Contents
Congenital scoliosis
Congenital scoliosis is a sideways curvature of the spine that is caused by a defect that was present at birth. The term “congenital” means that you are born with the condition. Congenital scoliosis occurs in only 1 in 10,000 newborns and is much less common than the type of scoliosis that begins in adolescence.
Congenital scoliosis starts as the spine forms before birth. Part of one vertebra (or more) does not form completely or the vertebrae do not separate properly. Some types of congenital scoliosis can change quickly with growth while others remain unchanged.
Children with congenital scoliosis sometimes have other health issues, such as kidney, heart or bladder problems.
Even though congenital scoliosis is present at birth, it is sometimes impossible to see any spine problems until a child reaches adolescence.
No certain cause of congenital scoliosis has been identified until today 1). Congenital scoliosis is a failure of vertebral formation, segmentation, or a combination of the 2 arising from abnormal vertebral development during weeks 4 to 6 of gestation. The associated spinal deformity can be of varying severity and result in a stable or progressive deformity based on the type and location of the anomalous vertebrae 2). The ultimate cause is probably multifactorial, involving some combination of inherited genetic susceptibility and de-novo alteration in molecular mechanisms, possibly from exposure to teratogens such as cigarette smoking, organophosphate pesticides, or carbon monoxide 3).
The diagnosis requires a thorough clinical and imaging examination in order to establish an individualized therapeutic strategy.
The treatment of congenital scoliosis is different from the adolescent idiopathic one. Therapeutic criteria are significantly different. It is essential to assess the difference in growth of the concavity related to the convexity when choosing a particular procedure. The magnitude of the curve and the progressive rate are fundamental issues to the surgeon.
Defects of segmentation usually induce a severe deformity. If the segmentation defect is associated to 2-3 fully segmented hemivertebrae, a maximal progression rate is present and significant curves are present at early ages (Figure 1). A severe curve in older children is very difficult to correct and a result is never obtained as in idiopathic scoliosis where correction may be up to 50-60%. In congenital scoliosis corrections of such kind of curves require laborious interventions, osteotomy or segmental resection, with high neurological risks 4) and low rates of success, not exceeding 20% as presented in different statistical data.
As a strategic aspect, the surgeon has to know that the preoperative planning has to identify the presence or absence of a dysraphic status 5) or syringomyelia. Always, the first aim is to stop the progression of the deformity.
Figure 1. Congenital scoliosis
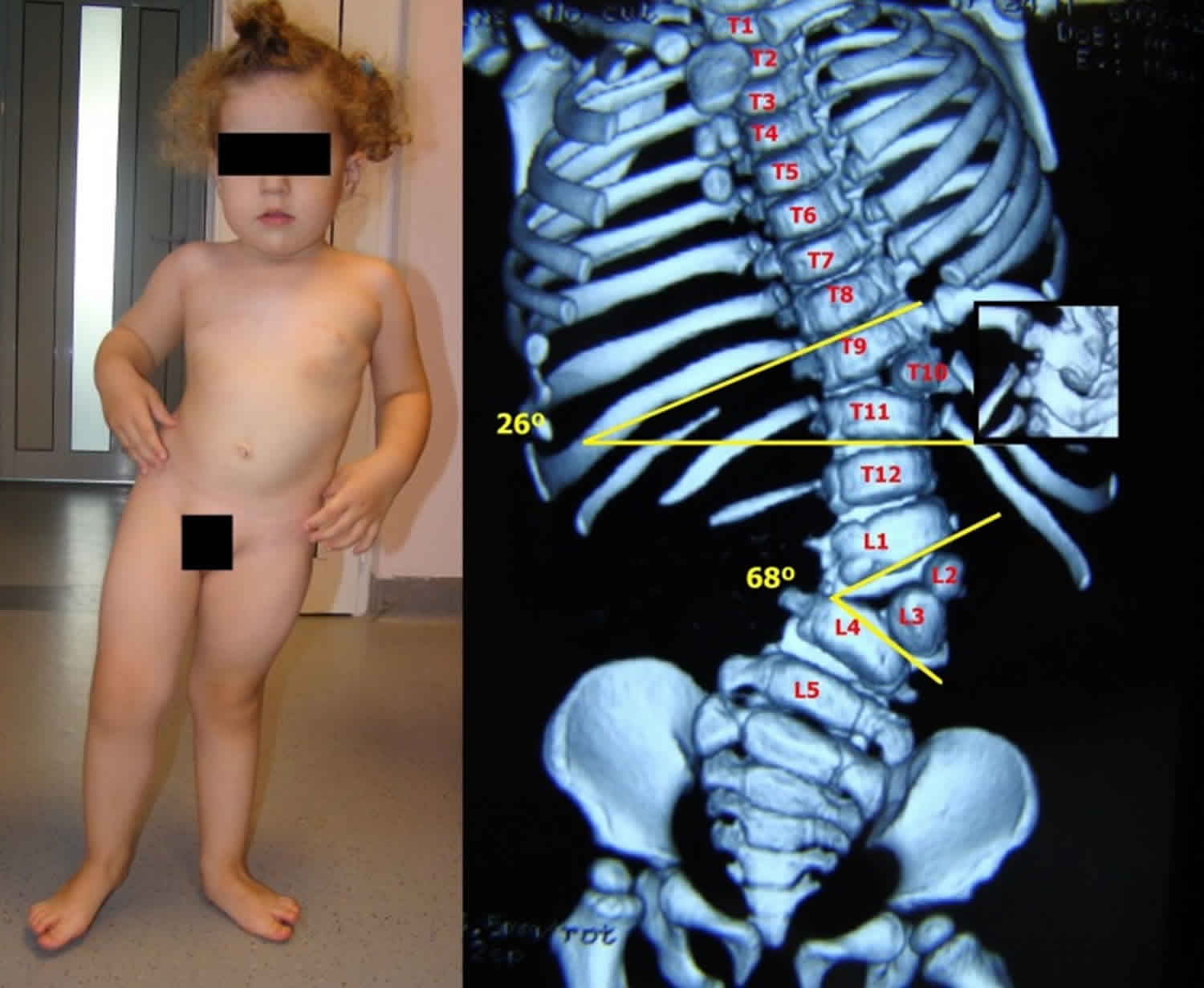
Footnote: Congenital scoliosis with a high progression potential due to 3 hemivertebrae situated on the same side of the spine. Trunk shifting and shoulder imbalance are noticed at an early age
[Source 6) ]Congenital scoliosis types
Congenital scoliosis represents a wide range of pathology from the simple, stable hemivertebra to the complex, progressive spinal deformity with chest wall abnormalities and associated cardiac, renal, and neural axis anomalies 7).
