
Vulvar varicosities during pregnancy
Vulvar varicosities are varicose veins (dilated veins) at the vulva or outer surface of the female genitalia (in the labia majora and labia minora) 1). Vulvar varicosities occur most often during pregnancy. This is due to the increase in blood volume to the pelvic region during pregnancy and the associated decrease in how quickly your blood flows from your lower body to your heart. As a result, blood pools in the veins of your lower extremities as well as your vulvar region, causing vulvar varicosities. Vulvar varicosities can occur alone or along with varicose veins of the legs.
The anatomical basis for the development of vulvar varicosities relates to the connections between the veins of the pelvis and external genitals 2). Vulvar veins drain into the external and internal pudendal veins, which deliver blood to the great saphenous vein and internal iliac vein. The veins of the labia majora and labia minora anastomose with the uterovaginal plexus. In addition, the connection to the pelvic veins is provided via the obturator vein and superficial circumflex iliac vein, as well as the groin, clitoral, and perineal perforant veins.
It is estimated that between 4 percent and 22 percent of women and 22–34 percent of women with varicose veins of the pelvis will develop vulvar varicose veins during pregnancy, although the actual figure is most likely to be much higher with many women not developing any symptoms, or being too embarrassed to discuss the symptoms with their doctor 3). In some patients, vulvar varicosities may be associated with a chronic pelvic pain syndrome called pelvic congestion syndrome 4). Vulvar varicosities are rare during a first pregnancy and generally develop during month 5 of a second pregnancy and occurred most often in women with a history of two or more full-term pregnancies (91%). The risk increases with the number of pregnancies 5).
Vulvar varicosities don’t always cause signs and symptoms. If they occur, they might include a feeling of fullness or pressure in the vulvar area, vulvar swelling and discomfort. In extreme cases, the dilated vessels can bulge. They might look bluish and feel bumpy. Long periods of standing, exercise and sex can aggravate the condition.
During the postpartum period, perineal veins may persist and enlarge with time in 4%–8% of patients 6). Vulvar varicosities are associated with venous thromboembolic events, both during pregnancy and in the nonpregnant state, superficial dyspareunia (painful intercourse), and vulvar pain (vulvodynia) 7). Vulvar varicosities may also cause psychoemotional and family problems. It is difficult to estimate reliably the prevalence of this pathological condition, as vulvar varicosities often remain undiagnosed because of the atypical localization of the varicose veins, women’s reluctance to consult, and in some cases the absence of any discomfort.
In most cases, vulvar varicosities can be diagnosed at clinical examination, and do not require any special investigation methods. Their diagnosis requires an assessment of the state of the intrapelvic veins, and in cases of pregnancy further observation and examination in the postpartum period.
Vulvar varicosities treatment varies from purely conservative measures during pregnancy to various surgical procedures on the ovarian and vulvar veins. A diagnostic and treatment algorithm for vulvar varicosities in various clinical situations is presented in Figure 4. An individualized approach to diagnostic methods and treatment for this disorder can significantly improve the quality of care of patients with chronic venous diseases.
To feel relief:
- Get a support garment. Look for one specifically designed for vulvar varicosities. Some designs also provide support for the lower abdomen and lower back.
- Change position. Avoid standing or sitting for long periods of time.
- Elevate your legs. This can help promote circulation.
- Apply cold compresses to your vulva. This might ease your discomfort.
Vulvar varicosities likely won’t affect your mode of delivery. These veins tend to have a low blood flow. As a result, even if bleeding occurred, it could easily be controlled.
Typically, vulvar varicosities related to pregnancy go away within about six weeks after delivery.
