Contents
Acetabular dysplasia
Acetabular dysplasia also called hip dysplasia, is a disorder that occurs when the acetabulum (hip socket) is shallow and doesn’t provide sufficient coverage of the femoral head (ball), causing instability of the hip joint. Over time, this instability causes damage to the labrum and cartilage lining of the joint, which can result in pain and development of early hip osteoarthritis 1). Hip joints which are abnormally shallow are predisposed to progressive damage to the cartilage, leading to osteoarthritis. Acetabular dysplasia is one of the leading causes for the development of hip joint osteoarthritis, particularly in women. Many patients worldwide have undergone hip arthroplasty due to secondary osteoarthritis caused by acetabular dysplasia, and the incidence has been known to be more frequent in Asia 2). Classic descriptions of acetabular dysplasia include anterosuperior acetabular deficiency 3). However, acetabular retroversion has been reported in approximately one in seven hips with acetabular dysplasia 4).
Acetabular dysplasia can be a result of developmental dislocation of the hip (DDH) that was treated in infancy or childhood. Therefore, children treated for hip dysplasia should be closely followed by a physician until their bones are fully grown. In babies and children with developmental dysplasia (dislocation) of the hip (DDH), the hip joint has not formed normally. The ball is loose in the socket and may be easy to dislocate. Although developmental dislocation of the hip (DDH) is most often present at birth, it may also develop during a child’s first year of life. Recent research shows that babies whose legs are swaddled tightly with the hips and knees straight are at a notably higher risk for developing developmental dislocation of the hip (DDH) after birth. As swaddling becomes increasingly popular, it is important for parents to learn how to swaddle their infants safely, and to understand that when done improperly, swaddling may lead to problems like developmental dislocation of the hip (DDH).
Sometimes acetabular dysplasia can develop as the result of other childhood hip conditions such as infection, trauma or Perthes disease.
Acetabular dysplasia can exist as a mild issue that can take years to decades for symptoms to develop. Patients who have been diagnosed with acetabular dysplasia often have a family history of early hip osteoarthritis or hip dysplasia.
The preferred treatment for adolescents and young adults with acetabular dysplasia is a periacetabular osteotomy (PAO), which is a surgical procedure that repositions the acetabulum into a more stable position with the acetabulum covering the femoral head properly. The surgery improves hip function, reduces pain, and stops the damage occurring inside of the hip joint.
During a periacetabular osteotomy (PAO), the acetabulum is repositioned to cover more of the femoral head in order to improve the stability of the hip joint. The PAO surgery improves hip function, decreases hip pain, and stops the damage occurring inside of the joint that can lead to hip arthritis over time.
The periacetabular osteotomy (PAO) preserves the integrity of the pelvic ring, but allows precise and full correction of even severe hip dysplasia. It involves cutting the pelvis around the entire acetabulum, which is then repositioned into a position that better covers the femoral head. Usually, 3 or 4 screws are used to hold the acetabulum in its new position. Over time, new bone will grow where the cuts are made, fusing the acetabulum to the rest of the pelvis.
Occasionally, the hip joint may need to be opened or a hip arthroscopy may need to be performed at the same time as a periacetabular osteotomy (PAO) in order to repair damage inside of the joint, such as a labral tear.
