Contents
- Vascular ring
- Vascular ring types
- Double aortic arch
- Right aortic arch with left ligamentum arteriosum
- Right aortic arch with retroesophageal left subclavian artery and left ligamentum arteriosum
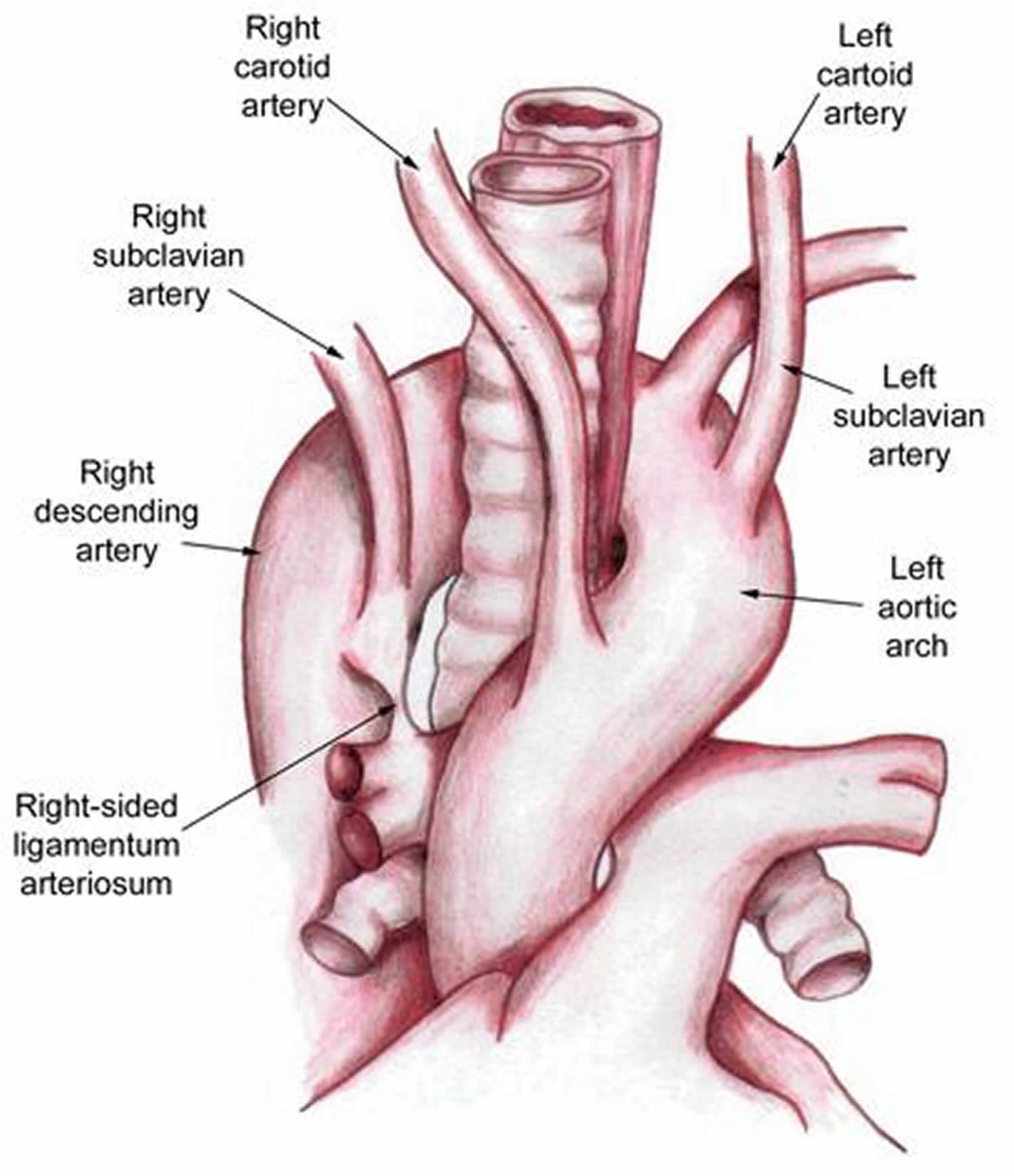
- Left aortic arch with right descending thoracic aorta and right ligamentum arteriosum
- Left aortic arch with right descending aorta and atretic right arch
- Anomalous innominate artery
- Retroesophageal right subclavian artery with left aortic arch and left ligamentum arteriosum
- Anomalous left pulmonary artery (pulmonary artery sling)
- Vascular ring causes
- Vascular ring signs and symptoms
- Vascular ring diagnosis
- Vascular ring treatment
- Vascular ring prognosis
- Vascular ring types
Vascular ring
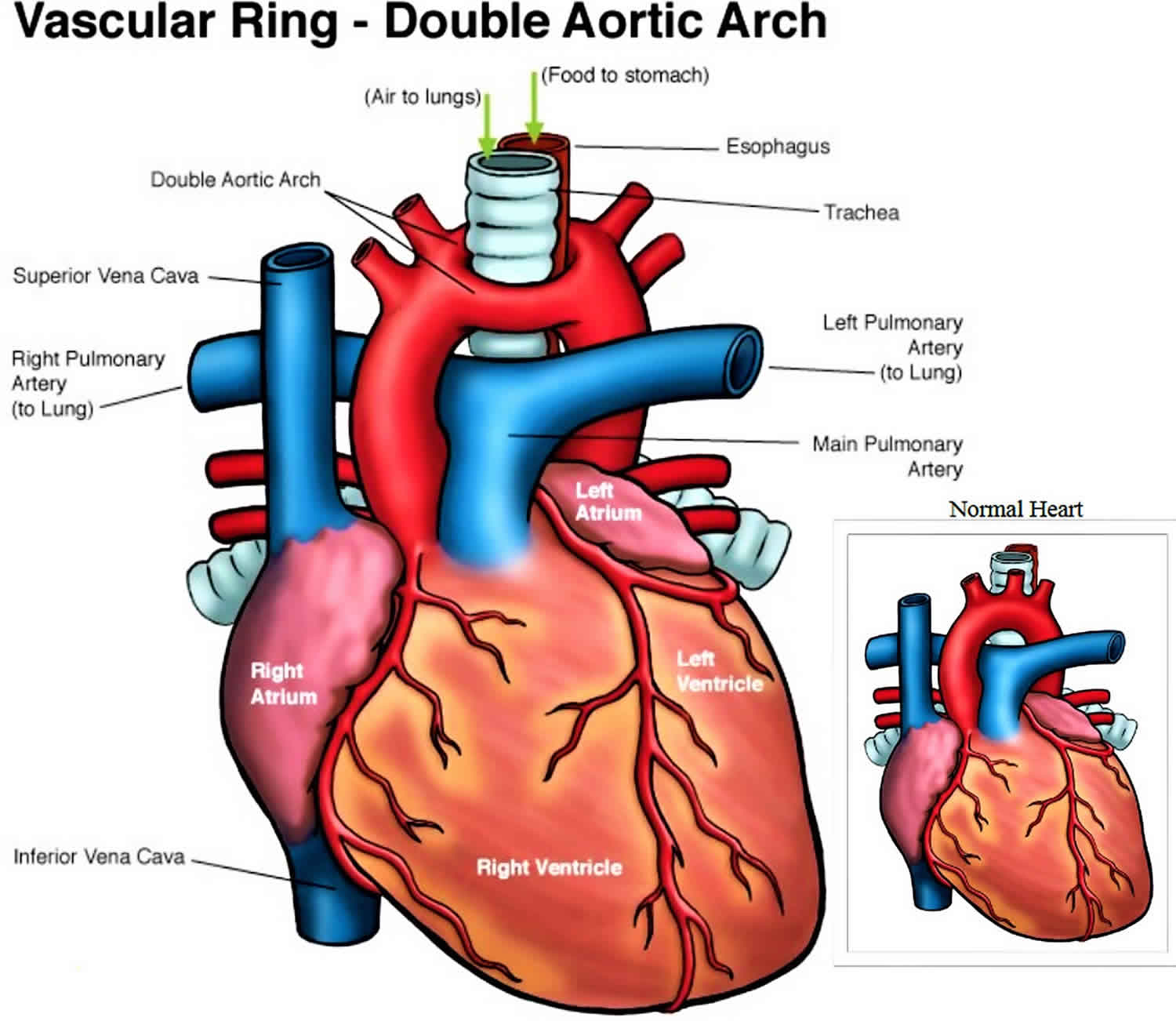
A vascular ring occurs when the aorta (the large artery that carries oxygenated blood out of the heart) or its branches form a complete ring around the trachea (the tube that carries air to the lungs) and the esophagus (the tube that carries food to the stomach) 1). This happens when certain parts of the aorta that normally disappear during fetal development persist abnormally. The aorta starts normally at the heart as one large vessel, but then divides into two arches: one on each side of the trachea and esophagus. The two arches then come back together into one vessel (the descending aorta).
