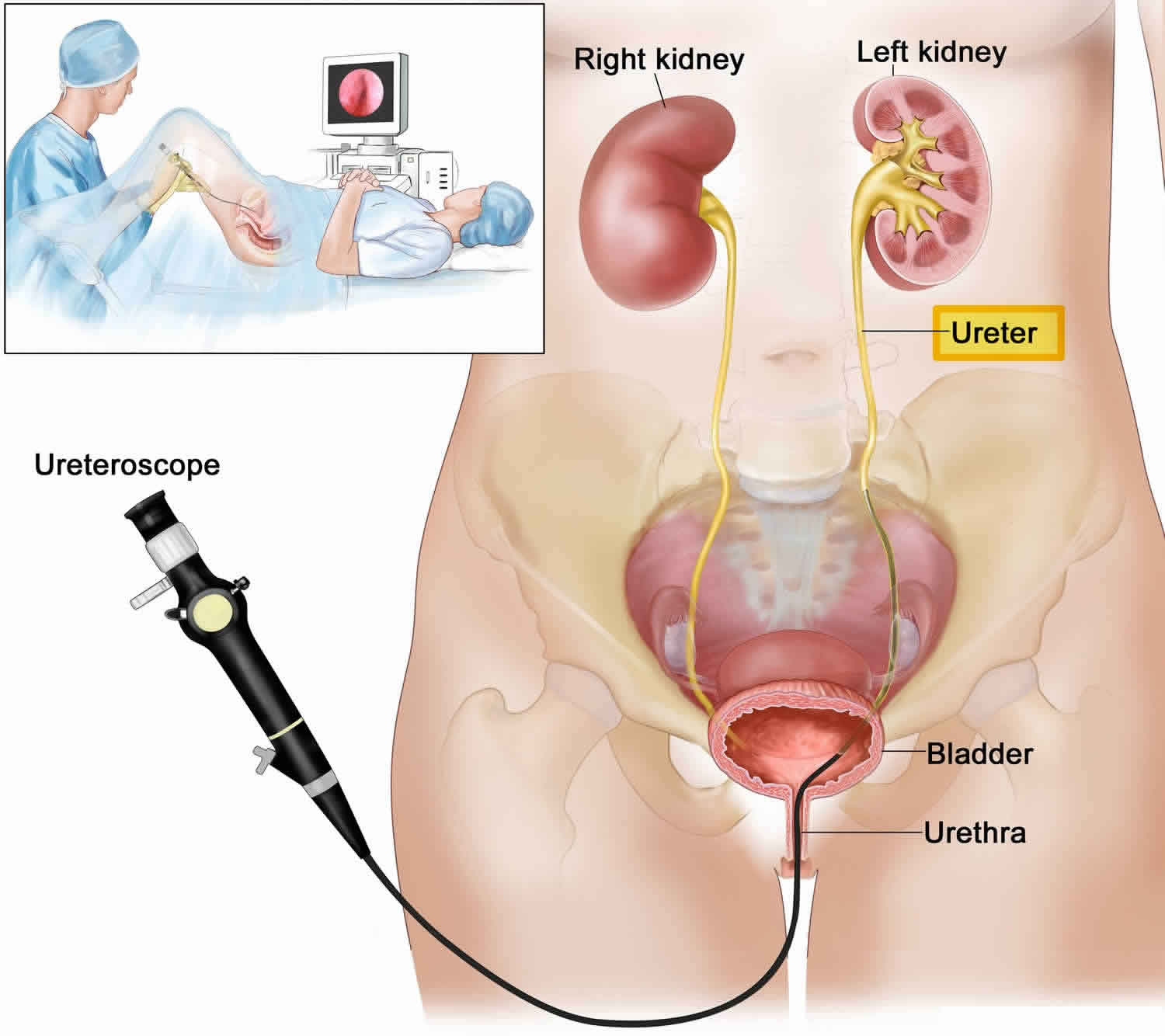
Figure 2. Megaureter
Normal urinary system
The urinary tract is like a plumbing system, with special ‘pipes’ that allow water and salts to flow through them. The urinary tract is made up of 2 kidneys, 2 ureters, the bladder, and the urethra.