The recovery and expectation for patients who have a periacetabular osteotomy (PAO) performed are:
- In the hospital for 3-5 days after surgery
- Walking and using crutches 1-2 days after surgery
- Using crutches for 6-8 weeks after surgery
- Most patients are completely healed and back to sports 3-6 months after surgery
Figure 1. Acetabular hip dysplasia

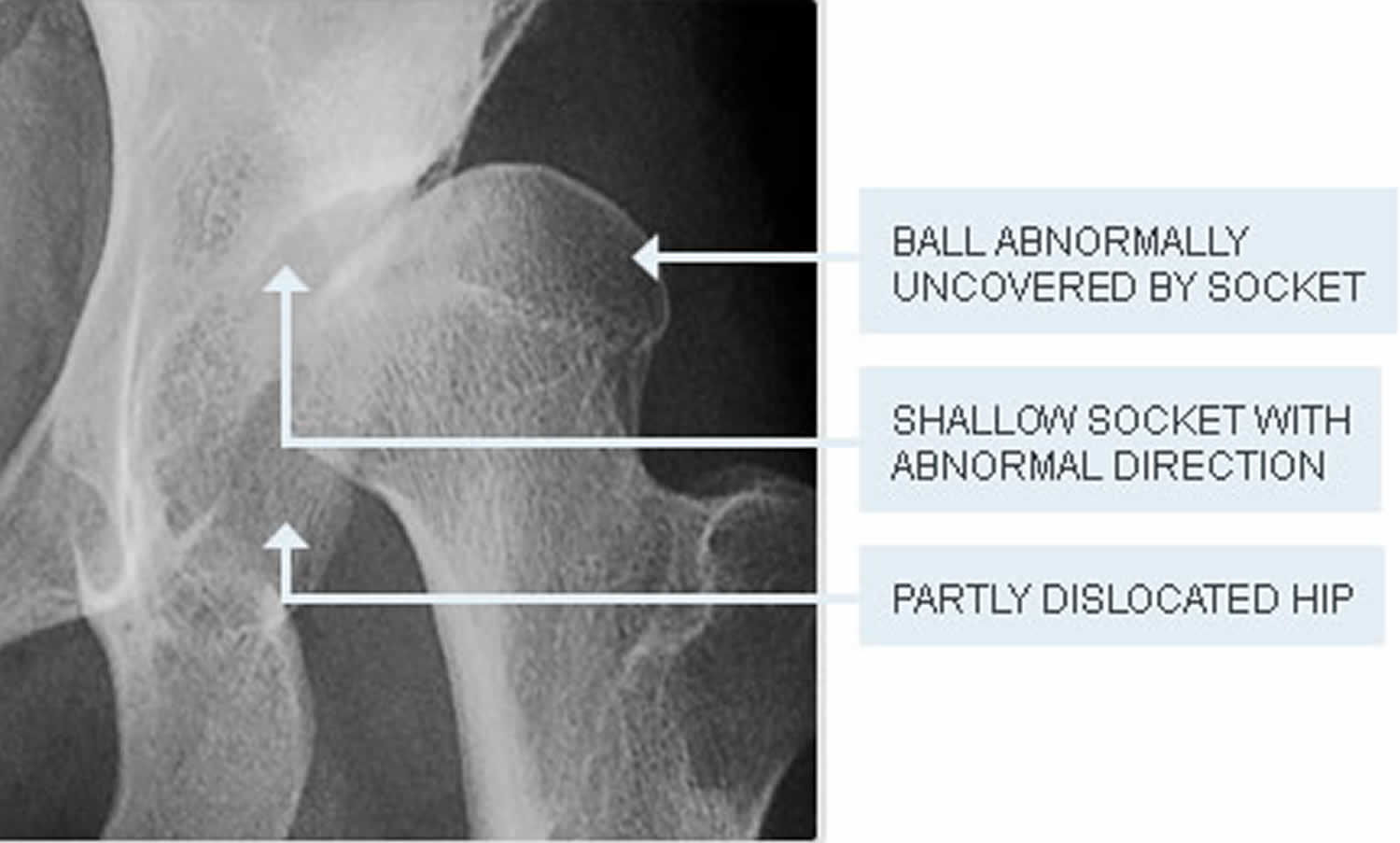
Footnote: Acetabular hip dysplasia. The acetabulum is not providing sufficient coverage of the femoral head, causing instability of the hip joint.
Hip joint anatomy
The hip is one of the body’s largest joints. It is a “ball-and-socket” joint. The socket is formed by the acetabulum, which is a part of the large pelvis bone. The ball is the femoral head, which is the upper end of the femur (thighbone).
The bone surfaces of the ball and socket are covered with articular cartilage, a smooth, slippery substance that protects and cushions the bones and enables them to move easily.