“Vascular” means relating to blood vessels (veins and arteries). The condition is called “vascular ring” because the aorta or other, related arteries — encircles the trachea and esophagus.
Normally, the aorta starts at the left ventricle of the heart as one large vessel: it arches up (the aortic arch) to the left of the trachea and then down (the descending aorta). Arteries that deliver blood to the head, arms and other parts of the upper body branch off at the top of the arch. Arteries that deliver blood to the abdomen, legs and other parts of the lower body branch off from the descending aorta.
As their name suggests, vascular rings are caused by malformed blood vessels. But the vessels themselves aren’t really the issue, and some people without symptoms may live their entire lives not even realizing that they have a vascular ring. Instead, symptoms occur when a vascular ring puts pressure on a child’s esophagus, trachea, or both.
Vascular ring types
There are different types of vascular rings. The most common are:
Double aortic arch
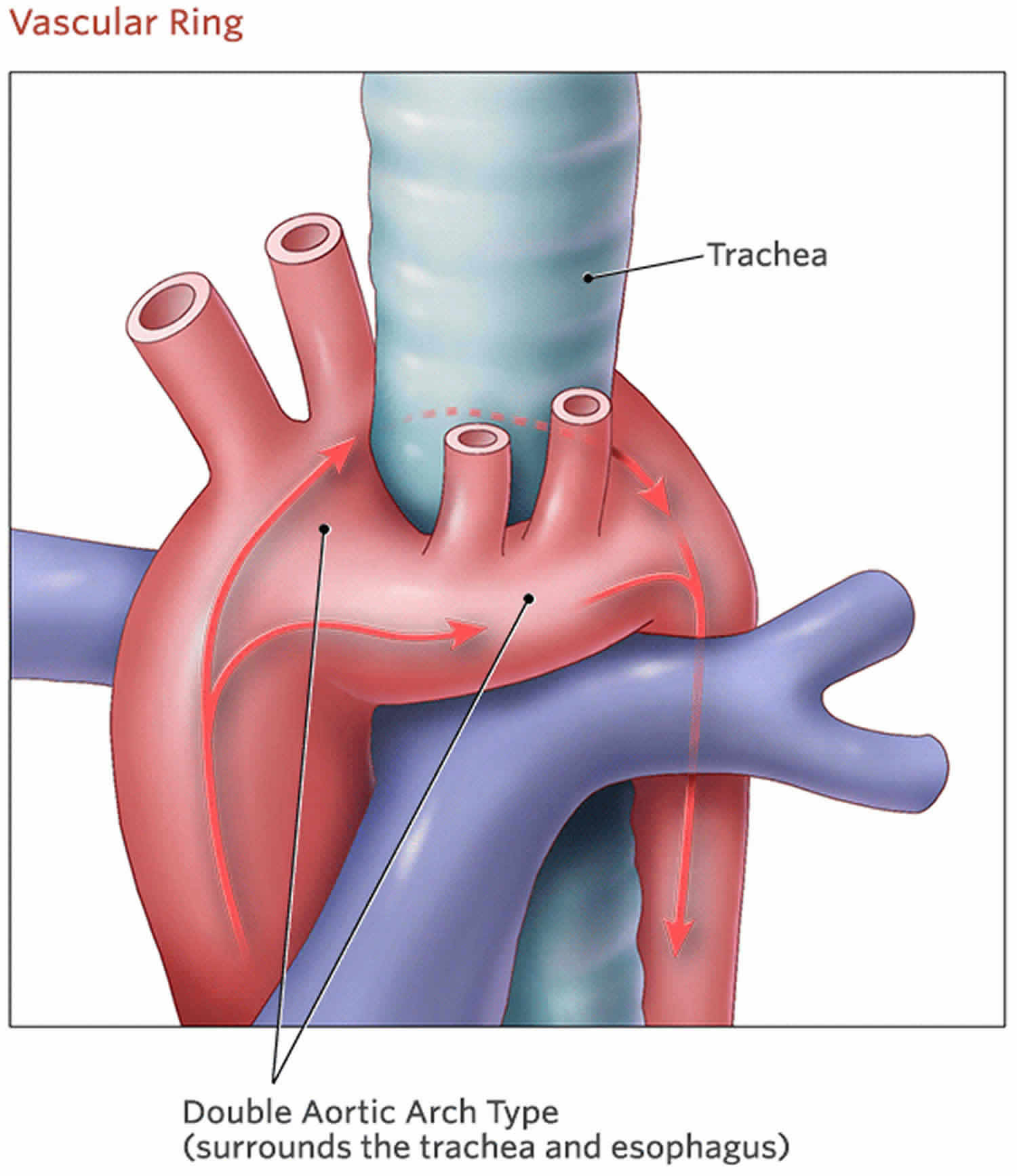
Double aortic arch is a congenital (present at birth) abnormal formation of the aorta, where both the left and right aortic arches are present, resulting in a complete circle around the trachea and esophagus 2). Double aortic arch is the most common cause of tracheoesophageal compression, with an incidence of 46% to 76% in reports of vascular rings 3).
