
Contents
Congenital vertical talus
Congenital vertical talus also called rocker-bottom foot is a rare congenital foot deformity in which the sole of a child’s foot flexes abnormally in a convex position giving the foot a rocker-bottom appearance. For this reason, congenital vertical talus is often called rocker-bottom foot. Congenital vertical talus is characterized by a prominent calcaneus/heel and a convexly rounded sole. Congenital vertical talus is usually a rigid deformity, unlike the more common calcaneovalgus foot (flexible deformity), and rarely improves with stretching or bracing. In most cases, surgery is required.
When a child is born, their feet usually appear flat because of the extra fat pads on the bottom. As the child grows, a concave arch in their foot normally develops. In a child with rocker-bottom foot, the bottom of the foot flexes in the opposite direction, making the middle of the foot touch the floor, while the toes and heel curve upward, touching the shin.
Congenital vertical talus is an uncommon disorder. Jacobsen and Crawford 1) reported only 273 cases. Congenital vertical talus (rocker-bottom foot) affects about 1 in 10,000 births and occurs equally in boys and girls. In about half of the cases, both feet are affected. Some have estimated the incidence of congenital vertical talus to be one tenth that of congenital clubfoot.
Congenital vertical talus is often associated with an underlying musculoskeletal or neurological condition such as:
- Spina bifida
- Trisomy 13, 14, 15 or 18
- Arthrogryposis multiplex congenita
In a minority of cases, the cause of rocker-bottom foot is unknown, in an otherwise healthy child.
Although the cause of congenital vertical talus is likely heterogeneous, recent evidence strongly supports a genetic cause linking it to genes expressed during early limb development 2). Traditional management for vertical talus involves extensive surgeries that are associated with significant short- and long-term complications. A minimally invasive approach that relies on serial manipulation and casting to achieve most of the correction has been shown to produce excellent short-term results with regard to clinical and radiographic correction in both isolated and nonisolated cases of vertical talus. Although long-term studies are needed, achieving correction without extensive surgery may lead to more flexible and functional feet, much as Ponseti method has done for clubfeet 3).
Autopsy and surgical findings have contributed to the understanding of the pathologic anatomy of the vertical talus 4). The hindfoot is in marked equinus and valgus caused by contracture of the Achilles tendon and the posterolateral ankle and subtalar joint capsules. The midfoot and forefoot are dorsiflexed and abducted relative to the hindfoot secondary to contractures of the tibialis anterior, extensor digitorum longus, extensor hallucis brevis, peroneus tertius, and extensor hallucis longus tendons and the dorsal aspect of the talonavicular capsule. The navicular is dorsally and laterally dislocated on the head of the talus, resulting in the development of a hypoplastic and wedge-shaped navicular. Both the talar head and neck are abnormal in shape and orientation, resulting in a flat appearance that is angled medially from the midline. The position of the talus stretches vertically and weakens the plantar soft tissues, including the calcaneonavicular, or spring ligament, which gives the foot a rocker-bottom appearance. The plantar surface of the foot is convex, whereas the dorsal aspect of the midfoot has deep creases (see Figure 1). The calcaneus is in extreme equinus, which often causes either dorsolateral subluxation or frank dorsal dislocation of the calcaneocuboid joint. The posterior tibial tendon and the peroneus longus and brevis are commonly subluxated anteriorly over the medial and lateral malleolus, respectively; the subluxated tendons may then function as ankle dorsiflexors rather than plantar flexors 5).
Primary surgical treatment of a congenital vertical talus in a child younger than 2 years can be done with either a one-stage or two-stage extensive soft-tissue release 6). The first stage of the two-stage approach consists of lengthening the contracted dorsolateral tendons, releasing the associated dorsolateral capsular contractures, and reducing the talonavicular and subtalar joint complex. The second stage consists of lengthening the Achilles and peroneal tendons as well as performing a posterolateral capsular release 7). Historically, the one-stage approach was simply a combination of the two stages into a one-stage procedure. Seimon 8) modified the one-stage approach, emphasizing that, by carefully addressing the dorsolateral soft-tissue contractures, less extensive soft-tissue release was needed posteriorly. Mazzocca et al 9) compared Seimon’s dorsal approach with more extensive staged approaches and found that it required less surgical time, had fewer complications, and resulted in improved clinical outcomes. Today, most authors use some form of the single-stage approach 10) and report better results than those achieved using a two-stage approach 11). However, the complications associated with both approaches (eg, wound necrosis, osteonecrosis, undercorrection and overcorrection of deformities) are concerning 12). Longer-term problems include stiffness of the ankle and subtalar joints and the development of degenerative arthritis, leading to the need for salvage procedures, such as subtalar and triple arthrodeses. These problems are similar to the poor long-term outcomes and functional disability reported with extensive soft-tissue release surgery for clubfoot 13).