The first classification of congenital scoliosis based on X-rays imaging was described by Winter in 1968 8). Kawakami 9) reclassified the vertebral malformations depending on the presence or absence of normal formation based on a 3D-CT study. The purpose of these classifications is to understand the embryology, etiology, prognostic and to choose the right therapeutic strategy.
Congenital scoliosis is a malformation characterized by a longitudinal and rotational imbalance.
- Congenital scoliosis with imbalance in the longitudinal growth is produced by defects of formation, segmentation or mixed ones.
- Congenital scoliosis with rotational imbalance is mainly characterized by the vertebral rotation related to the curve in the coronal plan and they may be due to an effect of:
- spinal traction – osseous bridges with congenital transverso-sacrate synostosis;
- spinal pushing – mega-apophysis of the L5 transverse process;
- mixed (traction and pushing) – sacral agenesis with pelvic malposition.
- These types of scoliosis are secondary to a congenital malformation, either vertebral or pelvic, which induce as the main manifestation the vertebral rotation by means of traction, pushing or mixed action. Usually, the scoliosis and the vertebral rotation are not present at birth. During growth and development, the first presence is the vertebral rotation accompanied by walking impairment and next by the scoliotic curve.
Congenital scoliosis with longitudinal imbalance, mainly with deviation in the coronal plan in comparison with vertebral rotation, may be due to defects of formation with the presence of: trapezoidal vertebra, hemivertebra or vertebral hemibody. Hemivertebra depending on segmentation may be fully segmented, hemisegmented (partially segmented) or unsegmented. There may be congenital malformations characterized by the presence of more than one hemivertebra disposed in the following manner: adjacent (successive) – 2-3 hemivertebrae disposed unilaterally inducing a short arch scoliosis, being noticed at birth and having a high rate of evolution, unilateral alternant (intermittent) – 2-3 hemivertebrae placed unilaterally leading to a long arch scoliosis and a unique curve and bilateral alternant which themselves may be:
- compensated – 2 symmetric hemivertebrae in a 4-5 vertebral segment inducing an equilibrated spinal deformity not requiring surgery;
- uncompensated – if the hemivertebrae are disposed on a distance of more than 6 vertebrae leading to a double congenital scoliosis.
Due to defects of segmentation, congenital scolioses are characterized by a unilateral defect: longitudinal bar or a bilateral defect: vertebral block.
The third possibility is represented by mixed anomalies where we may find the next malformations:
- hemivertebra and a bar on the opposite spinal side;
- hemivertebra, vertebral block and longitudinal bar.
Incomplete formation of vertebrae
As the spine forms before birth, part of one vertebra (or more) may not form completely. When this occurs, the abnormality is called a hemivertebra and can produce a sharp angle in the spine. The angle can get worse as the child grows.
This abnormality can happen in just one vertebra or in many throughout the spine. When there is more than one hemivertebra, they will sometimes balance each other out and make the spine more stable.
Failure of separation of vertebrae
During fetal development, the spine forms first as a single column of tissue that later separates into segments that become the bony vertebrae. If this separation is not complete, the result may be a partial fusion (boney bar) joining two or more vertebrae together.
Such a bar prevents the spine from growing on one side after a child is born. This results in a spinal curve that increases as a child grows.
Combination of bars and hemivertebrae
The combination of a bar on one side of the spine and a hemivertebra on the other causes the most severe growth problem. These cases can require surgery at an early age to stop the increased curvature of the spine.
Compensatory curves
In addition to scoliosis curves, a child’s spine may also develop compensatory curves in order to maintain an upright posture. This occurs when the spine tries to make up for a scoliosis curve by creating other curves in the opposite direction above, or below, the affected area. The vertebrae are shaped normally in compensatory curves.
Congenital scoliosis causes
Congenital scoliosis is a failure of vertebral formation, segmentation, or a combination of the 2 arising from abnormal vertebral development during weeks 4 to 6 of gestation. The associated spinal deformity can be of varying severity and result in a stable or progressive deformity based on the type and location of the anomalous vertebrae 10).
The ultimate cause of a congenital spinal abnormality is an irrecoverable difference in spine development at the embryonic level. Much research has been performed to understand the mechanisms of embryonic segmentation, and a variety of genetic defects have been suggested as a cause for congenital vertebral malformations.
Single-nucleotide polymorphisms in glucose-metabolizing genes, including GLUT1, HK1, and LEP, have been linked to the occurrence of malformations observed in diabetic embryopathy 11). Hox-mediated gene expression has been thought to be the target for spine abnormalities related to carbon monoxide 12). In addition, an increased risk of congenital vertebral malformations is noted in monozygotic and dizygotic twins 13).
Despite the isolation of genetic mechanisms, no convincing familial linkage exists to explain the majority of congenital scoliosis cases. Winter et al 14) found that only 13 of 1250 patients had a positive family history of such deformity. Furthermore, hereditary congenital scoliosis is relegated to sporadic case reports and is described mostly in the setting of an overlying syndrome, such as Jarcho-Levin (extensive defects of segmentation in association with spondylocostal, costovertebral, or spondylothoracic dysplasia).