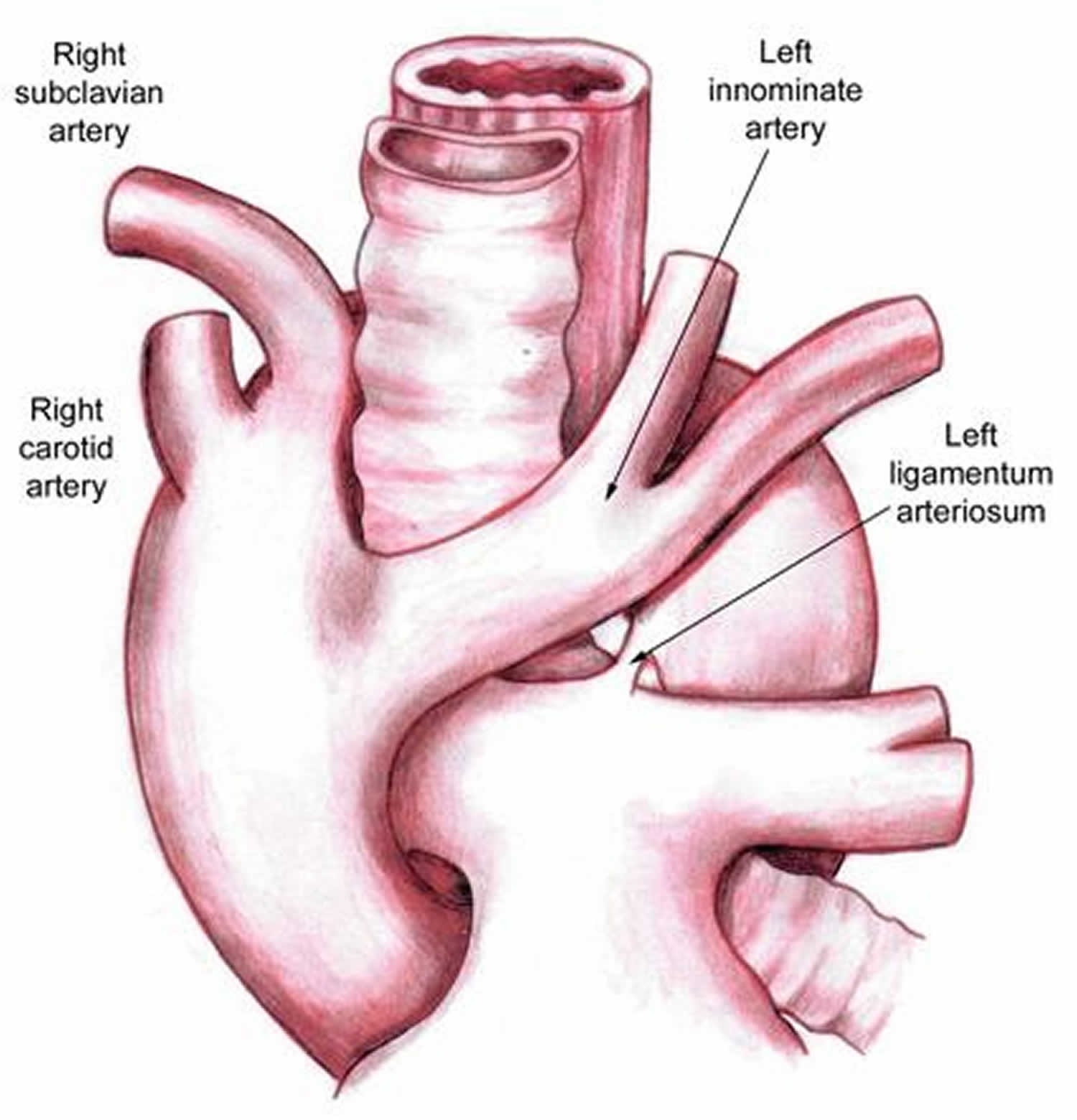
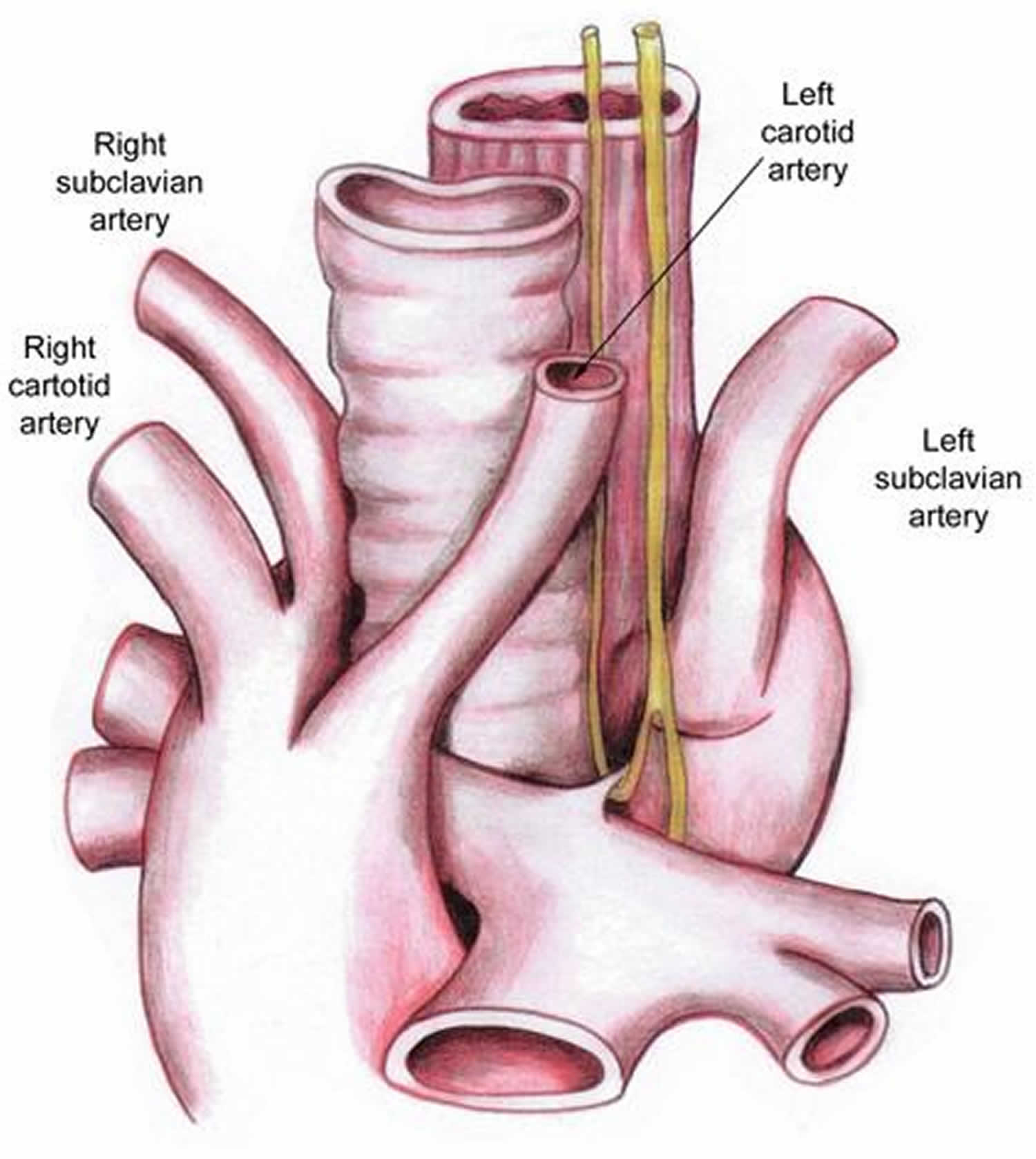
The fetal heart starts with two symmetrical branches of the aorta. Parts of the aortic arch regress in the second month of fetal life, usually resulting in a left aortic arch with three artery branches: the innominate artery, the left common carotid artery, and the left subclavian artery. The ductus arteriosus is present from the left pulmonary artery to the aorta, near the left subclavian origin. Double aortic arch occurs when there is abnormal regression of parts of the original two aortic arch branches. A left and a right aortic arch are present, resulting in a complete circle around the trachea and esophagus. The right aortic arch is usually larger than the left aortic arch. The right arch gives rise to the right common carotid artery and right subclavian artery and the left arch gives rise to the left common carotid artery and left subclavian artery.
Generally, incidence of double aortic arch and vascular rings is unknown, although vascular rings comprise an estimated 1% of cardiovascular malformations that are managed surgically. In most surgical series, 45-65% of patients undergoing repair of a vascular ring have a double aortic arch 4).
Figure 1. Double aortic arch
Right aortic arch with left ligamentum arteriosum
The aorta starts off to the right, instead of the left (as is normal), and gives off an abnormal branch from the descending aorta. This abnormal branch passes behind the esophagus and gives off the vessel to the left arm (the left subclavian artery) and the ligamentum arteriosum. The ligamentum arteriosum is a remnant of a blood vessel that exists normally in the fetus; it runs between the aorta and the pulmonary artery, and in doing so completes the ring and also might constrict the trachea and/or esophagus.
The structure of the vascular ring and its relationship to the trachea and esophagus varies from child to child.
As viewed through a left thoracotomy, the descending thoracic aorta is visible and can be traced proximally to the area of its merger with the right aortic arch, which joins it from behind the esophagus. In this area, the ductus diverticulum and ligamentum arteriosum can be found.
Figure 2. Right aortic arch with left ligamentum arteriosum
Right aortic arch with retroesophageal left subclavian artery and left ligamentum arteriosum
The aortic arch travels to the right and behind the esophagus, joining the left-side descending aorta. As it takes this course, it gives off the left carotid artery first. Then, it sequentially gives off the right carotid, the right subclavian, and the left subclavian arteries. This last branch often has a retroesophageal position. The ligamentum arteriosum courses from the base of the left subclavian artery to the left pulmonary artery.