The kidneys act as a filter system for the blood. They remove toxins and keep the useful sugar, salts, and minerals. Urine, the waste product, is made in the kidneys and flows down 2, 10 to 12-inch-long tubes called ureters into the bladder. The ureters are about a quarter inch wide and have muscled walls which push the urine into the bladder. The bladder stretches or expands to store the urine until you’re ready to drain it by peeing. It also closes the pathways into the ureters so urine can’t flow back into the kidneys. The tube that carries the urine from the bladder out of the body is called the urethra.
How is megaureter treated?
- Most patients require no intervention and patients can outgrow this over time.
- Surgery may be needed for megaureters that do not resolve with time, that have had a worsening in dilation, or have developed infections. In such cases, ultrasound testing is done on a regular schedule to make sure the kidneys keep working normally.
- Initial treatment of megaureters of all types usually includes the use of antibiotics to treat and to reduce the chance of urinary tract infections.
- When kidney function is affected, open surgery (requiring an incision) is the preferred treatment method. Surgery is used to reconnect ureters to the bladder, to narrow down widened ureters, or to remove blockages that may be present.
- If it is possible to do so without risking kidney damage or infection, surgery can be delayed until a child is at least one year old in order to reduce some of the risks of operating on a very young child.
- Another treatment option in children over two years old is balloon dilation. A long, thin telescope with a light at the end is placed into the bladder and up the ureter. A balloon is inflated to stretch the narrowed part of the ureter and then a silicone tube is put in place for four to six weeks to expand the tissue.
Left untreated, megaureter can lead to infections, blocked flow of urine, and possibly serious damage to the kidneys.
Is surgery always needed to fix a megaureter?
No. Most megaureters found before birth get better over time without needing surgery. Megaureters found in older patients with pain or infection are more likely to need surgery. Antibiotics are often given to prevent urinary tract infection.
Is minimally-invasive surgery an option?
It may be possible to place a stent or catheter through the blocked part of the megaureter as a short-term fix to help the kidney drain. Laparoscopic techniques to fix megaureters are being explored.
Why are megaureters treated?
Regardless of the cause of megaureter (reflux or obstruction), megaureters are treated to prevent urinary tract infection and possible kidney damage. Both reflux and obstruction can lead to kidney damage, especially in the setting of urinary tract infections. Prophylactic antibiotics may be given because of the increased risk of urinary tract infection. Surgery may be required as well (see section on surgery below).
Are there long-term problems to megaureter if I don’t do anything?
Possibly yes. They include:
- ureteral stones
- urinary tract infection
- kidney function getting worse
- back pain.
Megaureter types
There are two main types of megaureter:
- Refluxing megaureter: In this type, the urine flows back up the ureter from the bladder. This backflow, known as vesicoureteral reflux, expands the ureter.
- Primary obstructed megaureter: The ureter is too narrow where it enters the bladder, causing a blockage of urine flow at that point.
There are also combinations of the two main types:
- Primary non-obstructed, non-refluxing megaureter: This occurs when there is neither reflux nor obstruction.
- Refluxing obstructed megaureter: This rare condition occurs when there is both reflux and obstruction.
The 4 categories of megaureters are refluxing, obstructing, refluxing/obstructing, and nonrefluxing/nonobstructing. Each category is further divided into primary or secondary, based on either intrinsic or extrinsic causes for their appearance, as follows:
- Primary obstructed megaureter is most commonly caused by an adynamic juxtavesical segment of the ureter that fails to effectively propagate urine flow.
- Secondary obstructed megaureter occurs usually when ureteral dilatation is the result of a functional ureteral obstruction associated with elevated bladder pressures secondary to posterior urethral valves (PUV) or a neurogenic bladder that impedes ureteral emptying.