The ultimate cause is probably multifactorial, involving some combination of inherited genetic susceptibility and de-novo alteration in molecular mechanisms, possibly from exposure to teratogens such as cigarette smoking, organophosphate pesticides, or carbon monoxide 15).
Congenital scoliosis symptoms
Congenital scoliosis is often detected during the pediatrician’s examination at birth because of a slight abnormality of the back.
Scoliosis is not painful, so if the curvature is not detected at birth, it can go undetected until there are obvious signs — which could be as late as adolescence. A child may suspect that something is wrong when clothes do not fit properly. Parents can discover the problem in early summer when they see their child in a bathing suit.
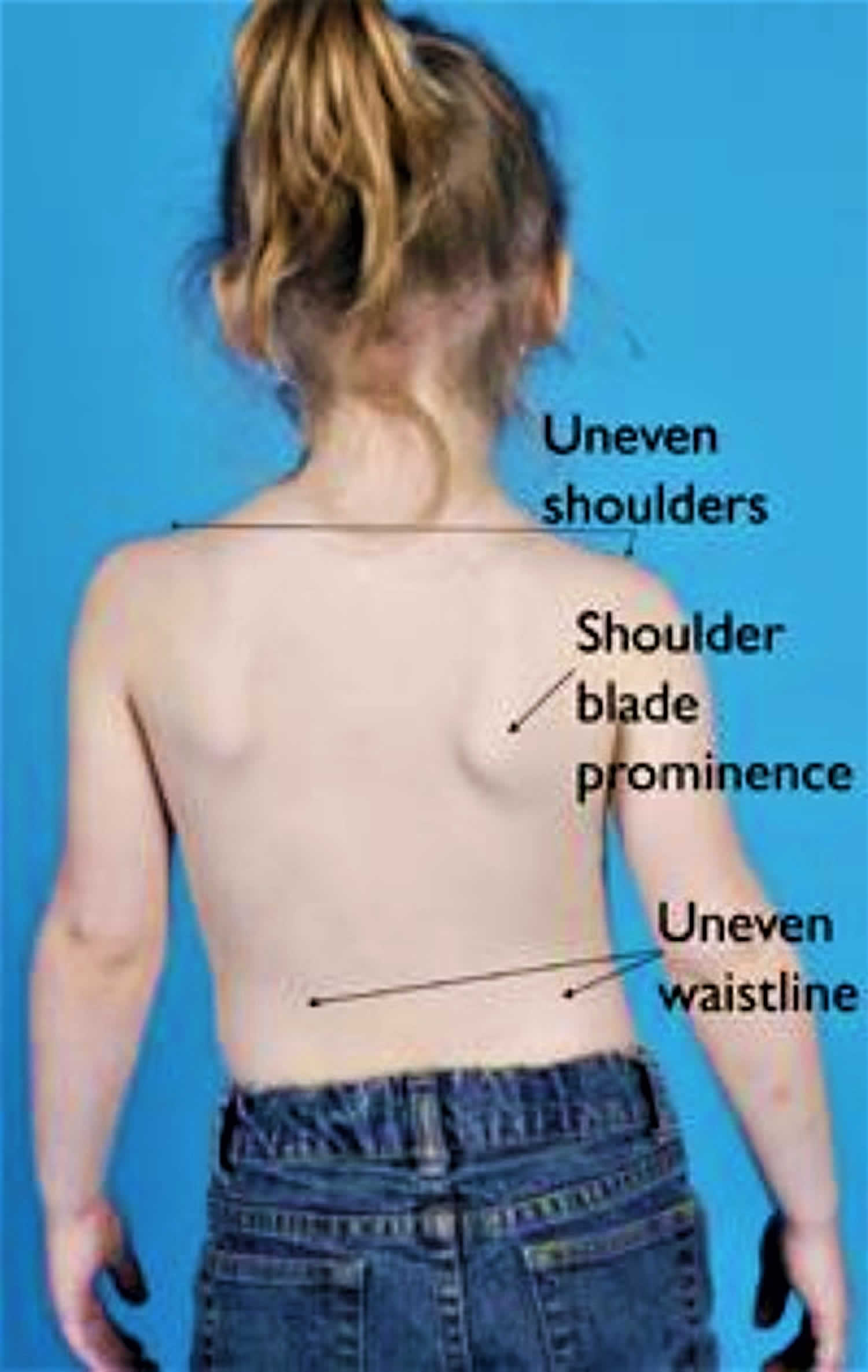
The physical signs of scoliosis include:
- Tilted, uneven shoulders, with one shoulder blade protruding more than the other
- Prominence of the ribs on one side
- Uneven waistline
- One hip higher than the other
- Overall appearance of leaning to the side
- In rare cases there may be a problem with the spinal cord or nerves that produces weakness, numbness, or a loss of coordination.
Associated anomalies
Letts et al 16) found that 82% of patients with congenital scoliosis had associated malformation in four different organ systems. Beals et al found that 61% of patients with congenital scoliosis had abnormalities in seven different organ systems. Highest on the list were anomalies of the genitourinary tract.
Research on patients with congenital scoliosis by MacEwen et al 17) revealed a 20% incidence of urinary tract anomalies detected on routine intravenous pyelography (IVP), whereas a study by Hensinger et al 18) on cervical spine anomalies found a rate of 33%. Many of these anomalies, such as the presence of a single kidney, duplicate ureters, or crossed renal ectopia, while being of interest, were not potentially dangerous. However, in about 5% of the patients, obstructive uropathy, most commonly urethrovesicular obstruction, was present.
Renal ultrasonography (US) and magnetic resonance imaging (MRI) may be used to diagnose renal anomalies accurately 19).
A second area of great concern is cardiac anomalies. As many as 10-15% of patients with congenital scoliosis have been noted to have congenital heart defects. Murmurs should never be attributed to the scoliosis and must be evaluated thoroughly.