Figure 1. Vertical talus deformity
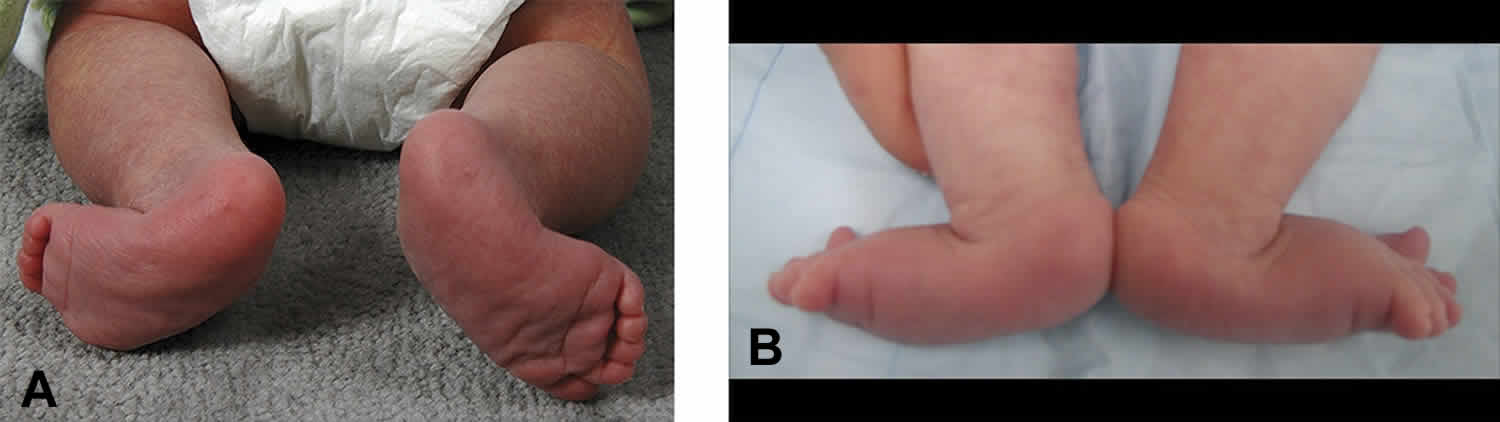
Footnote: Clinical photographs of a newborn’s feet demonstrating the features of vertical talus. The plantar aspect of the feet (A) show forefoot abduction deformities, and the dorsolateral aspect of the feet (B) demonstrate deep creases on presentation secondary to forefoot and midfoot dorsiflexion.
[Source 14) ]Congenital vertical talus classification
Current classification systems for vertical talus focus on either a description of the anatomic abnormalities present or the presence or absence of associated diagnoses. The most widely used anatomic classification system was proposed by Coleman et al 15). They described two types of vertical talus; type 1 deformity is characterized by a rigid dorsal dislocation of the talonavicular joint. In addition to a rigid dislocation of the talonavicular joint, a type 2 deformity has a dislocation or subluxation of the calcaneocuboid joint (ie, the long axis of the calcaneus lies plantar to the long axis of the cuboid). Other classification systems have focused on whether the vertical talus was an isolated deformity or was present in addition to other abnormalities 16). The problem with these classification systems is that they do not directly take into account the motor function of the lower legs. Weak or absent motor function in the lower leg musculature is predictive of not only poor response to initial treatment but also a risk of relapse 17). The child’s ability to dorsiflex and plantarflex the toes can be evaluated by lightly stimulating the dorsal and plantar aspects of the foot. Movement can be graded as definitive, slight, or absent. This simple examination can be repeated at each clinical visit to improve accuracy. A new classification system that takes this into account is needed because the ability to better predict the response to treatment will allow for the development of an individualized treatment program for patients.