- Primary refluxing megaureter is associated with severe vesicoureteral reflux (VUR) that alters ureteral efficiency by ureteral distention. The megaureter-megacystis syndrome is an extreme form of the primary refluxing megaureters in which massive reflux prevents effective bladder emptying because urine is passed back and forth between the ureters and bladder.
- Secondary refluxing megaureter occurs secondary to posterior urethral valves (PUV) or neurogenic bladder when elevated bladder pressures cause decompensation of the ureterovesicular junction (UVJ) (also known as vesicoureteric junction [VUJ]).
- Primary nonrefluxing/nonobstructed megaureter is diagnosed when no evidence of obstruction or reflux can be demonstrated (diagnosis of exclusion).
- Secondary nonrefluxing/nonobstructed megaureter occurs secondary to diabetes insipidus, in which high urinary flow rates may overwhelm the maximum transport capacity of the ureter by peristalsis, or as the result of ureteral atony accompanying a gram-negative urinary tract infection (UTI).
- Primary refluxing obstructed megaureter occurs in the presence of an incompetent vesicoureteric junction (VUJ) that allows reflux through an adynamic distal segment.
The two most common types are refluxing megaureter and primary non-obstructed, non-refluxing megaureter.
Another class of megaureters is known as secondary megaureters. These are caused by health problems that include:
- A blockage in the male urethra
- Prune belly syndrome (the absence of abdominal muscles at birth)
- Neurogenic bladder (a poorly functioning bladder due to damage to the nerves that control the bladder)
Megaureter causes
Megaureter can occur alone, but usually it occurs in combination with other disorders, such as prune belly syndrome.
A megaureter can be associated with the reverse flow of urine (vesicoureteral reflux, VUR). A megaureter can also be associated with an obstruction. The obstruction can either be the result of a ureterocele, or narrowing where the ureter meets the bladder (ureteral vesical junction obstruction).
A megaureter that is not associated with other problems occurs during fetal development. It occurs when a section of the ureter, which is normally a muscular layer of tissue, is replaced by stiff, fibrous tissue. In the absence of a muscular layer, normal peristalsis (worm-like movement of the ureter that propels urine toward the bladder) cannot occur.
The goal with megaureters is to determine which are obstructed, which have the reverse flow of urine, called reflux, and which have both.
Is megaureter genetic?
At this time, scientists don’t know if there are genetic links.
Congenital megaureter
Congenital megaureter also called primary megaureter is an enlarged ureter which are intrinsic to the ureter, rather than as a result of a more distal abnormality; e.g. bladder, urethra (also called secondary megaureter).
Congenital megaureter or primary megaureter includes:
- Obstructed primary megaureter: This type is when the ureter is too thin where it enters the bladder. This block causes the ureter to get wider further up. The narrowing can damage the kidney over time. Surgery may be needed to fix the problem and remove the block. It’s important to follow up with your health care provider even if the symptoms improve.
- Refluxing primary megaureter: Refluxing primary megaureter is a result of an abnormal vesicoureteric junction, which impedes the normal anti-reflux mechanisms. This can be due to a short vertical intramural segment, congenital paraureteric diverticulum, ureterocele with or without associated duplicated collecting system, etc.
- although vesicoureteric reflux (VUR) is a cause of primary congenital megaureter it is usually considered separately
- Non-refluxing unobstructed primary megaureter: These are wide ureters that aren’t caused by blockage or urine backflow. Many of these get better with time. Your health care provider will check carefully to rule out a block or reflux.
In all three types of megaureter, patients are often asymptomatic. Symptoms, when present, are usually arise from complications due to urinary stasis (e.g. urinary sepsis and nephrolithiasis).
Congenital primary megaureter is sometimes associated with:
- congenital megacalyces 4)
- ipsilateral renal dysplasia 5)
In all three types the ureter is enlarged (>7 mm) sometimes markedly so 6). On all modalities able to visualize the ureter (CT, US, MRI, IVP) it appears as a tubular structure usually posterior to the bladder 7).
Primary megaureter is usually asymptomatic and requiring no treatment. If complications occur or the degree of obstruction is marked then, reimplantation following resection of the aganglionic segment may be performed.