The frequency of spinal dysraphism is high in patients with congenital scoliosis. The prevalence of a dysraphic lesion was approximately 40% in three independent studies. McMaster 20) reported that about 20% of these patients with congenital scoliosis had some form of dysraphism (eg, diastematomyelia, tethered spinal cord, fibrous dural band, syringomyelia, or intradural lipoma). Many other anomalies can occur in addition to the above problems, such as Sprengel deformity, Klippel-Feil deformity, Goldenhar syndrome (oculoauriculovertebral dysplasia), and anal atresia.
Neurologic malformations
Congenital scolioses are associated in 35% of the patients with other neurologic malformations related to the nervous system and its coating. The most frequently encountered are diastematomyelia, Chiari’s malformation, intradural lipoma and tethered cord 21).
Congenital heart malformations
Congenital heart malformations are present in up to 25% of the patients with congenital scoliosis. Severe anomalies like Fallot tetralogy or the transposition of the great vessels require surgery prior to a spinal surgical approach 22).
Urologic anomalies
Urologic anomalies are encountered in 20% of the cases. These anomalies associated to congenital scoliosis are horseshoe kidney, vesicoureteral reflux (VUR) or hypospadias. Some kids may also have inguinal hernia, which is usually of great size, needing surgery 23).
Musculoskeletal anomalies
These malformations, clinically and imagistically detected, are usually treated after scoliosis surgery. They include Sprengel’s disease, Klippel-Feil syndrome 24), congenital femoral hypoplasia or acetabular dysplasia.
Congenital scoliosis diagnosis
The doctor will initially take a detailed medical history and may ask questions about recent growth.
Taking a full, detailed history and performing a full physical examination are mandatory because associated anomalies of many organs are common. [18] Maternal perinatal history, family history, and developmental milestones must be explored fully. A comprehensive review of systems includes evaluation for the following:
- Hearing, visual, and dental problems
- Cleft palate and cleft lip
- Hernias, anorectal abnormalities, and genitourinary problems
- Cardiac murmurs
- Respiratory complaints
- Neurologic disorders
In the physical examination, the physician must not only explore the spinal deformity but also focus particular attention on chest deformities and cutaneous lesions (especially dimples and hair patches overlying the spine). A detailed neurologic examination should be performed.
The genitalia should be examined for maturity, epispadias, hypospadias, and the presence of undescended testicles. The hand must be examined for clubhand, thenar hypoplasia, or other, more subtle, anomalies. The feet must be studied for clubfeet, cavus or varus deformities, vertical tali, clawing of the toes, or other signs of motor weakness.
During the physical exam, your doctor may have your child stand and then bend forward from the waist, with arms hanging loosely, to see if one side of the rib cage is more prominent than the other.
Your doctor may also perform a neurological exam to check for:
- Muscle weakness
- Numbness
- Abnormal reflexes
Physical examination
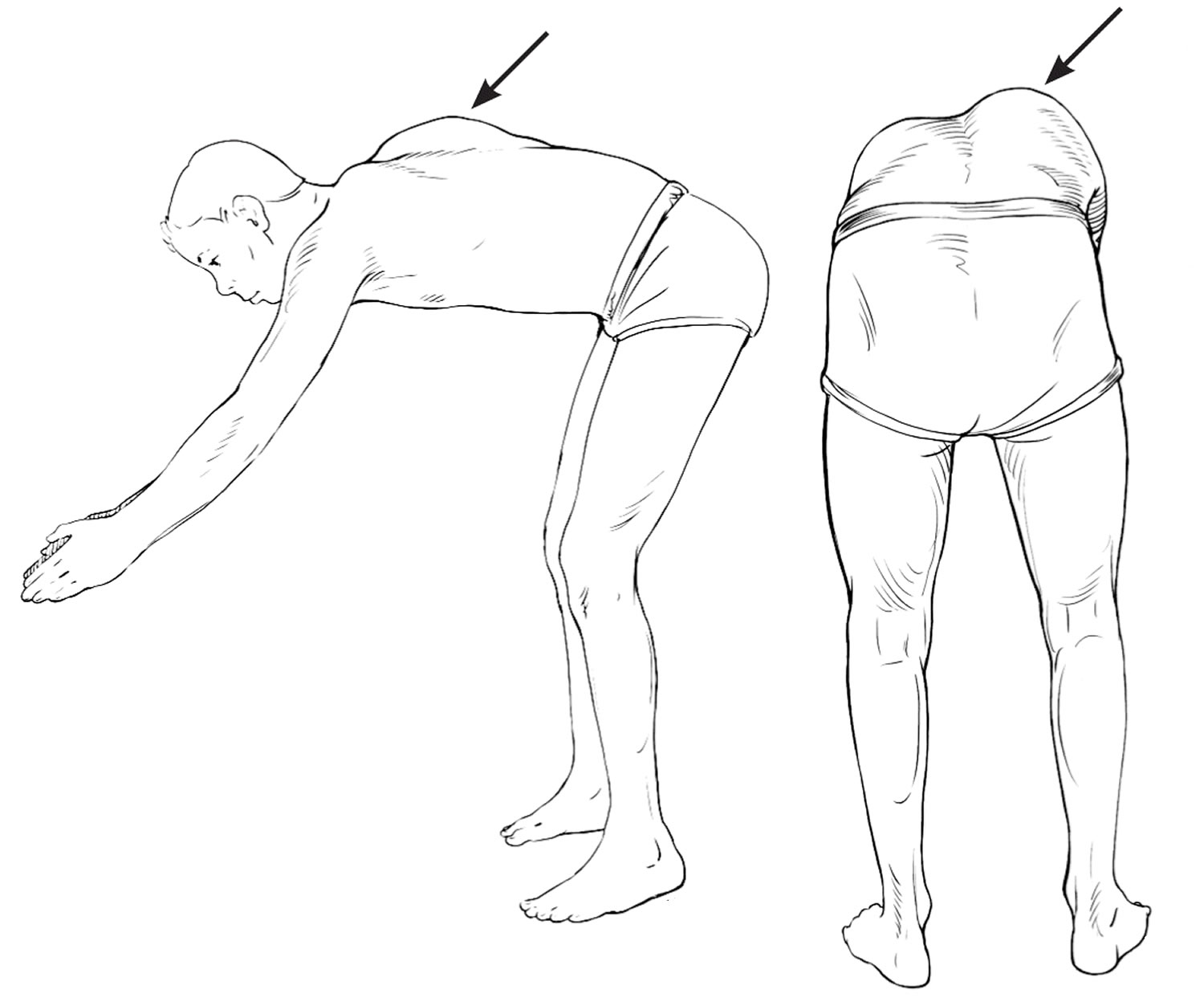
Physical examination for scoliosis mainly consists of the Adam’s forward bend test or the forward bending test (Figure 2) 25). A spinal deformity will be most noticeable when your child is in this position. Your child stands and bends forward at the waist, your doctor will observe your child from the back assessing for symmetry of the back from behind and beside your child, looking for a difference in the shape of the ribs on each side 26). A child with possible scoliosis will have a lateral bending of the spine, but the curve will cause spinal rotation and eventually a rib hump, which is visible on examination 27).