The acetabulum is ringed by strong fibrocartilage called the labrum. The labrum forms a gasket around the socket, creating a tight seal and helping to hold the femoral head in place.
In patients with acetabular hip dysplasia, the acetabulum is shallow, meaning that the ball, or femoral head, cannot firmly fit into the socket. As a result of this abnormality, the way that force is normally transmitted between the bone surfaces is altered. The labrum can end up bearing the forces that should normally be distributed evenly throughout the hip joint. In addition, more force is placed on a smaller surface of the hip cartilage and labrum. Over time, the smooth articular cartilage becomes frayed and wears away and the labrum becomes torn or damaged. These degenerative changes can progress to early osteoarthritis.
The severity of hip dysplasia can vary from patient to patient. In mild cases, the head of the femur may simply be loose in the socket. In more severe cases, there may be complete instability in the joint and/or the femoral head may be completely dislocated out of the socket.
Figure 2. Hip joint anatomy

Acetabular dysplasia causes
An abnormally shallow acetabulum can result from several developmental diseases of the hip joint. Invariably, acetabular dysplasia usually results from developmental dysplasia of the hip (DDH), which is the most common developmental hip disease, that is undiscovered or untreated during infancy or early childhood. In addition, other childhood bony diseases, such as slipped capital femoral epiphysis and Legg-Calves-Perthes disease, can also produce residual acetabular dysplasia 5).
Developmental dislocation (dysplasia) of the hip (DDH) can occur in families, passed on from one generation to the next. It can be present in either hip and in any individual. It usually affects the left hip and occurs more often in:
- Girls
- First-born children
- Babies born in the breech position
Acetabular dysplasia can also arise secondary to certain neuromuscular conditions, such as cerebral palsy (CP) 6), Charcot-Marie-Tooth disease, myelomeningocele, and arthrogryposis 7). Acetabular dysplasia may be seen as an associated finding in syndromes such as Ehlers-Danlos syndrome and Larson syndrome. Essentially, any condition that interferes with the interdependent relation between the femoral head and the acetabulum during the growth period can lead to acetabular dysplasia.
Acetabular dysplasia symptoms
The symptoms of acetabular dysplasia are directly related to its severity. Acetabular hip dysplasia in younger children is not a painful condition. However, over time, pain results when the altered forces in the hip cause degenerative changes to occur in the articular cartilage and the labrum. Patients with mild acetabular dysplasia may remain pain-free until the fourth or fifth decade of life, or they may experience only vague discomfort with strenuous weightbearing activities, particularly during the most productive years of their life. In the mild forms of pain-free acetabular dysplasia, abductor lurch or a limp is the only presenting symptom. Patients with severe acetabular dysplasia begin to experience pain in the second decade of life.
In most cases, symptoms of acetabular dysplasia may include:
- Pain located in the groin area, although it may sometimes be more toward the outside of the hip
- Pain in the front of the hip
- Pain in the muscles around the hip
- Pain occasional and mild initially, but may increase in frequency and intensity over time
- Pain that is worse with activity or near the end of the day
- Feelings of instability or the hip/leg “giving way”
Some patients may also experience the feeling of locking, catching, or popping within the groin.
The patient’s activity level, functional status, and expectations are also contributing factors in the genesis of the symptoms. For instance, a severely dysplastic acetabulum in a nonambulatory cerebral palsy (CP) patient may be asymptomatic, whereas mild acetabular hip dysplasia in an adolescent athlete may be painful and may limit the activity level significantly. Thus, characterization of the patient’s symptoms should be individualized and should be correlated with the pathology underlying the residual acetabular dysplasia.
Lateral abductor-fatigue pain should be differentiated from anterior groin pain that is intra-articular in origin and indicates joint overload, with possible labral pathology or cartilage damage; the onset of degenerative changes is expected in such cases.
Acetabular dysplasia diagnosis
During the physical examination, your doctor will discuss your child’s medical history and symptoms. He or she will move your child’s hip in different directions to assess the range of motion and duplicate the pain or discomfort he or she is feeling.