Obstructive primary megaureter
In obstructive primary megaureter the ureter tapers to a short segment of normal caliber or narrowed distal ureter, usually just above the vesicoureteric junction (VUJ). The distal ureter above this narrowed segment is most dilated (similar to achalasia). There is associated hydronephrosis, and active peristaltic waves can be seen on ultrasound.
Obstructive primary megaureter is related to a distal adynamic segment with proximal dilatation and is a common cause of obstructive uropathy in children 8). It is analogous to esophageal achalasia or colonic Hirschsprung disease although a lack of ganglion cells within the wall of the ureter has not been proven to be the cause 9).
Refluxing primary megaureter
In refluxing primary megaureter, vesicoureteric reflux (VUR) is demonstrated. It is relatively common and usually considered separately.
In refluxing primary megaureter, the ureters are wider because of urine flowing back up the ureters from the bladder (“vesicoureteral reflux” [VUR]). Normally, once urine is in the bladder, it shouldn’t go back up the ureters. A refluxing megaureter is a sign of vesicoureteral reflux. This is more common in newborn males. Sometimes the reflux and stretched ureters gets better over the first year of life. But if the problem doesn’t go away, surgery may be needed. Refluxing megaureters may be linked to a health issue where the bladder doesn’t drain all the way. Instead, it sends urine back up the ureters, and the bladder swells. This condition is called “megacystis megaureter syndrome.”
Non-refluxing unobstructed primary megaureter
In non-refluxing unobstructed primary megaureter, there is absent or only a minor degree of hydronephrosis. Although rare, a congenital megaureter may co-exist with congenital megacalyces 1, making the assessment of hydronephrosis more difficult.
This is thought to be the most common cause of primary megaureter in neonates, and even though the vesicoureteric junction is normal, with no evidence of reflux or obstruction the ureter is enlarged. The reason for this is unknown.
Secondary megaureters
These are megaureters that show up as a result of other health problems. Some of these health problems that cause megaureters are:
- posterior urethral valves (a block in the male urethra)
- prune belly syndrome
- neurogenic bladder (spina bifida, spinal cord injury, etc.)
Obstructed refluxing megaureters
This type is caused by a ureter that’s blocked and also suffers from reflux. This is dangerous, as the ureters get bigger and more blocked with time. People with this problem are more likely to get urinary tract infections.
Megaureter symptoms
Each child may experience megaureter symptoms differently. The symptoms of a megaureter may resemble other conditions or medical problems. Always consult your child’s doctor for a diagnosis.
Doctors used to find most megaureters when checking a child with a urinary tract infection (UTI). These patients often have fever, back pain, and vomiting. But today, because of the widespread use of checking with ultrasound before birth, most megaureters are discovered as hydronephrosis or a stretched (“dilated”) urinary tract in the fetus.
Because megaureters can cause severe infection or blocks that lead to kidney damage, this health issue can be serious. Urinary tract stretching may suggest a blockage, but that’s not always the case. In some cases, a dilated ureter may not affect the kidney at all. Also, most patients with megaureters found before birth don’t get symptoms. Also, occasionally flank pain can be seen or there may be blood in the urine. It’s important to have it checked to make sure it won’t affect the way the kidney works and cause problems later.
Megaureter possible complications
Most megaureters found before birth will improve over time without surgery. In older patients with pain or infection, surgery is more likely to be needed.
If nothing is done to correct megaureter, complications can include:
- Formation of stones in the ureter
- Urinary tract infections
- Kidney function that continues to get worse
- Back pain
Megaureter diagnosis
The severity of the megaureter often determines how a diagnosis is made. Often a megaureter is diagnosed by ultrasound while a woman is still pregnant. After birth, some children may have other problems that may suggest the presence of megaureter. Children who are diagnosed later often have developed urinary tract infections that require evaluation by a doctor. If your child gets a urinary tract infection or other symptoms that could be signs of a megaureter, check with your child’s doctor. A urologist will likely do tests to check how his/her urinary tract is working. This may prompt your child’s doctor to perform further diagnostic tests, which may include the following:
- Intravenous pyelogram (IVP). A diagnostic imaging technique that uses an X-ray to view the structures of the urinary tract. An intravenous contrast of dye is given so that the structures can be seen on film. An IVP also reveals the rate and path of urine flow through the urinary tract.