The standard screening test for scoliosis is the forward bending test. Your child will bend forward and your doctor will observe your child from the back.
With your child standing upright, your doctor will check to see if the hips are level, the shoulders are level, and that the position of the head is centered over the hips. He or she will check the movement of the spine in all directions.
To rule out the presence of a spinal cord or nerve problem, your doctor may check the strength in your child’s legs and the reflexes in the abdomen and legs.
Figure 2. Forward bending test (Adam’s forward bend test)
Tests
Although the forward bending test can detect scoliosis, it cannot detect the presence of congenital abnormalities. Imaging tests can provide more information.
X-rays. Images of your child’s spine are taken from the back and the side. The x-rays will show the abnormal vertebrae and how severe the curve is. If a doctor suspects that an underlying condition — such as a tumor — is causing the scoliosis, he or she may recommend additional imaging tests, such as an MRI.
Once your doctor makes the diagnosis of congenital scoliosis, your child will be referred to a pediatric orthopaedic surgeon for specialized care and further tests.
Computed tomography (CT) scan and 3D-CT. A CT scan can provide a detailed image of your child’s spine, showing the size, shape, and position of the vertebrae. To see the vertebrae better, your doctor may have a 3-D image made from the CT scan. This looks like a photograph of the bones (Figure 4).
Ultrasound. Your doctor will do an ultrasound of your child’s kidneys to detect any problems.
Magnetic resonance imaging (MRI) scan. Because an MRI can evaluate soft tissues better than a CT scan, an MRI will be done to check for abnormalities of the spinal cord at least once for every patient.