Through a left thoracotomy, the structures visible in normal position are the descending thoracic aorta and the distal portion of the left subclavian artery. These structures can be traced proximally to identify the site where the left subclavian artery exits the right arch as it joins with the descending aorta. The ligamentum arteriosum can be found at the base of the subclavian artery and traced towards the pulmonary artery.
Figure 3. Right aortic arch with aberrant left subclavian artery and left ligamentum arteriosum
Left aortic arch with right descending thoracic aorta and right ligamentum arteriosum
The arrangement of this anomaly is the mirror image of right aortic arch with retroesophageal left subclavian artery and left ligamentum arteriosum. Approached through a right thoracotomy, structures are identified and traced in the same manner.
Figure 4. Left aortic arch with right descending thoracic aorta and right ligamentum arteriosum
Left aortic arch with right descending aorta and atretic right arch
In a retroesophageal position, the left arch passes to the left of the trachea to join the right descending thoracic aorta. The surgical view is via a right thoracotomy. At the level of this junction and immediately superior to a right ligamentum arteriosum, an atretic right arch is found. The brachiocephalic vessels in this case exit the left arch in a normal sequence.
Anomalous innominate artery
The brachiocephalic vessels exit the left arch in the normal sequence. The innominate artery may be more distally positioned and leftward on the arch than normal.
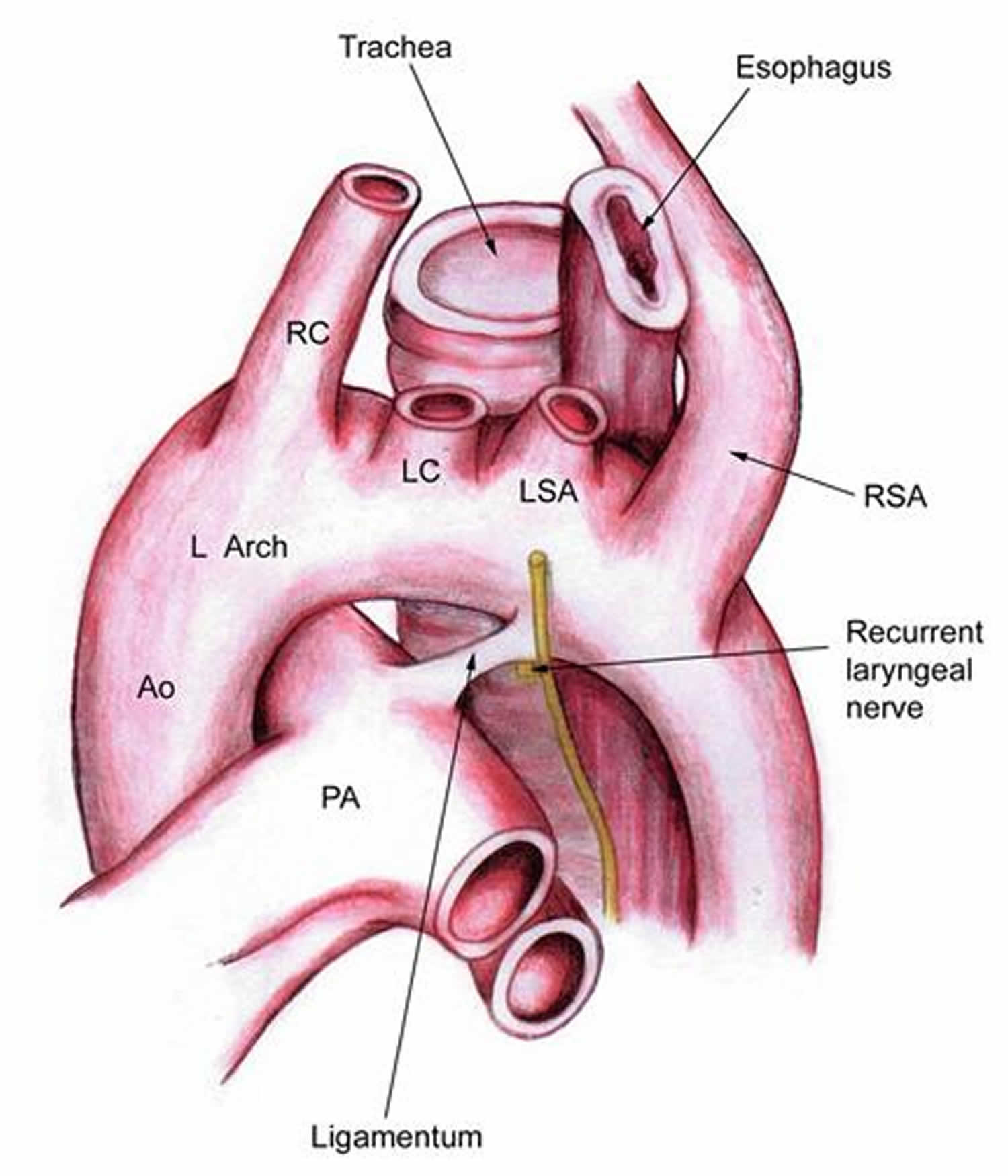
Retroesophageal right subclavian artery with left aortic arch and left ligamentum arteriosum
Rather than an innominate artery exiting the arch as the normal first brachiocephalic branch, the right carotid is the first brachiocephalic vessel. It is followed by the left carotid and then the left subclavian artery. The right subclavian artery is the last brachiocephalic branch to exit the arch, and it takes a course rightward and posterior to the esophagus. The ligamentum arteriosum is normally positioned on the left.