It should be noted that current classification systems have attempted to define oblique talus as a milder form of vertical talus based on radiographic and clinical examination criteria 18). However, these attempts at classification have not translated into consistent treatment recommendations because some oblique tali do require treatment despite being milder in nature 19). Oblique tali that have an associated Achilles tendon contracture are at risk of becoming symptomatic with time. For this reason, some experts consider oblique tali and vertical tali to be related entities that occur along a spectrum of severity. Similar to clubfeet, not all vertical tali have the same rigidity. If oblique talus is diagnosed on radiography, but an equinus contracture (defined as the inability to achieve 10° of passive ankle dorsiflexion with the knee extended and flexed) is present, some experts treat it as a vertical talus. Treatment decisions, should be based on the rigidity of the talonavicular joint as well as of the hindfoot.
Vertical talus causes
In most cases, the cause of vertical talus deformity remains unknown. Approximately one half of cases of vertical talus occur in conjunction with neurologic disorders (neuromuscular and central nervous system) 20) or known genetic defects and/or syndromes 21). The other half occur in children without other congenital anomalies and are considered idiopathic or isolated cases 22). Ogata et al 23) proposed a congenital vertical talus classification system that divides patients into the following three groups:
- Idiopathic
- Genetic/syndromic
- Neuromuscular
The most common neurologic disorders associated with vertical talus are distal arthrogryposis and myelomeningocele 24) and the most common genetic defects include aneuploidy of chromosomes 13, 15, and 18 25). Vertical talus is also commonly associated with a variety of syndromes, including De Barsy, Costello, and Rasmussen syndromes22 and split hand and split foot limb malformation disorders. Of the 50% of cases of vertical talus that are isolated, almost 20% have a positive family history of vertical talus. In most of these cases, congenital vertical talus is inherited in an autosomal dominant fashion, supporting the theory that a significant number of isolated cases have a genetic origin, as well 26). Specific gene mutations in the homeobox transcription factor and cartilage-derived morphogenetic protein-1 genes have been found to be causative in some patients with familial, autosomal dominant isolated vertical talus and in some families with congenital hand and foot anomalies of which vertical talus is a feature 27). Growth differentiation factor 5 is closely related to the bone morphogenetic proteins associated with neurologic and limb development.
No single gene defect is responsible for all cases of vertical talus; therefore, it is likely that the pathophysiologic basis for the development of vertical talus is heterogeneous in nature. One hypothesis to explain vertical talus associated with neuromuscular disorders is an imbalance in muscle strength. In patients with myelomeningocele with vertical talus, a weak posterior tibialis and relatively strong ankle dorsiflexors could be contributing factors, whereas weakness of the foot intrinsic muscles may play a contributing role in other neuromuscular disorders. These mechanisms and congenital muscle abnormalities, which are also seen in the setting of distal arthrogryposis, may play a role in some cases of isolated vertical talus, as well. This is supported by the high percentage of abnormal skeletal muscle biopsies performed in this patient population 28). Congenital vascular deficiency of the lower extremities has also been proposed as a potential cause of vertical talus based on magnetic resonance angiography findings that demonstrated congenital arterial deficiencies of the lower extremity in a group of patients with isolated vertical talus 29).
Vertical talus associations
- Aneuploidic syndromic
- trisomy 13
- trisomy 18
- 18q deletion syndrome
- Non-aneuploidic non-syndromic
- spina bifida
- arthrogryposis
Congenital vertical talus symptoms
The most common symptom of congenital vertical talus is a rocker-bottom appearance of the foot, which is usually obvious at birth or seen when a child begins to walk.
Other symptoms include:
- An upward flex of the mid- and forefoot
- The hindfoot is elevated due to an abnormal flex in the ankle
- The midfoot cannot be properly aligned with the hindfoot
- Abnormal positioning of the foot; child may walk on the inside of their foot, while the outside edge is elevated, leading to improper balance and weight distribution
Clinically, congenital vertical talus presents as a rigid flatfoot with a rocker-bottom appearance of the foot. The calcaneus is in fixed equinus, and the Achilles tendon is very tight. The hindfoot is in valgus, and the head of the talus is found medially in the sole, creating the rocker-bottom appearance. The forefoot is abducted and dorsiflexed.
The foot is stiff. In ambulatory children, calluses can develop under the head of the talus, which is very prominent along the plantar-medial foot.