Figure 1. The vulva
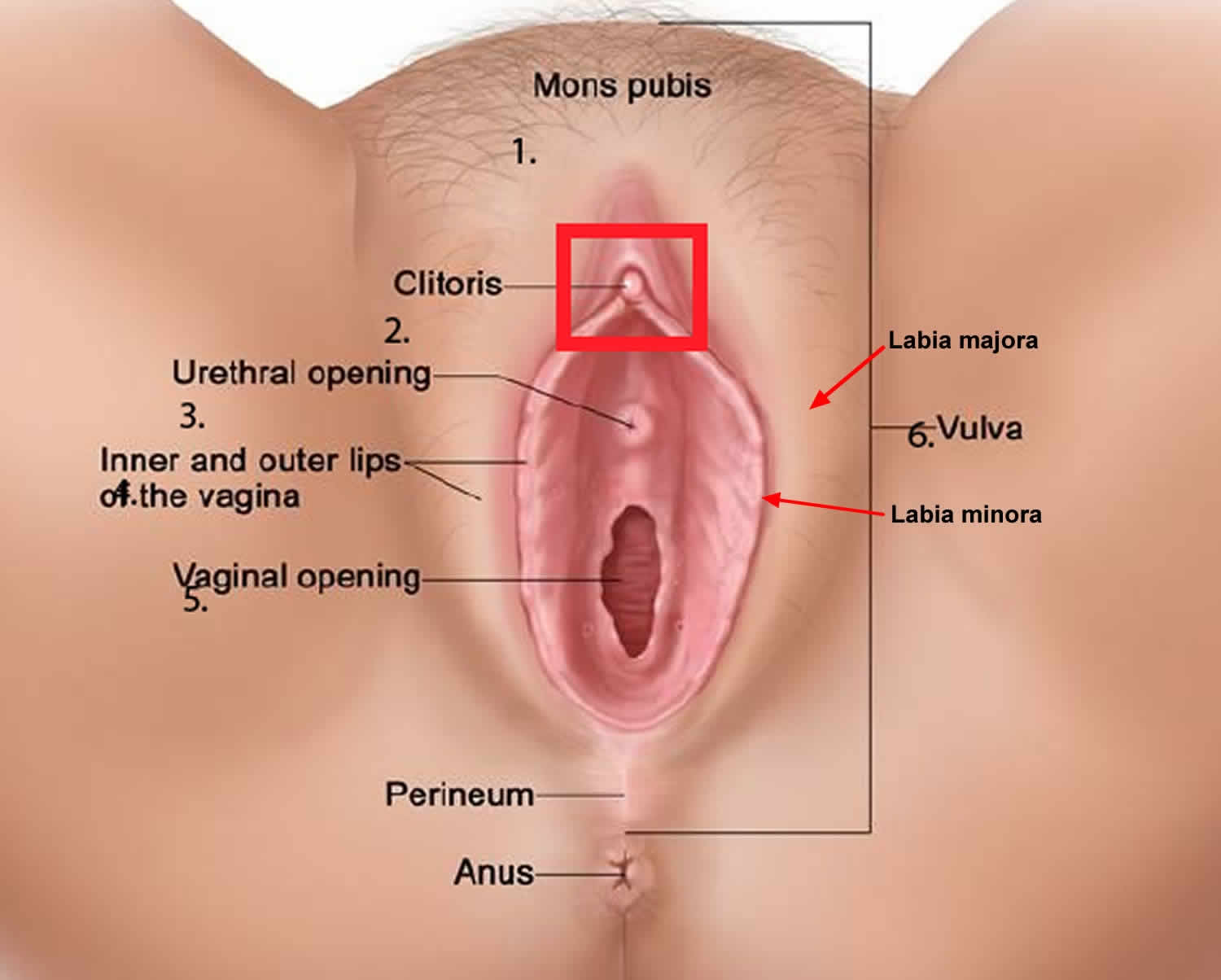
Figure 2. Vulvar varicose veins

Footnotes: A 33-year-old woman was admitted for induction of labor at 41 weeks 3 days of gestation. This was her third full-term pregnancy, and she had received regular antenatal care. Before induction, the physical examination revealed venous varicosities on the right labia majora and minora and the right vaginal wall (Panel A). Varicose veins in both legs were also noted. The patient reported that the varicosities had developed several months earlier and caused increasing discomfort and pruritus, but she had been embarrassed to mention them. She had had smaller varicosities during her previous pregnancies, with normal vaginal delivery. Vulvovaginal varicosities are common in pregnancy and usually appear in the second trimester. Possible mechanisms include compression of the inferior vena cava by the gravid uterus and hormonal changes. The presence of vulvar varicosities is not a contraindication for vaginal delivery, but clinical discretion regarding the route of delivery is required, depending on the size and location of the varicosities. In this instance, the patient underwent caesarean delivery without complications. The vulvar varicosities were substantially smaller after delivery (Panel B).
[Source 8) ]Figure 3. Thrombophlebitis of the vulvar veins. Hyperemia and edema in the area of thrombosed veins (arrow).