Figure 5. Retroesophageal right subclavian artery with left aortic arch and left ligamentum arteriosum
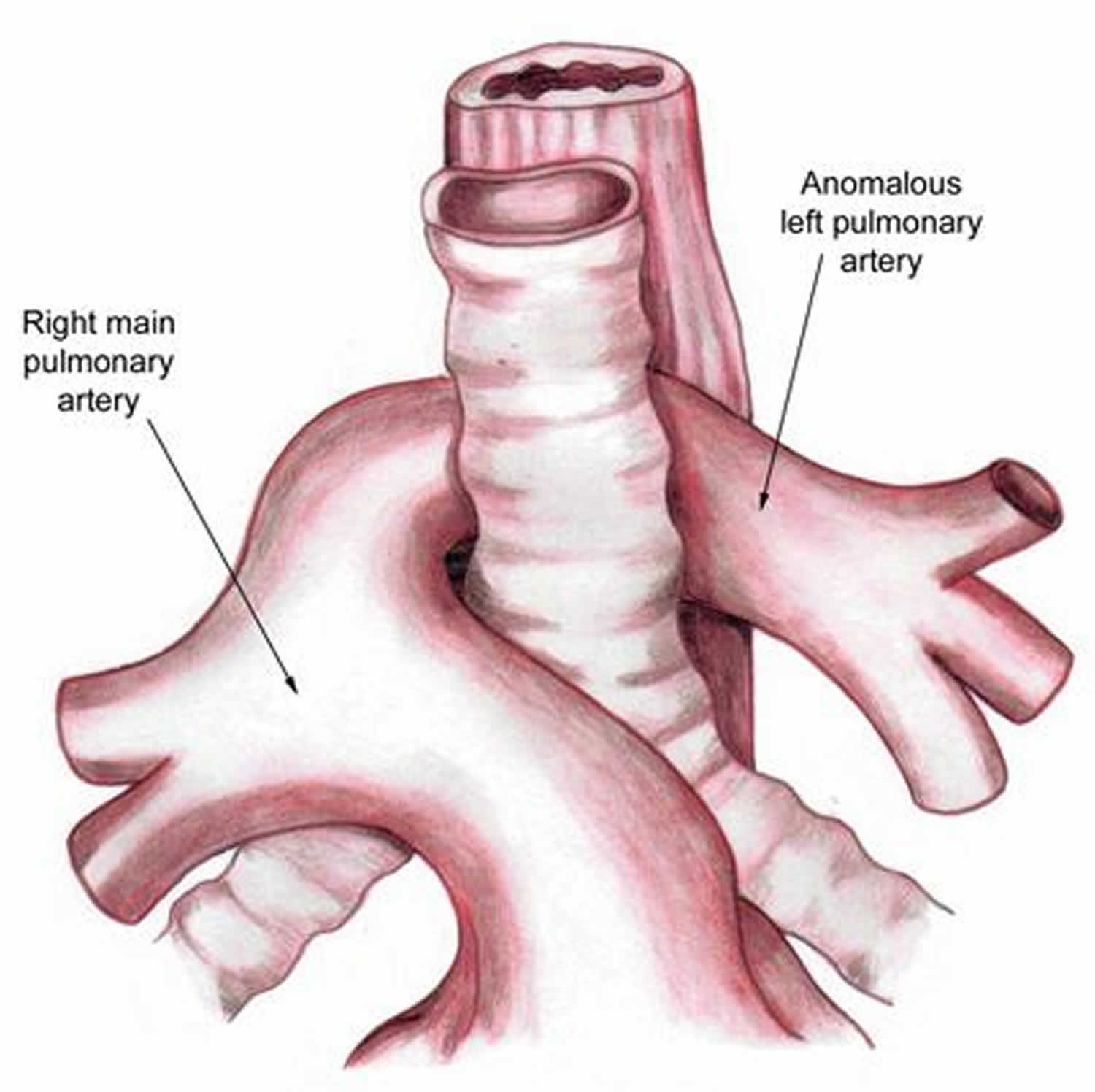
Anomalous left pulmonary artery (pulmonary artery sling)
Instead of the normal pulmonary artery configuration, in which the main pulmonary artery gives rise to the right and left pulmonary arteries, the main pulmonary artery continues behind the ascending aorta and rightward as the right pulmonary artery, which then gives off the left pulmonary artery. The left pulmonary artery passes from right to left between the trachea and esophagus in its course to the left lung. The ligamentum arteriosum takes a course from the junction of the main and right pulmonary arteries posteriorly to the aorta.
Figure 6. Pulmonary artery sling
Vascular ring causes
Normally, the aorta develops from one in a series of symmetrical arches (six embryonic branchial arches). By the end of the second month of fetal development, the other arches are naturally broken down or formed into arteries. When a vascular ring occurs, certain arches that should have disappeared still remain and form a ring structure. Several papers have reported the close association of band 22q11 deletion with anomalies of the aortic arch, as well as other congenital cardiac abnormalities 5).
In normal development, each primitive arch either progresses into a functional vascular structure or involutes as follows 6):
- The right and left first and second arches become a portion of the arterial supply to the face
- The third arches develop into the carotid arteries
- The dorsal aorta between the third and fourth arches involutes
- The fourth arches are the primary contributors to the aortic arch itself, with the proximal right fourth arch developing into the proximal right subclavian artery; the distal portion of the right fourth arch involutes at the point where it joins the dorsal arch; the left fourth arch remains as the aortic arch in normal development
- The fifth arches involute bilaterally
- The ventral right sixth arch becomes the proximal right pulmonary artery; the ventral portion of the left sixth arch develops into the left pulmonary artery, while the dorsal portion becomes the ductus arteriosus
- The entire left and the distal right subclavian arteries arise from the seventh segmental arterial branches of the dorsal aorta
Abnormal arch development results when one or more of the necessary involutions or other changes in embryonic arch structures does not occur.
Tracheal or tracheobronchial malacia and stenosis may develop in association with some of these lesions in the areas where the greatest degree of compression exists. This is particularly true in cases of anomalous left pulmonary artery.
Other congenital cardiac anomalies may be present in association with aortic arch anomalies.
The presence of a right aortic arch should always raise the suspicion of additional congenital cardiac disease. Right aortic arch has been reported in as many as 34% of cases of tetralogy of Fallot. Other intracardiac lesions found in association with a right aortic arch include double-outlet right ventricle, truncus arteriosus, ventricular septal defect with pulmonary atresia, transposition of the great vessels, tricuspid atresia, and absent left pulmonary artery.