Associated genetic syndromes must be excluded; therefore, a consultation with a pediatric geneticist may be indicated.
Congenital vertical talus diagnosis
Early detection of congenital vertical talus is important for successful treatment. Trained pediatric orthopaedic surgeon will perform a complete medical history, a physical examination and a visual evaluation of your child.
During the physical exam, the doctor will examine your entire child — not just their foot. The doctor will be looking for other abnormalities such as multiple joint contractures or evidence suggesting your child may have a larger multisystem genetic disorder.
Doctors will also closely examine your child’s foot — while standing and in motion — to determine if your child has rocker-bottom foot, or a more common and benign conditions such as calcaneovalgus foot or flat foot. Though symptoms of these conditions may mimic each other in young children, treatments are very different.
Physical examination
Hindfoot equinus, hindfoot valgus, forefoot abduction, and forefoot dorsiflexion are present in all newborns with vertical talus. The rigidity of the deformity is the key to distinguishing between vertical talus and more common conditions, such as calcaneovalgus foot, posteromedial bowing of the tibia, and oblique talus. If hindfoot equinus is not a clinical feature, then the deformity is not vertical talus and is likely positional in nature. Because of the frequency of neuromuscular and genetic abnormalities associated with vertical talus, it is important to perform a comprehensive physical examination. The clinician should look for facial dysmorphic features that require a referral to a geneticist or abnormalities suggestive of a neuromuscular etiology, which would require MRI evaluation of the neuroaxis and referral to a pediatric neuromuscular specialist. The presence of a sacral dimple, in particular, should alert the examiner to possible central nervous system anomalies.
It is equally important for the examiner to document motor function of the foot and ankle with special attention to the toe flexors and extensors. This is done by stimulating the plantar and dorsal aspects of the foot separately to elicit plantar flexion and dorsiflexion of the toes. This should be done serially during treatment sessions because the examination can be difficult, and results from serial examinations are more telling. The presence of dorsiflexion and plantar flexion of the toes is recorded as absent, slight, or definitive. This should be recorded for the great toe alone as well as the lesser toes as a separate group. In our experience, slight or absent ability to move the toes with stimulation correlates with a vertical talus deformity that is more rigid and less responsive to treatment. It may also be indicative of a subtle congenital neurologic or muscular anomaly.
Clinically, a congenital vertical talus foot has a convex plantar surface that results in a rocker-bottom appearance (Figure 1A). The dorsum of the foot has deep creases secondary to forefoot and midfoot dorsiflexion (Figure 1B). The extreme dorsiflexion of the forefoot creates a distinct palpable gap dorsally where the navicular and talar head would articulate in a normal foot. Characteristics of this gap can help the examiner assess rigidity. If the gap reduces with plantar flexion of the forefoot, then the deformity has a degree of flexibility; this may help predict responsiveness to treatment. Left untreated, a rigid vertical talus deformity may worsen with weight bearing because secondary adaptive changes occur in the tarsal bones 30). Painful callosities can develop along the plantar medial border of the foot around the prominent and unreduced talar head. Heel strike does not occur, shoe wear becomes difficult, and pain develops 31).
Imaging studies
To confirm the diagnosis or better understand the anatomy of your child’s foot and leg, doctors may also order imaging tests such as:
- X-rays, which produce images of bones. Weightbearing anteroposterior (AP) and lateral views of the foot are the first radiographs that must be obtained. A lateral radiograph with the foot in maximum plantarflexion is mandatory to confirm congenital vertical talus. The hallmark of congenital vertical talus deformity is an abnormally positioned talus bone (this is the bone that connects the foot to the ankle). Because the navicular may not be ossified, the alignment of the first metatarsal to the talus must be evaluated. In a vertical talus, the metatarsal does not line up with the talus. Lines drawn through the long axis of the first metatarsal and the talus converge on the plantar aspect of the foot. Hamanishi 32) described two radiographic angles: the talar axis–first metatarsal base angle (TAMBA) and the calcaneal axis–first metatarsal base angle (CAMBA). The changing point from a flexible oblique talus to rigid CVT is a TAMBA of approximately 60° and a CAMBA of 20°.
- EOS imaging, an imaging technology that creates 3-dimensional models from two flat images. Unlike a CT scan, EOS images are taken while the child is in an upright or standing position, enabling improved diagnosis due to weight-bearing positioning.