Figure 4. Vulvar varicosities diagnostic and treatment algorithm

Abbreviations: DUS = duplex ultrasound; VTE = venous thromboembolic event; UV = uterine vein; PV = parametrial vein; GV = gonadal (ovarian) vein; PVC = pelvic venous congestion; VAD = venoactive drug; MSCT = multislice computed tomography; SOPP = selective ovariography with pelvic phlebography; PhE = phlebectomy; ST = sclerotherapy; VCI = vena cava inferior; VCFI = vena cava-filter implantation; ACT = anticoagulant therapy.
[Source 9) ]Will the vulvar varicose veins rupture during childbirth?
It’s highly unlikely that damaged vein will rupture during childbirth. There have been a few cases of the varicose vein rupturing during pregnancy, however following the above tips, and seeking professional advice, will help prevent this from happening.
The good news is for most women is the varicose veins will resolve on their own after several months post-partum. In some cases, it can take up to a year. For a small percentage of women, however, varicose veins will not shrink or disappear after pregnancy and may require medical treatment.
Varicose veins and swelling in your legs, ankles and feet
If you look down and can’t see your ankles, you’re not alone. Many women have swelling in their legs, ankles and feet during pregnancy. Swelling may be caused by pregnancy hormones, having more fluid in your body during pregnancy, and pressure from your growing baby on the veins that carry blood to your heart.
Pressure on a vein called the inferior vena cava may cause sore, itchy, blue bulges on your legs. These are called varicose veins. They usually don’t cause problems, but they’re not pretty. You’re more likely to have them if it’s your first pregnancy or if other people in your family have them.
Here’s what you can do to help relieve varicose veins and swelling in your legs, ankles and feet:
- Don’t stand for long periods of time.
- When you’re sitting down, put your feet up. Don’t cross your legs when you sit.
- When you’re lying down, put your legs up on a pillow.
- Sleep on your left side. This takes pressure off the vein that returns blood from the lower parts of your body to your heart.
- Wear support hose or compression stockings or leggings. These fit tight all over and can help control swelling. Don’t wear socks or stockings that have a tight band of elastic around the leg.
- Do something active every day. Talk to your provider about activities that are safe during pregnancy.
- Put an ice pack on swollen areas.
If you have extreme or sudden swelling, call your doctor right away. These may be signs of a serious condition called preeclampsia. This condition can happen after the 20th week of pregnancy. It’s when a woman has high blood pressure and signs like a severe headache that mean that some of her organs aren’t working properly.
Vulvar varicosities causes
Varicose veins can develop in your vulva during pregnancy due to normal changes that occur to your body at this time, such as:
- increased blood volume
- hormonal softening of the walls of your veins
- increasing pressure on the large veins in the abdomen and pelvis as your baby grows.
Vulvar varicosities symptoms
Not all women with vulvar varicosities will be able to see them and most often they are asymptomatic. Some women will have visible veins around the vulva or inner thigh. Yet others will not show any visible signs but they will experience pain.
If you don’t have any physical side-effects, here are a few symptoms you can look out for:
- Pain around the pelvis or lower back, usually described as a dull ache.
- A feeling of heaviness or fullness of the vulva.
- Any pain in the vulva that gets worse after standing, sexual activity, or physical activity.
- Swelling or itchiness around the vulva.
- An increase in urination.
In rare cases, they cause anxiety, pain, and manifest as heaviness, discomfort during walking, painful intercourse (dyspareunia) and pruritus (itch).
Vulvar varicosities complicationa
Complications such as thrombosis or bleeding are rare. A superficial thrombosis presents as a painful, red (inflammatory) swelling, and is firm to the touch. It requires examination to look for an underlying deep venous thrombosis. Spontaneous bleeding appears to be of academic interest, and in practice is not observed. Bleeding during childbirth is associated with vaginal tears or an episiotomy; internal bleeding results in formation of a hematoma, primarily affecting the labia. Vulvar varices are not an indication for a cesarean section delivery.
Vulvar varicosities diagnosis
Clinical examination of the patient standing and then supine reveals the following: soft, bluish dilatations, depressible by digital examination, with no painful point (sign of thrombosis). Often, this varicose network extends downwards to the medial aspect of the thigh, towards the long saphenous trunk, and sometimes posteriorly to the anal margin. The perfectly bilateral nature and the fact that they are associated with a varicose network in both lower limbs are reassuring.
The diagnostic test of pregnant women with vulvar varicosities is limited to duplex ultrasound of the veins of the perineum and lower extremities. This diagnostic test is required not only to verify the diagnosis but also to exclude latent thrombosis in the inferior vena cava in the presence of subjective symptoms. Dilation of the external pudendal vein and associated reflux, which represents an obvious reason for formation of vulvar varicosities, was found in 56% of patients.