Figure 3. Cobb angle
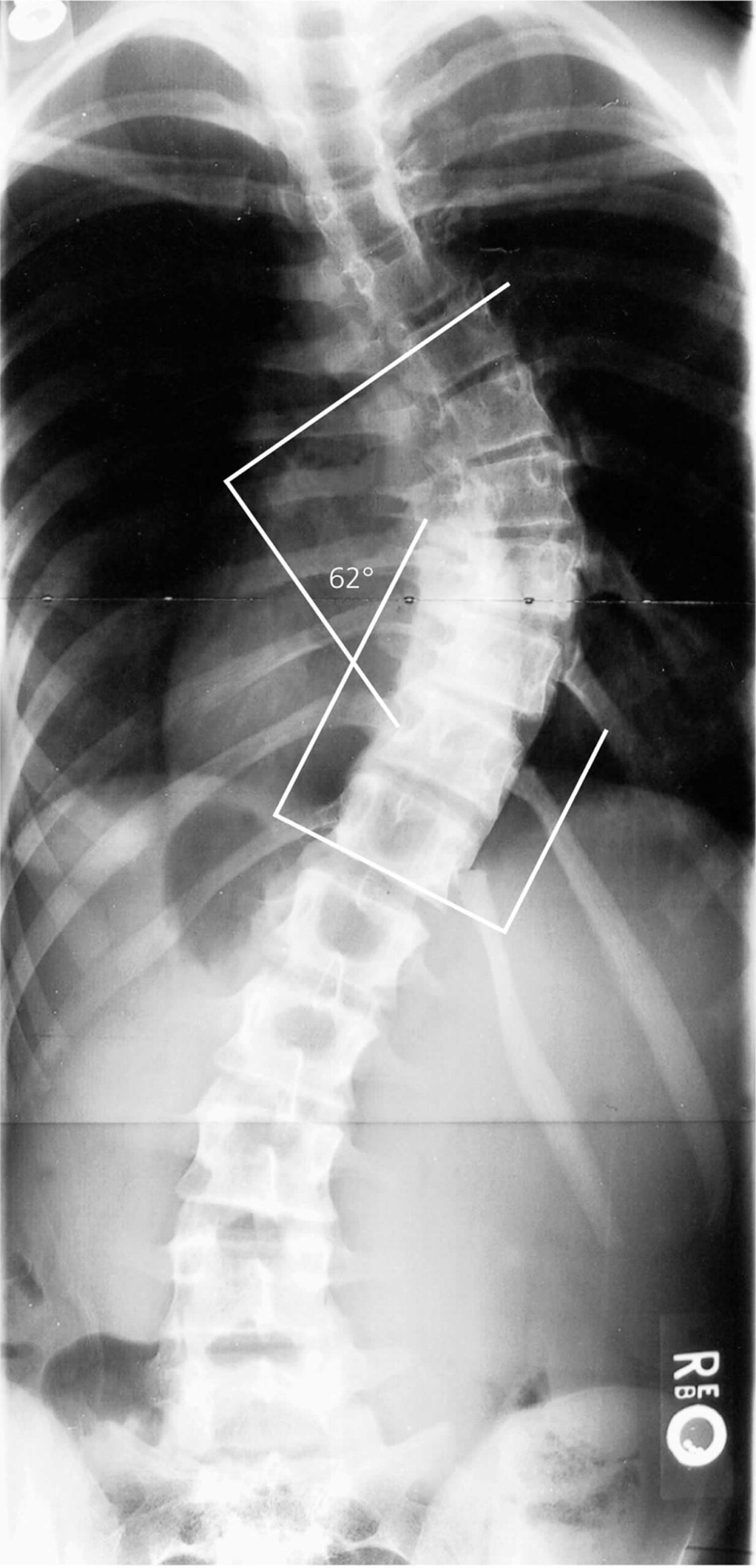
Figure 4. CT scan of hemivertebrae scoliosis
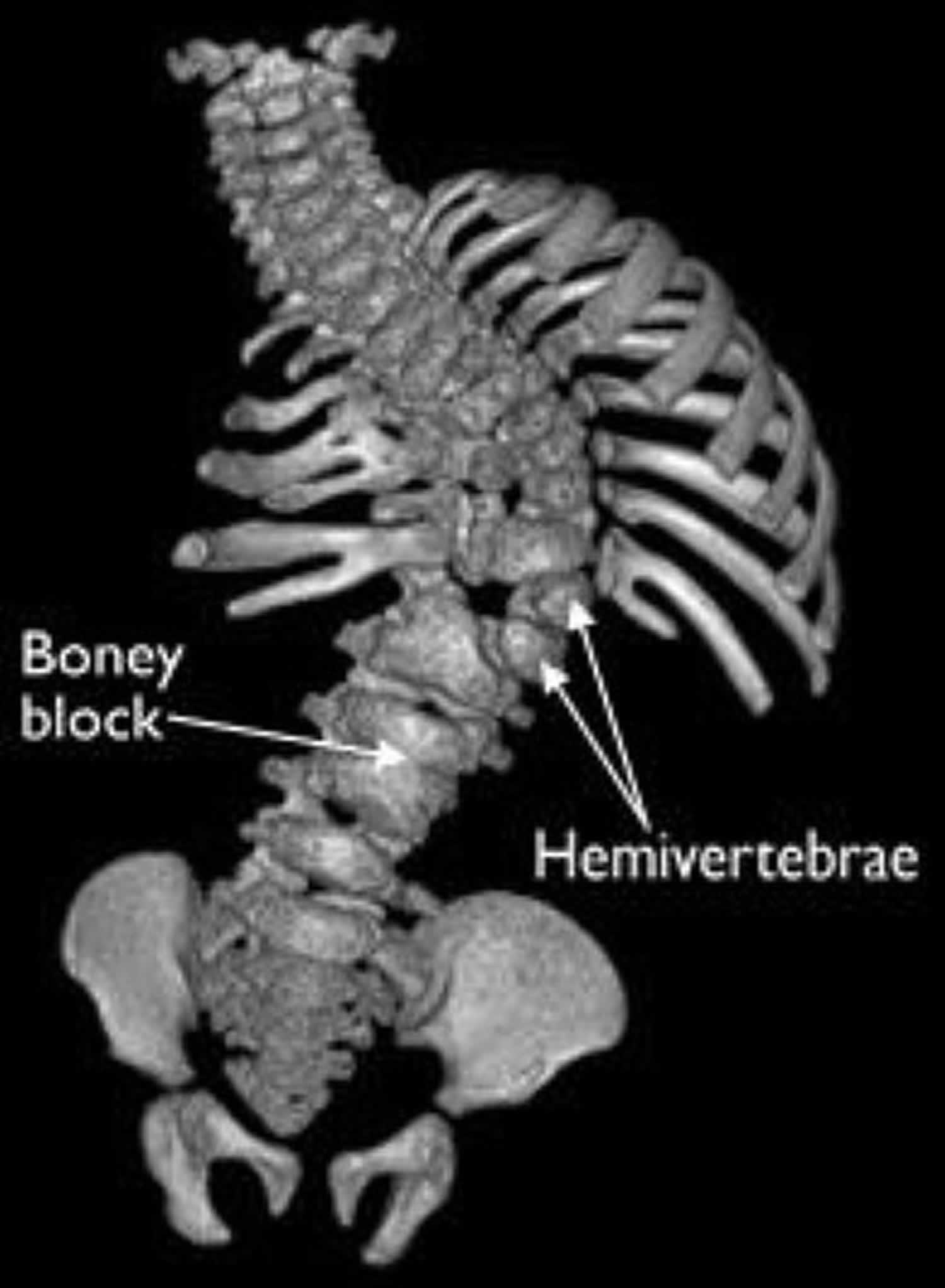
Footnote: This 3-D image from a CT scan shows hemivertebrae, as well as a fused, boney block.
Congenital scoliosis treatment
The presence of a scoliotic deformity at birth is a sign of worse prognosis and it requires treatment starting with the first days of life 29). Not all scolioses need bracing or surgery. 25% of them present a low progression rate or compensating defects of formation. These deformities have to be periodically evaluated and usually do not require surgery.
There are several treatment options for congenital scoliosis. In planning your child’s treatment, your doctor will take into account the type of vertebral abnormality, the severity of the curve, and any other health problems your child has.
Your doctor will determine how likely it is that your child’s curve will get worse, and then suggest treatment options to meet your child’s specific needs.
About 75% of congenital scoliosis require surgery. Surgery is indicated at the age of 1-4 years.
The essential criteria to choose the right moment of surgery is the magnitude of the scoliotic curve. Evaluation is performed by measuring the Cobb’s angle (Figure 3). Up to 40° of Cobb’s angle, the patient is periodically carefully monitored, at every 4-6 months. Above 40° Cobb’s angle, surgery is required. The presence of a respiratory disorder associated to some congenital malformations endangers the patient and imposes a more careful supervision and surgery as soon as possible. Congenital scoliosis with more than one fully segmented, successive hemivertebrae and severe deformities of the rib cage with thoracic insufficiency syndrome may be operated at the age of 8-12 months, even if Cobb’s angle is less than 40°.