- Voiding cystourethrogram (VCUG). A voiding cystourethrogram (VCUG) is an x-ray test done to look for vesicoureteral reflux. A catheter (hollow tube) is placed in the urethra (tube that drains urine from the bladder to the outside of the body) and the bladder is filled with a liquid dye. X-ray images will be taken as the bladder fills and empties. The images will show if there is any reverse flow of urine into the ureters and kidneys.
- Abdominal ultrasound. Ultrasound, also known as sonography, uses sound waves bouncing off organs in the body to make a picture of what’s inside. This painless imaging test is often done to check how the kidney, ureters, and bladder look. Ultrasound is very good at finding widened ureters. In fact, while sonography rarely picks up normal ureters because of their narrowed size, it makes excellent images of dilated ones.
- Diuretic renal scan (MAG III renal scan). A diagnostic nuclear imaging technique that is conducted by injecting a radioactive fluid into the vein. The radioactive material is then carried to the kidneys where it gives off signals that can be picked up by cameras. Midway during the procedure a diuretic medication is given to speed up urine flow through the kidneys. This helps detect any area of blockage in the urinary tract.
- Magnetic resonance of the urinary tract (MR-U). Magnetic resonance of the urinary tract (MR-U) uses magnetic fields to make pictures of what’s inside the body. This test shows the urinary tract even better than ultrasound or diuretic renal scans. MR-U involves injecting dye and getting pictures of the urinary tract using magnetic fields. This test isn’t often used for small children because it calls for sedation or general anesthesia.
- Blood tests. Tests to assess your child’s electrolytes and to determine kidney function.
Megaureter treatment
Experts have shown that as long as kidney function is not significantly affected and urinary tract infections do not become an issue, some megaureters can be managed medically 10). This may involve the use of antibiotic prophylaxis and radiology observation with repeated ultrasounds. When the dilation is severe without showing signs of improvement, or kidney function is affected, surgical repair may be necessary. Left untreated, megaureter can lead to infections, blocked flow of urine, and possibly serious damage to the kidneys.
Specific treatment for megaureter will be determined by your child’s doctor based on:
- Your child’s age, overall health, and medical history
- The extent of the disease
- Your child’s tolerance for specific medications, procedures, or therapies
- Expectations for the course of the disease
- Your opinion or preference
Your child may require antibiotic therapy as a precaution to prevent future urinary tract infections.
In some cases, medical intervention is not required because the megaureter will resolve on its own over time. If there is a blockage of the urinary tract, however, a megaureter may require surgical intervention. The surgical procedure involves removing the section of the ureter that is abnormal, reducing it, and reconnecting the ureter.
Megaureter surgery
If tests show a block or impaired kidney function, your child may need surgery to fix it. The typical surgery for megaureters involves putting the ureters back into the bladder (“ureteral reimplantation”) and trimming the widened ureter (“ureteral tapering”). If your child doesn’t have a urinary tract infection or decrease in kidney function, the surgery can be delayed until he/she is 12 months old. Surgery in infants isn’t easy and should be done by surgeons skilled at neonatal surgery. Many babies are kept on antibiotics until surgery to help protect them from infections.
During the procedure, the surgeon makes a cut in the lower belly. Depending on the child’s anatomy, the surgeon will get to the ureter either through the bladder (transvesical) or from outside the bladder (extravesical). The ureter is removed from the bladder. If the ureter is very wide, it may need to be trimmed (tapered). Any blocks will be removed. The ureter is then replaced in the bladder. Your child may have a catheter for a few days to help healing. He/she will often stay in the hospital for between 2 and 4 days.
Most megaureters with symptoms are best treated by this open type of surgery. For obstructed megaureters, the block is removed. For refluxing megaureters, the reflux (urine back-up) is corrected. And for very wide ureters, the ureters can be trimmed.