- Computed tomography (CT) scan, which uses a combination of X-rays and computer technology to examine bones and produces cross-sectional images (“slices”) of the body.
- Magnetic resonance imaging (MRI), which uses a combination of large magnets, radiofrequencies and a computer to produce detailed images of organs, soft tissues, muscles, ligaments and other structures within the body. Your child is exposed to no radiation during an MRI. Magnetic resonance imaging (MRI) of the spine may be indicated if an occult spinal dysraphism, such as lipomeningocele, is suspected 33). Posterior and lateral lumbar spine radiographs also may be useful to exclude occult spinal dysraphism. Thometz et al 34) evaluated nine patients with congenital vertical talus using MRI to evaluate the three-dimensional morphologic changes and pathoanatomy. They concluded that there is significant pathology at the level of the subtalar joint.
- Ultrasonography. Ultrasonography has been reported to be helpful in distinguishing between congenital vertical talus (irreducible talonavicular dorsal dislocation) and oblique talus (reducible talonavicular dorsal dislocation) 35). Lateral radiographs of the foot in maximal plantarflexion can reveal if the navicular is reducible. However, radiographs of an infant’s foot can be difficult to interpret. The use of dynamic ultrasonography has been reported to be helpful in the evaluation of infants with vertical or oblique talus 36).
If your child appears to have a neurological condition, the orthopedic physician may refer your child to a neurologist for a complete neurological exam.
Congenital vertical talus treatment
All children with congenital vertical talus will require some form of treatment. While some children may be helped with non-surgical treatment, most will require surgery.
Non-surgical treatment
Doctors may recommend a variety of non-surgical treatments to prevent your child’s condition from getting worse. These include:
- Stretching exercises for the forefoot and hindfoot
- Serial manipulation and casting of the midfoot and forefoot in a flexed position to reduce the upward curve of the foot
Improvements from these treatments do occur, but are often temporary.
Congenital vertical talus surgery
Surgery for congenital vertical talus is complicated because it involves correcting foot movement in three directions — side-to-side, up-and-down and front-and-back. A specialist in pediatric foot deformities should perform it. Surgery can dramatically improve the long-term outcomes for your child with congenital vertical talus, but it can also be a stressful experience for you and your child. With adequate serial casting, need for extensive soft-tissue release surgery can be minimized to minimally invasive tendon procedures which leave smaller scars and shorter recovery time. Other procedures can include bone work in older children.
Controversy exists over the choice of surgical approaches. However, some experts believe that the choice of structures to be released is a more important factor in determining outcomes than is the choice of incisions to be used. Special attention must be paid to the dorsal and dorsolateral contracted tissues. Controversy also exists over the need for an anterior tibialis tendon transfer.
Several authors, beginning with Osmond-Clarke 37), Herndon and Heyman 38) and Coleman and associates 39), described staged two-incision reconstructive surgery. The first stage of the Coleman procedure consisted of lengthening the extensor digitorum longus, the extensor hallucis longus, and the tibialis anterior, with capsulotomies of the talonavicular and calcaneocuboid joints and release of the talocalcaneal interosseous ligament. The second stage consisted of Achilles tendon lengthening and a posterior capsulotomy of the ankle and subtalar joints.
After noting a high incidence of complications with the two-stage technique, Ogata et al 40) recommended a single-stage procedure with a medial approach. Kodros and Dias 41) published results they derived using a single-stage approach with a Cincinnati incision.
Seimon described a single-stage dorsal approach in which the extensor digitorum longus and the peroneus tertius were tenotomized and the talonavicular joint was opened 42). The talonavicular joint was reduced and held with a K-wire. The Achilles tendon was lengthened percutaneously. Stricker and Rosen 43) published their experience with this technique, as did Mazzocca et al 44); both groups noted excellent results with few complications.
The trend toward less surgery for congenital vertical talus continued with Dobbs et al 45), who published their technique of casting, percutaneous K-wire pinning of the talonavicular joint, and percutaneous heel-cord tenotomy. No patients had extensive soft-tissue releases, though some required lengthening of the tibialis anterior or the peroneus brevis tendon. Casting without pinning of the talonavicular joint was associated with recurrence of deformity.