Nonsurgical treatment
Observation
A child with a small curve that seems to be unchanging will be monitored to make sure the curve is not getting worse. Although it does not happen in every patient, congenital scoliosis curves can get bigger as the spine grows and the deformity of the back becomes more noticeable. It is likely that a curve in a young child will get worse because younger children still have a lot of growing to do.
Your doctor will follow the changes of your child’s curve using x-rays taken at 6- to 12- month intervals during the growing years.
Physical activity does not increase the risk for curve progression. Children with congenital scoliosis can participate in most sports and hobbies.
Bracing or casting
Braces or casts are not effective in treating the curvature caused by the congenitally abnormal vertebrae, but they are sometimes used to control compensatory curves where the vertebrae are normally shaped 30). This is because the primary deformity in congenital scoliosis is in the vertebrae rather than in the soft tissues, and the curves tend to be rigid. In addition, in cases where the natural history indicates a poor prognosis, orthotic treatment is contraindicated. Thus, contraindications for orthotic treatment are as follows:
- Short, stiff curves
- Unsegmented bar
- Congenital lordosis
- Congenital kyphosis
Congenital scoliosis responds well to bracing only when the scoliosis features long curves with good flexibility—best determined by bending or by traction radiographs—or when the scoliosis is unbalanced secondary to an unbalanced hemivertebra at the T12 or L5 level.
The brace of choice is the Milwaukee brace for high thoracic curves (apex T6 or above), because it avoids the constriction of the thorax that may occur with an underarm brace, and the thoracolumbosacral orthosis (TLSO) for lower curves. Winter et al indicated that certain patients did well in the Milwaukee brace for many years and that a few could even be treated permanently with an orthosis and avoid surgery 31).
The best results were in patients with mixed anomalies that were flexible and in patients with a progressive secondary curve. Braces are unlikely to be effective if the scoliosis is more than 40° or if less than 50% flexibility is established using side bending or distraction radiographs 32).
A significant shoulder elevation is best treated with a shoulder ring that is attached to the Milwaukee brace, and head support pads can be added to create a neutral head position if the patient has a head tilt. Only the Milwaukee brace and its modifications can control high curves.
Congenital scoliosis surgery
Surgical treatment is reserved for patients who:
- have curves that have significantly worsened during the course of x-ray monitoring
- have severe curves
- have a large deformity of the spine or trunk
- are developing a neurological problem due to an abnormality in the spinal cord
An important goal of surgery is to allow the spine and chest to grow as much as possible. There are several surgical options.
- Spinal fusion. In this procedure, the abnormal curved vertebrae are fused together so that they heal into a single, solid bone. This will stop growth completely in the abnormal segment of the spine and prevent the curve from getting worse.
- Hemivertebra removal. A single hemivertebra can be surgically removed. The partial correction of the curve that is achieved by doing this can then be maintained using metal implants. This procedure will only fuse two to three vertebrae together.
- Growing rod. Growing rods do not actually grow but can be lengthened with minor surgery that is repeated every 6 to 8 months. The goal of a growing rod is to allow continued growth while correcting the curve. One or two rods are attached to the spine above and below the curve. Every 6 to 8 months, the child returns to the doctor and the rod is lengthened to keep up with the child’s growth. When the child is full grown, the rod(s) are replaced and a spinal fusion is performed.
In situ spinal fusion
This procedure, even if being a safe technique, presents certain indications because correction possibilities are limited. It is indicated in progressive scoliosis presenting with a minimal deformity at surgery time, no more than 25°, with a limited area of no more than 5 vertebrae. It may be regarded as a prophylactic act in cases of high rate progression scoliosis with a fully segmented hemivertebra. This kind of arthrodesis insignificantly limits the growth in length of the spinal column and it may be used as an elective procedure in children with age ranging 1 to 4 years.
Present deformities correct slowly and the result is efficient if the growth potential is properly assessed by a CT-scan or MRI. In situ fusion may be performed by an open anterior approach, by thoracoscopy or by an open posterior approach through the pedicles. Usually, the surgeon chooses one of these options depending on its experience and the deformity’s location.
Convex hemiepiphysiodesis
The elective indication is congenital scoliosis due to defect of formation with the presence of a hemivertebra 33). During surgery, the correction of the curve is partially obtained, the remaining correction being achieved slowly in time because of the ablation of the intervertebral disks on the convex side.
Best results are achieved if the procedure is performed in a child with age ranging 1 to 4 years. All over, in the long term, same as for in situ fusion, the correction limit is up to 20-25°. Argues about its indication are present in literature due to the fact that expected results were not obtained. Good results may be obtained if the curve is less than 30°, if it is associated to posterior fusion, the progressive rate before surgery being constantly of 8-10° per year and the malformation being a fully segmented vertebra 34). The approach is via a thoracotomy or an abdomino-thoracotomy on the side of the convexity depending on the level of the malformation.
Excision of the hemivertebra
The excision of the hemivertebra is recommended if the curve progresses rapidly. It becomes an emergency in the presence of spinal canal stenosis or disk hernia, as a measure of decompression.
Excision of the hemivertebra is the best treatment method in comparison to in situ fusion and hemiepiphysiodesis. Maximal efficiency is obtained if performed at the age of 1-4 years, when the hemivertebra has a thoracic, lumbar or lumbo-sacral position and there is an imbalance of the trunk. Excision of the hemivertebra may be performed by an anterior or a posterior approach 35). A posterior approach is indicated in case of an isolated resection. A posterior and anterior simultaneous approach allows a complete excision of the adjacent disks of the hemivertebra by a circumferential exposure. This allows total visibility when excising the hemibody and the pedicle. This kind of approach requires the reposition of the patient during surgery.
The approach is variable depending on the site of the hemivertebra: Transthoracic for T4-T11, Hodgson (transpleural, retroperitoneal for T9-L5), Burnei (transthoracic, retropleural for T2-T11) and Mirbaha (extrapleural, retroperitoneal for T11-L5).