Surgical options
- Cutaneous distal ureterostomy: This may be necessary in a newborn with massive ureteral dilation or poor renal function. The ureter is surgically brought to the surface of the skin to allow it to drain urine freely into the diaper. This allows the affected kidney and ureter to decompress. Around 18 months of age, the ureter is then reimplanted into the bladder.
- Ureterovesical junction obstruction: This surgical procedure involves removing the section of the ureter that is abnormal, reducing it and reconnecting the ureter. The segments of most megaureters regain tone once they are unobstructed.
Other options
In children over 2 years old, balloon dilation of the narrowed part may be possible. The surgeon looks into the bladder with a long, thin telescope with a light at the end (cystoscope). A small wire is passed through the bladder opening and up the ureter. A balloon is used to stretch the narrowed part of the ureter. A silicone tube is left in the ureter for 4 to 6 weeks. Studies show this can clear the block and help most cases of reflux.
Minimally invasive methods, like injecting substances to fix reflux, don’t work well because of the abnormal connection to the bladder.
Laparoscopy is surgery done through thin tubes put into the body through a small cut. The surgeon uses a special camera to see inside the body and miniaturized tools. Laparoscopy for ureteral reimplantation is hard and requires a highly skilled laparoscopic surgeon.
After treatment
For megaureters that require surgery, generally prophylactic antibiotics are continued for some time after surgery, and serial ultrasounds are performed to monitor the kidney. The surgery is very successful at relieving the obstruction.
For megaureters that do not have reflux or obstruction, they generally resolve on their own during childhood. Prophylactic antibiotics are often continued until after potty training and periodic ultrasounds are performed to monitor kidney growth and the megaureter. Once the megaureter resolves, there is no need for further follow up or prophylactic antibiotics.
Even if surgery is needed, the vast majority of children with megaureters go on to live normal lives.
After surgery the size of the ureter may not be corrected immediately, so tests will be repeated several weeks later to show how well the surgery worked. Some of the tests that were done before surgery may need to be repeated several weeks later. The size of the ureter may not improve right away after surgery, so it’ll need to be checked over time.
Some problems that can arise from the surgery are:
- bleeding
- blocked ureter
- vesicoureteral reflux (new or ongoing)
A blockage of urine may occur soon after the operation or after a longer period of time. This problem is seen in only 5 out of 100 of cases, but it may require more surgery. Vesicoureteral reflux problems are seen after surgery in 5 out of 100 of cases as well. This may go away on its own. Most patients are followed for a number of years after surgery. Ultrasound is used to make sure the appearance of the kidney and ureter continues to improve. A renal scan is often done to make sure the kidney is working properly and that the block is fixed. A voiding cystourethrogram (VCUG) is often done a few months after surgery to check for reflux.
Megaureter prognosis
The outcome of ureteral anomalies chiefly depends on the presence or absence of obstruction and/or infection, and associated kidney injury. In the absence of these, no treatment may be necessary, especially in the case of isolated ureteral duplication anomalies, low-grade vesicoureteral reflux (VUR), a small orthotopic ureterocele, or a nonobstructed, nonrefluxing primary megaureter. With respect to primary megaureters, as in the case of vesicoureteral reflux (VUR), spontaneous resolution is common. In the case of the obstructed primary megaureter, spontaneous resolution is less likely to occur; however, one study reported a 70% spontaneous regression 11).
Cases of high-grade vesicoureteral reflux (VUR) are less likely to spontaneously resolve and more likely to put the kidney at risk of scarring due to pyelonephritis. Prevention of infection is essential to minimize the risk of renal damage; therefore, continuous antibiotic prophylaxis is usually used in children with high-grade vesicoureteral reflux (VUR) while awaiting spontaneous resolution. In the case of obstructive ureteroceles, treatment to relieve obstruction optimizes preservation of renal function, as chronic obstruction can lead to renal deterioration.
References [ + ]





{kind=link}