Anomalous left pulmonary artery has also been associated with other cardiac defects in as many as 50% of cases. These include the aforementioned lesions, as well as persistent left superior vena cava, atrial septal defect, and ventricular defect. Complete tracheal rings (congenital absence of the membranous trachea) resulting in tracheal stenosis are another anomaly reported in as many as 50% of infants with anomalous left pulmonary artery. The combination of these two lesions is often termed the ring-sling complex.
Vascular ring signs and symptoms
In most cases, the symptoms of a vascular ring are mild. Some people without symptoms may live their entire lives not even realizing that they have a vascular ring. Instead, symptoms occur when a vascular ring puts pressure on a child’s esophagus, trachea, or both. That means the condition may go undiagnosed until your child is older, or even an adult. Symptoms range widely depending on the severity of the compression. If the condition is severe and your child has trouble breathing, a vascular ring may be diagnosed at several weeks or months of age.
The following symptoms may be present in children with vascular rings:
- Stridor (noisy breathing) or labored breathing, especially with eating
- Difficulty eating and swallowing: the child regurgitates milk or other food
- Difficulty feeding when you introduce solid foods
- Swallowing difficulties (dysphagia): the child feels like something is “stuck in the throat”; the child keeps choking or feels like he or she is choking on food
- Persistent cough or wheezing
- Acid reflux or gastroesophageal reflux (GERD)
- Respiratory distress
- Respiratory infections
Children with vascular rings often also have an airway disorder called tracheomalacia. In this condition, the trachea narrows or collapses when your child exhales, which makes it feel hard to breathe and may lead to a vibrating noise or cough. Like vascular rings, tracheomalacia can be present at birth, or it can develop in response to vascular rings or other anomalies.
Vascular ring diagnosis
If your child has any symptoms of a vascular ring — particularly noisy breathing or a weak pulse — their doctor may refer you for testing.
Diagnosis of a vascular ring may require some or all of these tests:
- Chest X-ray
- Cardiac MRI : a three-dimensional image that shows heart and vessel abnormalities
- Chest CT (CAT scan)
- Echocardiogram : sound waves create an image of the heart
- Bronchoscopy: a doctor looks at the trachea using an instrument called a bronchoscope (while patient is under anesthesia)
- Gastrointestinal tests such as barium swallow or barium esophagram. Barium (contrast) fluid is consumed by mouth and coats the esophagus. Fluoroscopy (x-ray) is done at the same time the barium is consumed, which reveals compression or obstruction of the esophagus
The gold standard for evaluating and identifying vascular rings is a computed tomography (CT) scan. This technique allows physicians to visualize your child’s vascular anatomy properly. Vascular rings can be diagnosed at any age, including while a child is still in the womb.
Vascular ring treatment
Children who with vascular rings but no symptoms usually don’t need surgical treatment. However, those who have symptoms from vascular rings typically require to surgery to relieve pressure on their airway and esophagus. Surgeons may use a variety of techniques to accomplish this, including:
- Complete resection of the diverticulum of Kommerell, which is typically left as an out-pouching of the aorta and compresses the esophagus and airway from the back
- Descending aortopexy, which moves the descending aorta to the side of the spine so it doesn’t compress the airway
- Rotation esophagoplasty, which moves the esophagus out of the airway so it doesn’t contribute to airway compression and can’t be compressed itself by the aorta and airway
- Posterior tracheobronchopexy, which keeps the airways open in children with vascular rings who also have tracheobronchomalacia below the narrow, compressed region of the airway. Occasionally, these children will also need anterior airway support to completely open the airways.
- Aortic uncrossing, which reroutes the aorta and can be combined with the airway procedure
Vascular surgeons repair vascular rings with a combination of these procedures in one comprehensive surgical procedure. In most cases, the surgeon makes an incision on the left side of the chest and goes between the ribs to access the area.
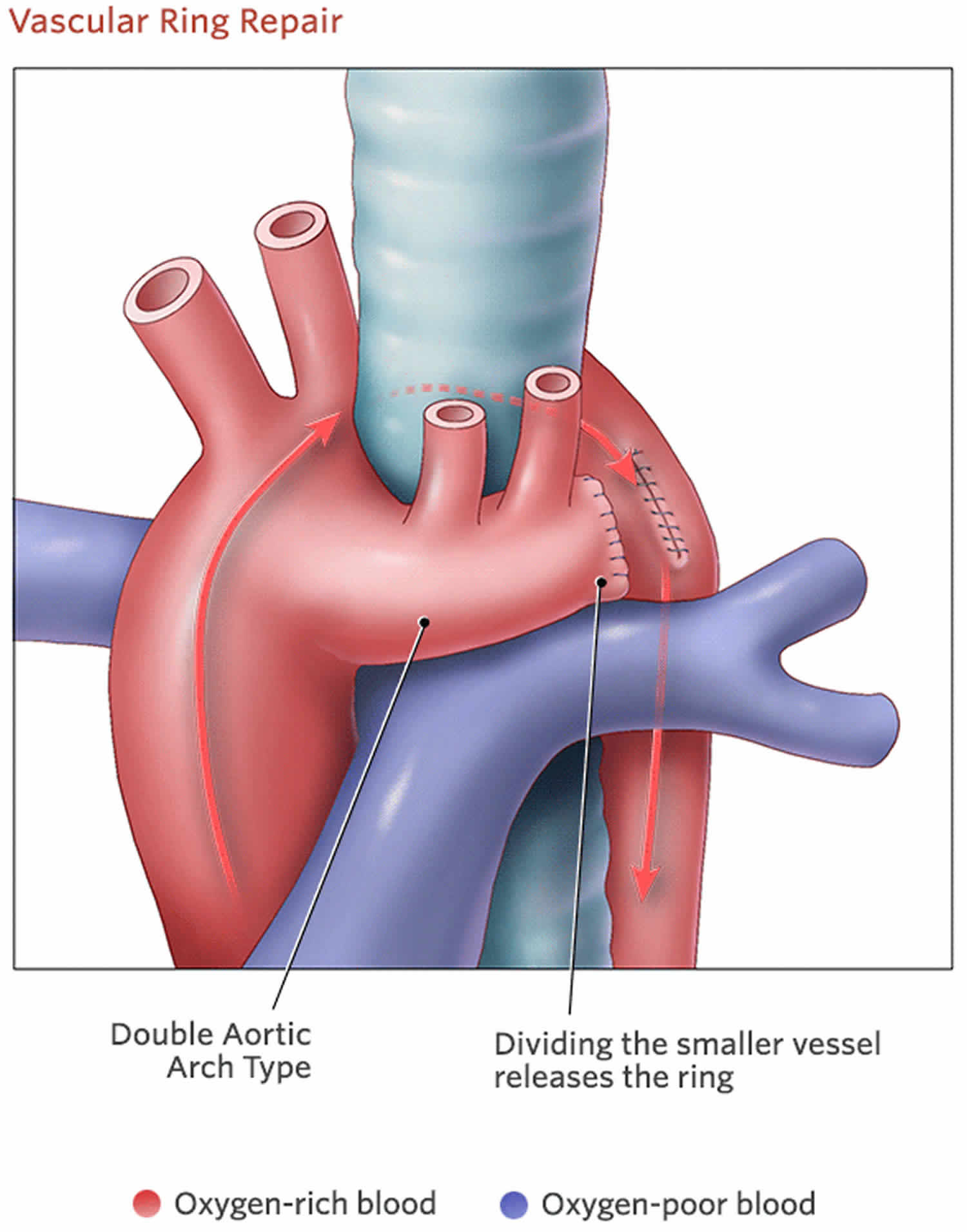
Double aortic arch surgery