Acetabular dysplasia is carefully diagnosed through several different tests:
- Overall range of motion of the hip in flexion, extension, internal and external rotation
- Observation of gait
- Muscle strength and reflexes
- Positive anterior apprehension test: Tests for instability of the hip when it is extended and turned out.
- Positive anterior impingement test: Tests for irritation of the acetabular labrum when the hip is flexed and turned inwards.
- Imaging: X-rays and MRIs show different views of the hip, the degree of dysplasia, and any damage to the cartilage and labrum.
Acetabular dysplasia treatment
Treatment for acetabular hip dysplasia focuses on delaying or preventing the onset of osteoarthritis while preserving the natural hip joint for as many years as possible.
Treatment of acetabular dysplasia is fundamentally surgical (ie, pelvic osteotomy); little in the way of nonsurgical treatment can be offered 8). Symptomatic medical therapy, muscle-strengthening exercises, and weight-relieving exercises can be provided initially until the execution of the pelvic osteotomy. The goals are to eliminate hip irritability and instability and minimize the chances of further hip-joint degeneration.
In deciding whether to reduce the hips, a distinction should be made between a patient who presents later with a unilateral dislocation and one who presents with bilateral hip dislocations. There are differences in the long-term health of the hip: Bilateral dislocated hips tend to have better function without symptoms into adulthood, whereas a unilateral dislocation is more likely to have significant disability. In general, reduction of a unilateral hip dislocation is recommended up to 6-8 years of age; bilateral dislocations are more likely to be left alone at that age.
Nonsurgical treatment
Your doctor may recommend nonsurgical treatment if your child has mild hip dysplasia and no damage to the labrum or articular cartilage. Nonsurgical treatment may also be tried initially for patients who have such extensive joint damage that the only surgical option would be a total hip replacement.
Common nonsurgical treatments for acetabular dysplasia include:
- Observation. If your child has minimal symptoms and mild acetabular dysplasia, your doctor may recommend simply monitoring the condition to make sure it does not get worse. Your child will have follow-up visits every 6 to 12 months so that the doctor can check for any progression that may warrant treatment.
- Lifestyle modification. Your doctor may also recommend that your child avoid the activities that cause the pain and discomfort. For a child who is overweight, losing weight will also help to reduce pressure on the hip joint.
- Physical therapy. Specific exercises can improve the range of motion in the hip and strengthen the muscles that support the joint. This can relieve some stress on the injured labrum or cartilage.
- Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen and naproxen, can help relieve pain and reduce swelling in an arthritic joint. In addition, cortisone is an anti-inflammatory agent that can be injected directly into a joint. Although an injection of cortisone can provide pain relief and reduce inflammation, the effects are temporary.
Surgical treatment
Your doctor may recommend surgery if your child is experiencing pain and has limited damage to the articular cartilage in his or her hip. The surgical procedure most commonly used to treat acetabular hip dysplasia is an osteotomy or “cutting of the bone.” In an osteotomy, the doctor reshapes and reorients the acetabulum and/or femur so that the two joint surfaces are in a more normal position.
There are different types of osteotomies that can be performed to treat acetabular hip dysplasia. The specific procedure your doctor recommends will depend on a number of factors, including:
- Your child’s age
- The severity of the dysplasia
- The extent of damage to the labrum
- Whether osteoarthritis is present
- The number of remaining growing years
Periacetabular osteotomy (PAO)
Currently, the osteotomy procedure most commonly used to treat adolescent hip dysplasia is a periacetabular osteotomy (PAO). “Periacetabular” means “around the acetabulum.”
In most cases, periacetabular osteotomy (PAO) takes from 2 to 3 hours to perform. During the surgery, the doctor makes four cuts in the pelvic bone around the hip joint to loosen the acetabulum. He or she then rotates the acetabulum, repositioning it into a more normal position over the femoral head. The doctor will use x-rays to direct the bony cuts and to ensure that the acetabulum is repositioned correctly. Once the bone is repositioned, the doctor inserts several small screws to hold it in place until it heals.