Some surgeons prefer a successive approach during the same surgical procedure by rotating the patient in the same sterile field, next instrumenting the spine after the hemivertebral excision 36). During 1998 and 2006 Burnei et al 37) practiced 23 procedures with a medium correction of 64% (an average of 41° preoperatively to an average of 16° postoperatively). The evolution in time of the deformity has been of about 3-4° per year, requiring a conversion of the anterior instrumentation to a posterior one at puberty in order to stabilize the spine.
Posterior excision of the hemivertebra ensures very good results. This method is best for a hemivertebra located in the thoracolumbar junction and is accompanied by kyphosis 38).
Growing rods
The first to initiate this concept was Harrington in 1960. The promoter of this method is Akbarnia 39) who improved the distraction device by using tandem connectors on 2 rods with distraction possibilities. He succeeded in correcting the angle from 82° to 38° in cases of early onset scoliosis and ensured a 1.2 cm/ year growth of the spine 40).
This method is a fusionless curve correcting one. Growing rods have become implants suitable in congenital scoliosis with large curves with normal disks above and below the malformation or the curve’s apex and with flexibility of the upper and lower segments of the spine. Growing rods are more suitable due to the fact that children younger than 5 years treated by thoracic fusion developed important respiratory problems finally leading to respiratory insufficiency. Data regarding physiopathology, growth and development of the spine and thoracic organs up to 5 years showed that the height and volume of the vertebra are of about 70% of an adult. That is why congenital scoliosis is associated with a diminished trunk height and, as a consequence, a shorter stature. Arthrodesis in these children will lead to a more reduced trunk height and thoracic volume. Nowadays, fusion is avoided in children of less than 10 years of age, just as Harrington predicted.
Growing rods are distracted at every 6 months. Transpedicular screws have to be used with caution in the upper thoracic part in very young children, but if required at least 4 should be used in order to spread the local tension 41). If the established spinal anchoring points prove to be anomalous not allowing the placement of implants, a VEPTR (Vertical Expandable Prosthetic Titanium Rib) should be used.
Halo traction
If the spinal column in congenital scoliosis is very stiff halo traction should be used before surgery. Traction is indicated even in some cases with neurological problems. It is a gravitational traction allowing the patient to sit in bed or walk with a wheelchair or with any other walking device. Gravity will ensure a partial reduction of the curve up to 70% before surgery without any neurological issues. If required, the traction weight will be diminished or even suppressed.
VEPTR (Vertical Expandable Prosthetic Titanium Rib)
This device ensures a progressive correction of the curve and the expansion of the thorax by a thoracotomy. The elective indication is in cases of scoliosis associated to rib synostoses and thin thorax that induce a defective lung development and evolve to thoracic insufficiency if not treated 42). Thoracic volume may be increased by the use of VEPTR, fixed rib-to-rib or more frequently rib-to-spine. If the deformity is a lumbar one and the pelvis is unbalanced, a device rib-to-ilium is indicated. Expansion thoracoplasty resides in the axial sectioning of the bony synostotic rib plate followed by intra-operative distraction maintained next by the aid of VEPTR (Vertical Expandable Prosthetic Titanium Rib).
Contraindications of VEPTR consist in inadequate strength of bone for the attachment of the device, absence of ribs for attachment, inadequate soft tissue for coverage, age of less than 6 months, absent diaphragmatic function, allergy to material, infection at the operative site and age beyond skeletal maturity or spinal canal stenosis.
In our series, we met a case of congenital scoliosis with spinal stenosis due to the protrusion of the 11th and 12th rib into the canal, which were removed before scoliosis correction 43).
This method allows an important correction of the Cobb angle up to 60% and the vital capacity of the lung remains the same or even it increases in some cases. As a rule, the spine will grow and the volume of the hemithorax increases without an improvement of the functional pulmonary volume. The current results showed a benefic result especially in congenital scoliosis associated to chest wall deformities 44). If needed, the device may be repositioned or converted. The complications in the use of VEPTR are bone erosion, skin breakthrough, infection, post-operative pain, device fracture due to stress fatigue, scapular elevation, brachial plexus palsy 45) and medullar lesion, as an exception.
The thoracoplasty is adequate to the simultaneous treatment of the scoliotic curve, thoracic expansion and chest wall lesions 46). A proper correction of the thoracic deformity may require the use of 2 or more such devices.
Guided-growth implants
Growing rods and VEPTR (Vertical Expandable Prosthetic Titanium Rib) require periodic minimal invasive procedures for distraction. The use of guided-growth implants like Shilla or a modified Luque trolley presents the advantage of an in situ correction and arthrodesis of the apical site of the deformity. Spinal growth is ensured and guided by the implant below and above the apex of the curve 47). The guided-growth implants are indicated in early onset, neuro-muscular and syndromic scoliosis in children less than 10 years of age.
Vertebrectomy
Vertebrectomy is the most radical of all procedures for congenital scoliosis. It consists of the removal of two or more vertebrae in their entirety, including the pedicles from both sides as well as the laminae and bodies. Vertebrectomy is performed to create mobility, but it is carried out at the price of instability. The procedure is neurologically risky and must be accompanied by appropriate spinal cord monitoring and wakeup tests. It should be reserved for the most severe deformities and performed only by highly skilled spinal surgeons 48).
Congenital scoliosis surgery recovery
Rehabilitation. Young children usually recover quickly from surgery and are discharged from the hospital within 1 week. Depending on the operation, a child may need to wear a cast or brace for 3 to 4 months.
Once they are healed, children are allowed to participate in most of the activities that they had previously participated in.
Congenital scoliosis prognosis
Congenital scoliosis detected at an early age is one of the most challenging types of scoliosis to treat. The curves can be large to begin with and because children have so much growth ahead of them, the chance of severe curve is high.
Although fusion of vertebrae at an early age results in the spine and trunk being shorter than they would have been, children can have outstanding results and achieve normal, or near-normal, function.
References [ + ]





{kind=link}