






Leaking breast milk
Some nursing moms leak or spray milk from their breasts, especially when their breasts are full. Leaking is most likely to happen in the morning (when milk supply is at its peak) and during feedings (when one side leaks while the baby is nursing from the other side).
Some nursing moms leak only during the early weeks of breastfeeding, while others leak until their baby is weaned. For some women, leaking starts during pregnancy.
Some women continue to produce milk up to 2 years after they have stopped breastfeeding.
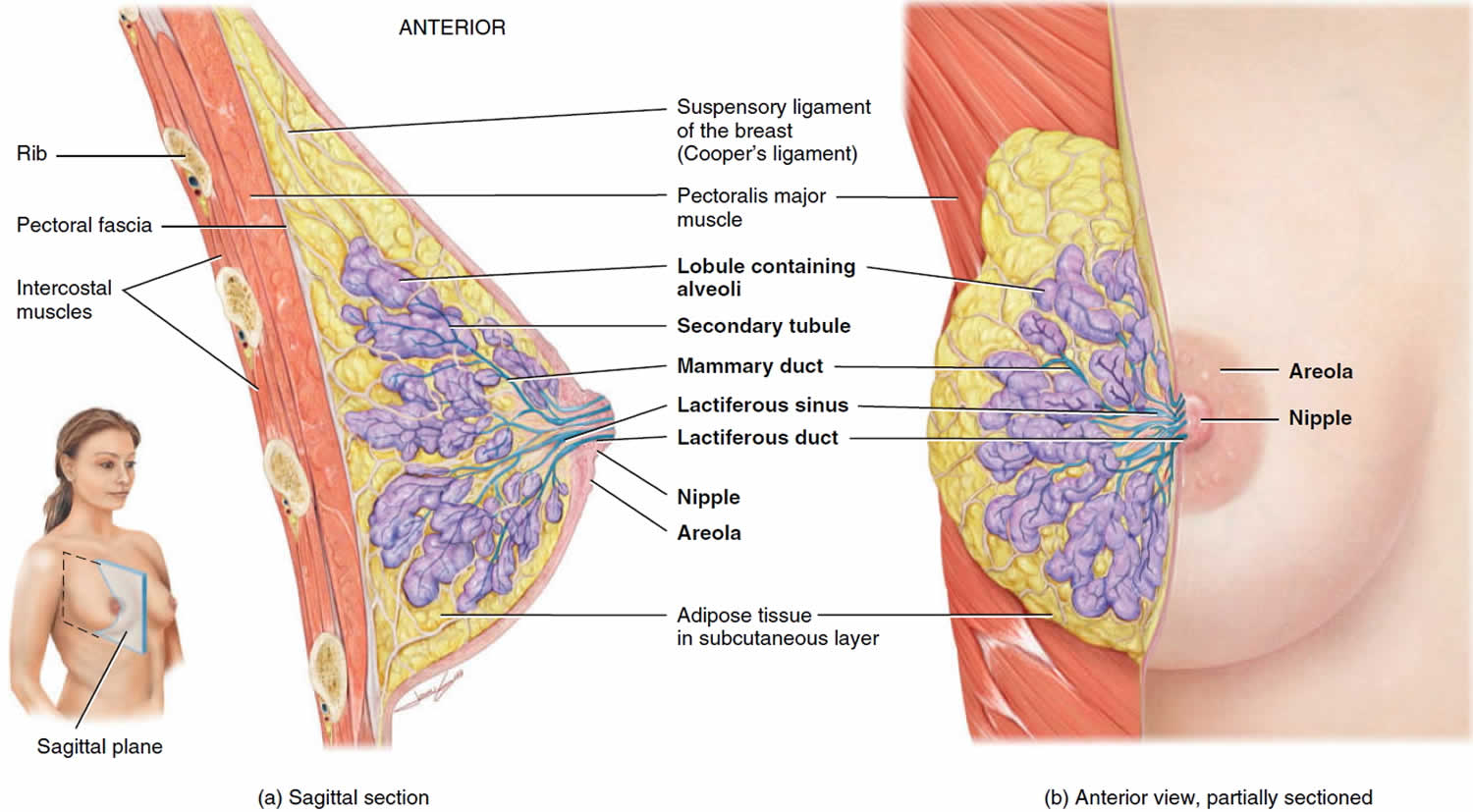
Figure 1. Normal breast
Breast leaking during pregnancy
Some women notice leaking from their nipples during pregnancy, and this is normal. In pregnancy, the breasts may start to produce milk weeks or months before you are due to have your baby.
If your nipples are leaking, the substance is usually colostrum, which is the first milk your breasts make in preparation for feeding your baby. Leaking is normal and nothing to worry about.
If it bothers you, you can try putting a tissue or an absorbent breast pad (sometimes called maternity breast pads, or nursing pads) in your bra to absorb the milk. Breast pads are available in some pharmacies and mother and baby shops.
If the milk leaking from your breasts becomes bloodstained, talk to your doctor.
How long will my breasts keep leaking?
Some women continue to leak for as long as they’re nursing, but many find that the problem goes away once their baby gets the hang of breastfeeding – usually within the first six to 10 weeks.