Saini et al 46) reported on their surgical experience with 20 cases of congenital vertical talus using a dorsal approach. According to the authors, talonavicular reduction was achieved in all 20 feet, and postoperative talocalcaneal and talo-first metatarsal angles were significantly improved. The results were retained at 4-year follow-up 47).
Bhaskar 48) described a surgical technique used for idiopathic congenital vertical talus in four feet; this technique was similar to the Ponseti technique for clubfoot, except that the forces applied were in a reverse direction. The four feet were treated by serial manipulation and casting, tendo Achillis tenotomy, and percutaneous pinning of the talonavicular joint.
To correct the forefoot deformity, four to six plaster cast applications were required 49). Once the talus and navicular were aligned, percutaneous fixation of the talonavicular joint with a K-wire and percutaneous tendo Achillis tenotomy under anesthesia were performed, followed by application of a cast with the foot in slight dorsiflexion. After treatment, the mean talocalcaneal angle decreased from 70º to 31º, and the mean talar axis–first metatarsal base angle (TAMBA) decreased from 60º to 10.5º.
Wright et al 50) reported on 12 children (21 feet) with idiopathic and teratologic causes. They noted 10 recurrences, a rate higher than those cited in other reports. The authors felt that a limited capsulotomy of the talonavicular joint might reduce the risk of recurrence. They did not find a difference in results between the two groups of patients.
In 2012, Chalayon et al 51) reported on 15 consecutive patients (25 feet) with nonisolated congenital vertical talus who were followed for a minimum of 2 years after reverse Ponseti casting, percutaneous Achilles tendon lengthening and pin fixation of the talonavicular joint. Five feet required a small medial incision to ensure joint reduction and accurate pin placement, and 20 feet had selective capsulotomies of the talonavicular joint and the anterior aspect of the subtalar joint. Initial correction was obtained in all cases, but recurrence was noted in three patients (five feet).
Yang and Dobbs 52) published a comparison of the minimally invasive method versus extensive soft-tissue release with a minimum follow-up of 5 years (Dobbs technique). They documented that the minimally invasive method resulted in better results in terms of range of motion and patient-reported outcomes.
Chan et al 53) evaluated the Dobbs method for correction of idiopathic congenital vertical talus versus correction of teratologic congenital vertical talus. The results were comparable, but the recurrence rate was slightly higher for teratologic congenital vertical talus.
Complications
Complications can occur around the time of surgery (perioperatively) or can manifest early or late in the postoperative period.
Common complications in the perioperative period include infection, wound-healing problems, and skin slough; however, these complications are not unique to congenital vertical talus.
In the first 1-2 years after surgery, the deformity can recur, usually secondary to undercorrection. Undercorrection can occur because of incomplete talonavicular reduction, insufficient posterior ankle release, or residual forefoot abduction. [16] Recurrence of the deformity can also be attributable to neurologic causes, especially in patients with spina bifida. Kodros and Dias reported a high recurrence rate in patients with spina bifida and believed that in these cases the recurrences might be secondary to a tethered spinal cord or other neurologic abnormality.
avascular necrosis (AVN) of the talus is a unique complication of congenital vertical talus surgery. It was more often reported in the older literature and was associated with the two-stage release and extensive surgery. Subsequent articles by Kodros and Dias 54), Seimon 55), Stricker and Rosen 56), and Mazzocca et al 57) did not report occurrences of avascular necrosis (AVN) of the talus.
Late complications include restricted range of motion of the foot and ankle, which can contribute to calf muscle atrophy. This in turn can lead to easy fatigue of the affected limb.
Congenital vertical talus prognosis
Most children who are surgically treated for congenital vertical talus have good outcomes. Some children may need an orthotic to ensure proper foot alignment during critical growth and development periods.
Children who have congenital vertical talus as part of a larger neurological or musculoskeletal syndrome will likely need lifelong follow-up care.
In general, the outcome and prognosis are good 58). Some minor calf atrophy and foot size asymmetry occur and are more noticeable in unilateral cases. Ankle range of motion is about 75% of normal. If avascular necrosis (AVN) of the talus occurs, the results are less optimal because of ankle pain, stiffness, and weakness.
Patients with congenital vertical talus have a more favorable prognosis when treated with the Dobbs technique than they do when treated with extensive soft-tissue release. Idiopathic congenital vertical talus tends to have a more favorable outcome than teratologic congenital vertical talus does 59).
References [ + ]





{kind=link}