- Arthroscopy. In conjunction with periacetabular osteotomy (PAO), your doctor may use hip arthroscopy to repair a torn labrum. During arthroscopy, the doctor inserts a small camera, called an arthroscope, into the joint. The camera displays pictures on a television screen, and your doctor uses these images to guide miniature surgical instruments. Arthroscopic procedures may include:
- Labral refixation. In this procedure, the doctor trims the torn and frayed tissue around the acetabular rim and reattaches the torn labrum to the bone of the rim.
Debridement. In some cases, simply removing the torn or weakened labral tissue can provide pain relief.
Figure 3. Periacetabular osteotomy (PAO)

Figure 4. Periacetabular osteotomy (PAO) combined with a femoral osteotomy
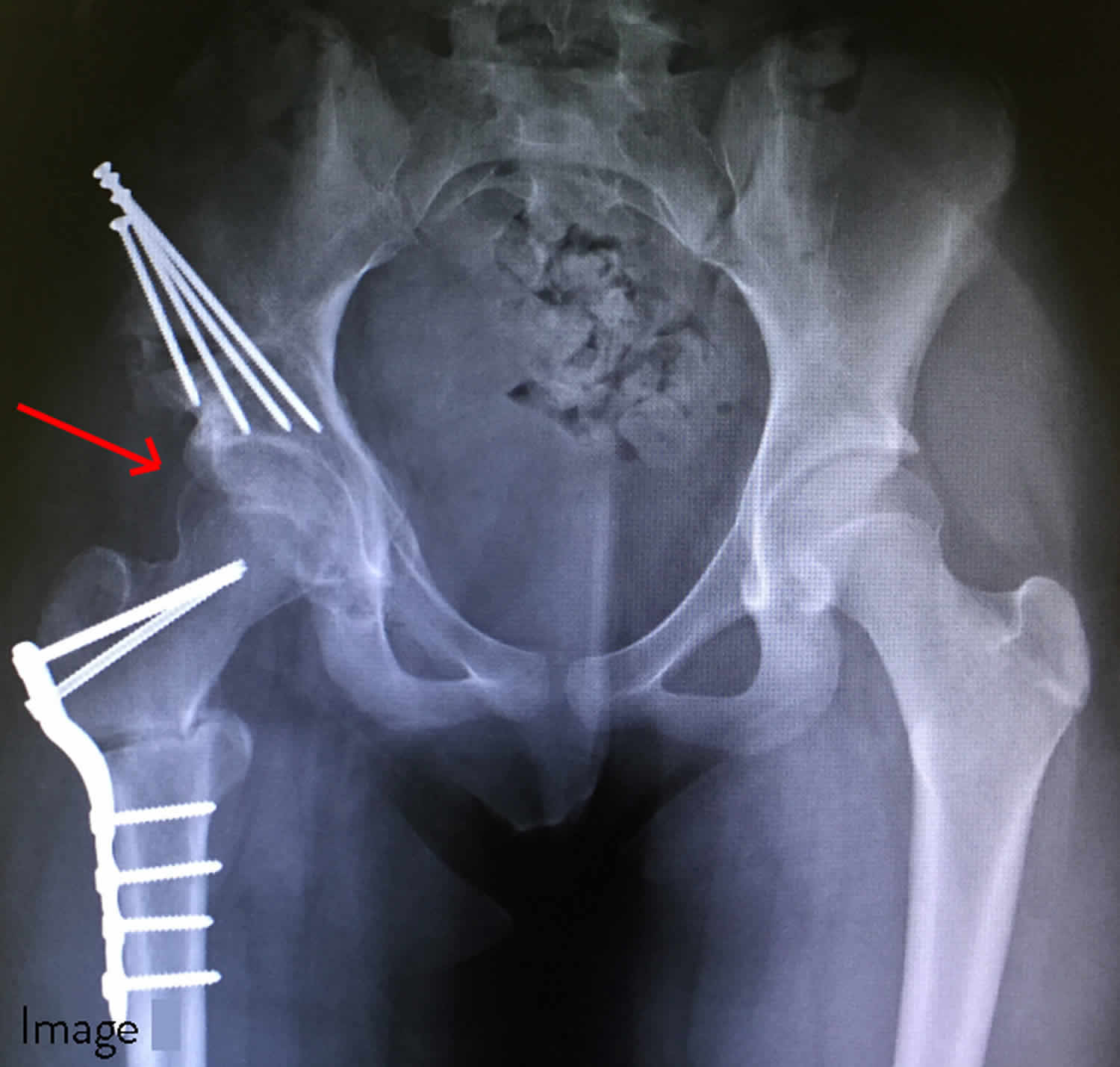
Footnote: The red arrow points to the right hip after a periacetabular osteotomy (PAO) combined with a femoral osteotomy has been performed. The femoral head is now properly covered and the femoral head is pointing towards the center of the socket. The right hip appears more symmetric with the normal left hip.