Children with double aortic arch that are asymptomatic do not require surgical intervention. Timing of surgical intervention is determined by the severity of associated symptoms. Double aortic arch requires surgery (not open heart) if there are symptoms. In most cases, the surgeon makes an incision on the left side of the chest and goes between the ribs to access the area. The surgeon will cut and stitch closed one of the arches (usually the left) so the aorta no longer encircles or puts pressure on the trachea or esophagus. Children need careful respiratory management in the postoperative period. Normal life expectancy and development for children without other congenital anomalies.
The surgeon will cut and stitch closed one of the arches (usually the left) so the aorta no longer encircles or puts pressure on the trachea or esophagus.
Figure 7. Double aortic arch repair
Follow-up care
Through age 18
In most cases, children with double aortic arch recover completely after surgery and won’t need additional procedures. It is not uncommon for noisy breathing to continue for several weeks or months after surgery as the trachea slowly takes on a more normal shape. Rarely, symptoms such as coughing or labored breathing continue after surgery. Your child’s surgeon will monitor your child to make sure recovery is as complete and rapid as possible.
Pediatric cardiologists will follow your child until she is a young adult, coordinating care with her primary care physician. She will need to carefully follow doctors’ advice. In rare cases, pediatric cardiologists will suggest that your child limit certain types of exercise.
Into adulthood
Children born with double aortic arch who do not require surgery should follow up with a cardiologist.
Right aortic arch with left ligamentum arteriosum
The surgeon divides the ligamentum arteriosum so that it no longer constricts the trachea or esophagus. The right aortic arch remains, as a person can live with this irregularity.
In some cases, a child has no symptoms of vascular ring and the condition is discovered during an unrelated medical test, procedure or evaluation. In some of these cases, instead of surgery, a cardiac surgeon will monitor the child to make sure symptoms don’t appear and the condition isn’t harming the the child’s health.
The procedure to correct vascular ring is considered low-risk. In most cases, surgery is recommended.
Vascular ring prognosis
Because of enormous strides in medicine and technology, today most children with heart defects such as vascular rings will go on to lead productive lives as adults. About 95% of patients who undergo surgical correction of a vascular ring survive for long periods, and most of these are soon relieved of their symptoms. In those infants with no intracardiac or extracardiac defects, surgery for vascular rings carries essentially no mortality.
Among those with less optimal long-term results are patients with an anomalous left pulmonary artery with and without complete tracheal rings and those with severe associated congenital cardiac defects. In those patients with a severely deformed trachea or tracheomalacia, additional reconstruction procedures may be required in the future.
In a series reported by Backer et al, reoperation proved necessary for 26 of 300 patients who had undergone surgical intervention for vascular rings 7). The four primary indications for reoperation were Kommerell diverticulum (18 patients), circumflex aorta (two patients), residual scarring (two patients), and tracheobronchomalacia necessitating aortopexy (four patients).
A number of patients continue to show evidence of some pulmonary function abnormalities years after surgery. Several studies report that measured pulmonary function studies show some degree of airway obstruction in as many as 50% of patients 7-8 years postoperatively. Also, a large number of patients appear to have a pronounced bronchial responsiveness to histamine.
Naimo et al 8) reported long-term outcomes of complete vascular ring division in 132 children from a 36-year experience at a single institution (median follow-up, 11.4 years; range, 44 days to 36 years). In-hospital mortality was 1.5% (2/132), and no late deaths occurred. Overall survival was 98.3 ± 1.2% at 20 years. After surgical treatment, three patients experienced persistent tracheal compression and 16 had tracheomalacia. The freedom-from-reoperation rate was 88.6 ± 4.0%. None of the patients required tracheal surgery during the follow-up period.
François et al 9) assessed early and late outcomes (mean follow-up, 7.8 ± 5.8 years) in 62 patients (median age, 1 year) who underwent surgical treatment of a vascular ring (most commonly a double aortic arch [53%]). Median extubation time was 4 hours, and median hospital stay was 5 days. Early mortality was 8% and was associated with the anatomic diagnosis, concomitant anomalies, and the need for preoperative intubation. At 1 month, 63% of patients were free of residual symptoms; at 6 months, 82% were. At final follow-up, the rate of freedom from inhalation therapy was 82%.
References [ + ]





{kind=link}