Vulvar varicosities treatment
Vulvar varicosities treatment is symptomatic during pregnancy and curative afterward if the vulvar varicosities persist. The good news about vulvar varicose veins during pregnancy is that they are likely to disappear spontaneously within a few days of giving birth and rarely persist one month later.
Follow-up of 25 patients who developed vulvar varicosities during pregnancy for at least 1 year after childbirth revealed that dilated vulvar veins persisted in only 20% of patients 10). A reduction in vulvar varicosity was observed from the first days after birth, and most patients reported their complete disappearance within 2–8 months (5.8±1.04 months on average).
An association was found between the end of lactation period or a reduction in breastfeeding and the rate of vulvar varicosity disappearance: the shorter the lactation period, the earlier the varicose veins of the perineum disappeared, and vice versa. This once again indicates that hormonal changes play an important role in the development of varicose veins of the lower extremities, in the perineum, and in the small pelvis during pregnancy.
During pregnancy
Here are few safe ways you can treat the symptoms and prevent further damage to the varicose veins:
- Avoid standing still for any length of time—move, walk, change positions.
- Strictly avoid any squatting (kneel or sit on a stool). This is very important.
- Avoid constipation (this increases the strain pressure on your veins). Make sure your bowel motions are soft and easy to pass and sit in the emptying position using hand support under your perineum. Remember:
- maintain curve in lower back
- lean forward from the hips
- allow abdomen to relax forward
- always keep breathing
- no straining
- a small footstool may enhance position.
- Avoid any other activities that cause straining such as lifting, pushing, pulling, sneezing or coughing. When you cannot avoid any of these activities, use your hands or a rolled towel to help support your perineum.
- Lie down to rest–often. Sitting does not relieve the pressure on this area. Lying on your side is best.
- Ice fingers – cold compresses may give temporary relief. A trick some women use after giving birth is filling a rubber glove with cold water and ice. Using the glove as an ice-pack can help reduce swelling and relieve pain. Please note: ice should not be held on the area for longer than 30 minutes to 1 hour. Ice can reduce the blood flow needed for your body to heal.
- Practise your pelvic floor exercises regularly this will help blood to circulate better in the area and strengthen the supporting tissues around the veins.
- Supportive underwear – using support garments to assist in reducing the symptoms of vulval varicosities. Many women also find that full leg support stockings can some provide relief. You can also try supportive underwear (with a gusset) or bike pants with double sanitary pads inside. You will get the best results if you apply garments and support hosiery before getting out of bed in the morning (i.e. before gravity has taken effect).
- Pruritus (itch) is treated by bathing with a foaming solution without soap, and then a water-based zinc oxide paste. Pain and heaviness are treated with high-dose phlebotonic agents 11).
- Aromatherapy – some aromatherapists suggest using diluted geranium oil in a bath or soaked into a gauze pad as a direct compress to the area.
It should be remembered that pregnancy is a risk factor for venous thrombosis.
- Bleeding requires compression therapy.
- Sclerotherapy is always possible during pregnancy. It does not carry any particular risks either for the woman or the fetus. It is rarely performed because its beneficial results are uncertain in an unfavorable hormonal context.
After pregnancy
A month after delivery, vulvar varices most often have disappeared. Small, asymptomatic residual vulvar varicose veins are seen again after 1 year. Large or symptomatic varices are managed with curative therapy. Sclerotherapy is the preferred method because it is very effective on these thin-walled varices. It is administered most often in a very superficial varicose vein blister under visual control using a very fine gauge needle (30G) and a liquid sclerosing product. Sclerosing foamy products are more thrombogenic and are not indicated here. The dose used is 1 cc of 0.5% or 1% Aetoxisclerol; or 0.33% or 0.5%.Trombovar.
Varices in the groin or the mons veneris can be treated with echosclerosis. Care should be taken to avoid the external pudendal artery for which an accidental injection produces disastrous lesions in the vascular area downstream. Identification with the duplex color technique, by greatly increasing gains in the future area of injection, is essential to keeping in mind that “what is not seen exists” 12).
Phlebectomy remains possible for perineal varices 13), but is little performed because of the good results obtained with sclerotherapy. The same holds true for ligation of the labial or marginal perforating veins with the patient in the lithotomy position after identification by sonography.
References [ + ]





{kind=link}