Surgical somplications
As with any surgical procedure, there are risks involved with periacetabular osteotomy (PAO). Your doctor will discuss each of the risks with you and will take specific measures to help avoid potential complications.
Although the risks are low, the most common complications include:
- Infection
- Blood clots
- Injuries to blood vessels and nerves
- Persistent hip pain
- Failure of the osteotomy to heal
Recovery
Your child will remain in the hospital for 2 to 4 days after surgery. During this time, he or she will be monitored and given pain medication.
In most cases, full weight-bearing will not be allowed on the operated leg for 6 to 12 weeks while the bones heal in their new position. During this time, your child will need to use crutches.
About 6 weeks after surgery, your child will have a follow-up visit with the doctor. X-rays will be taken so that the doctor can see how well the periacetabular osteotomy (PAO) has healed. During your visit, the doctor will determine when it is safe to put weight on the leg and when physical therapy can begin. The physical therapist will show your child specific exercises to help maintain range of motion and restore strength and flexibility in the hip joint.
Acetabular dysplasia prognosis
It is useful to consider acetabular dysplasia as a disorder with graded severity, ranging from a very mild (borderline) deformity through to very severe joint irregularity. The outcome for dysplasia is significantly influenced by the amount of dysplasia present. Some patients with mild forms of dysplasia may indeed not develop arthritis into the future, or alternatively have outcomes very similar to patients who do not have dysplasia. For this reason, not all patients with acetabular hip dysplasia require corrective surgical treatment, particularly if only mild deformity is present. In this respect, rather than asking “do I have have dysplasia?” a much more practical question is to to ask “how much dysplasia is present?”.
Periacetabular osteotomy is usually successful in delaying the need for an artificial hip joint and relieving pain. Whether or not a total hip replacement will be needed in the future depends on a number of factors, including the degree of osteoarthritis that was present in the joint when the periacetabular osteotomy (PAO) was performed.
How long will my hip joint last?
This is sometimes a difficult question to answer. Once the hip becomes painful, acetabular dysplasia predictably causes progressive damage to the joint, but the progression can be very slow. Most patients experience ongoing discomfort which gradually worsens over many years, even decades. Patients with very shallow hip joint sockets who have developed symptoms around the age of 20 rarely get beyond their early to mid- thirties without requiring an artificial joint replacement.
Why not just wait until I develop severe arthritis, then get an artificial joint replacement?
This is certainly an option. Artificial joint replacements are a reliable and safe method of treating established osteoarthritis. As joint replacement technology improves we are seeing far more wear resistant bearing surfaces more suitable for use in younger people with hip osteoarthritis. Younger patients managed with artificial joint replacements however do have a much higher likelihood (over their whole lifespan) of requiring increasingly complex re-operations to revise failed artificial joint replacements. In selected patients with acetabular dysplasia, early corrective surgical intervention can slow or prevent the progression of joint damage and improve symptoms.
References [ + ]





{kind=link}