In the meantime, remember that your leaking breasts are a sign of your body’s efficiency making milk for your baby. And don’t worry – when the leaking eventually stops, you’ll still be making plenty of milk to meet your baby’s needs.
Leaking breast milk causes
Your breasts may leak when they become so full of milk that they overflow. Leaking is common in women who produce more milk than their baby needs. Or you might leak when your let-down reflex – which releases the milk – kicks in. This can happen when your nipples rub against a bed sheet, bath towel, or clothing, or when you hear a baby cry.
The let-down reflex is what makes your breastmilk flow. When your baby sucks at the breast, tiny nerves are stimulated. This causes two hormones – prolactin and oxytocin – to be released into your bloodstream. Prolactin helps make the milk, while oxytocin causes the breast to push out the milk. Milk is then released or let down through the nipple.
Some women feel the let-down reflex as a tingling sensation in the breasts or a feeling of fullness, although others don’t feel anything in the breast.
Most women notice a change in their baby’s sucking pattern as the milk begins to flow, from small, shallow sucks to stronger, slower sucks.
Some women also notice, while feeding or expressing from one breast, that milk drips from the other.
Your let-down reflex needs to be established and maintained to ensure a good supply of milk. This reflex requires no thought, unless you are having problems with breastfeeding.
Once you begin to recognize when your baby wants to eat, your breasts shouldn’t leak as often. Going too long without breastfeeding or pumping (more than three hours) can also cause leaking. If you are changing your nursing schedule from nursing on demand to nursing less often, you should expect a certain amount of leaking during this period. It will probably continue until your body has adjusted to the new schedule.
The let-down reflex occurs:
- in response to your baby sucking at the breast
- hearing, seeing or thinking about your baby
- using a breast pump, hand expressing or touching your breasts or nipples
- looking at a picture of your baby
- hearing your baby (or another baby) cry
The let-down reflex generally occurs 2 or 3 times a feed. Most women only feel the first, if at all. This reflex is not always consistent, particularly early on, but after a few weeks of regular breastfeeding or expressing, it becomes an automatic response.
The let-down reflex can also occur with other stimulation of the breast, such as by your partner.
The let-down reflex can be affected by stress, pain and tiredness. There are many things to try if you are experiencing difficulty.
- Ensure that your baby is correctly attached to the breast. A well-attached baby will drain a breast better.
- Feed or express in a familiar and comfortable environment.
- Try different methods to help you to relax: calming music, a warm shower or a warm washer on the breast, some slow deep breathing, or a neck and shoulder massage.
- Gently hand express and massage your breast before commencing the feed.
- Look at and think about your baby.
- If you are away from your baby, try looking at your baby’s photo.
- Always have a glass of water nearby.
Milk let-down can be quite forceful, particularly at the beginning of a feed. This fast flow of milk can upset your baby, but it might not mean you have oversupply. It can be managed through expressing before a feed, reclining slightly and burping your baby after the first few minutes. If you continue to have problems, seek advice.
What can I do about my leaking breasts?
Until you and your baby fine-tune breastfeeding, many sensations and thoughts can trigger your let-down reflex. Leaking breasts can be embarrassing, but should stop once breastfeeding is fully established.
In the meantime you can feed regularly before your breasts become too full, apply firm pressure to your breasts when you feel the first sensation of let-down, use breast pads and wear clothing that disguises milk stains.
If your breasts are full but your baby isn’t ready to eat, it may help to “pump to comfort.” This means pumping just enough to make your breasts compressible and comfortable, but not so much that you boost your milk supply. Manually expressing a little milk is another option.
It’s important to relieve the pressure, otherwise you could develop a clogged breast duct or mastitis, a breast infection.
You’ll soon establish a breastfeeding rhythm that works for you and your baby. Once you’re in sync with each other, you’ll probably produce just the right amount of milk for each upcoming feeding.
Here are other ways to deal with leaking breasts:
- Apply pressure. If you feel let-down happening at an awkward moment (like if you’re chatting with a co-worker about your baby and your milk starts to drip), cross your arms over your breasts and press firmly. If you’re sitting at a table, cup your chin in your hands and press your forearms into your breasts.
- Use nursing pads. Tuck nursing pads inside your bra to absorb leaks. You can buy disposable or cloth pads online or at the drugstore. Or make your own cloth pads from cut-up cloth diapers. Be sure to change the pads when they get damp so bacteria and fungi won’t grow on your nipples. A warm, moist environment can lead to fungal infections, such as thrush.
- Be prepared. If one breast always leaks when your baby is nursing on the other, put a cloth over that breast or a nursing pad inside your bra ahead of time.
- Dress for leaks and pack extras. When you’re out and about, bring along some nursing pads and extra top. Try wearing prints – they’re great for camouflaging milk stains. Or carry a jacket or sweater that you can throw on if you notice your breasts leaking.
If you want, you can try to collect your leaking breast milk to save for later with a product like Milkies Milk-Saver and Lacti-Cups. If you are concerned about leaking milk, call your lactation consultant.






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}