
Contents
- Stillbirth
- Is stillbirth hereditary?
- What are the chances of a woman who has had one stillbirth to have another with her subsequent pregnancies?
- If you’ve had a stillbirth, can you have a healthy baby in another pregnancy?
- What if my baby is stillborn?
- How is a stillbirth baby delivered?
- Will parents get to spend time with their stillborn baby?
- Should an autopsy be performed on a stillborn baby?
- Should parents have a funeral service for a stillborn baby?
- Causes of stillbirth
- How do you know if your baby is stillborn?
- What are your options for giving birth if your baby is stillborn?
- What tests do you get after a stillbirth?
- Preventing stillbirth
- Coping with feelings of grief after a stillbirth
Stillbirth
Stillbirth is when a baby dies in the womb after 20 weeks of pregnancy. A miscarriage is usually defined as loss of a baby before the 20th week of pregnancy.
Stillbirth is further classified as either early, late, or term:
- An early stillbirth is a fetal death occurring between 20 and 27 completed weeks of pregnancy.
- A late stillbirth occurs between 28 and 36 completed pregnancy weeks.
- A term stillbirth occurs between 37 or more completed pregnancy weeks.
Most stillbirths happen before a woman goes into labor, but a small number happen during labor and birth. Stillbirth affects about 1 in 100 pregnancies each year in the United States; this is about 1 percent of all pregnancies and about 24,000 babies 1). That is about the same number of babies that die during the first year of life and it is more than 10 times as many deaths as the number that occur from Sudden Infant Death Syndrome (SIDS) 2).
Because of advances in medical technology over the last 30 years, prenatal care (medical care during pregnancy) has improved, which has dramatically reduced the number of late and term stillbirth 3). However, the rate of early stillbirth has remained about the same over time 4).
Stillbirths are due to natural causes. They can happen before delivery or during delivery. Causes include:
- Problems with the placenta, the organ that transports oxygen and nutrients to the fetus
- Genetic problems with the fetus
- Fetal infections
- Other physical problems in the fetus
In at least half of all cases, it is not possible to tell why the baby died. Stillbirth with an unknown cause is called “unexplained stillbirth.” Having an unexplained stillbirth is more likely to occur the further along a woman is in her pregnancy. Having an autopsy on the baby and other laboratory tests is important in trying to understand why the baby died before birth. Your health care provider can share more information about this.
Stillbirth occurs in families of all races, ethnicities, and income levels, and to women of all ages. However, stillbirth occurs more commonly among certain groups of people including women who:
- are of black race
- are 35 years of age or older
- are of low socioeconomic status
- smoke cigarettes during pregnancy
- have certain medical conditions, such as high blood pressure, diabetes and obesity
- have multiple pregnancies such as triplets or quadruplets
- have had a previous pregnancy loss
This does not mean that every individual of black race or older age is at higher risk for having a stillbirth. It simply means that overall as a group, more stillbirths occur among all mothers of black race or older age when compared to white mothers and mothers under 35 years of age. Differences in factors such as maternal health, income, access to quality health care, stress, social and emotional support resources and cultural factors may explain how these factors are related to having a stillbirth. More research is needed to determine the underlying cause of stillbirths in these populations.
These factors are also associated with other poor pregnancy outcomes, such as preterm birth.
If stillbirth happens before delivery, your health care provider may induce labor or perform a Cesarean section to deliver the fetus. In some cases, you can wait until you go into labor yourself. This usually happens within two weeks of stillbirth.
Counseling may help you cope with your grief. Later, if you do decide to try again, work closely with your health care provider to lower the risks. Many women who have a stillbirth go on to have healthy babies.
Stillbirth key points
- Some women are more likely than others to have a stillbirth. Reducing your risk factors for stillbirth may help you have a healthy baby.
- Scientists don’t know what causes all stillbirths. Common causes include infections, birth defects and pregnancy complications, like preeclampsia.
- You can have tests to try to find out what caused your baby’s death and prevent another stillbirth in your next pregnancy.
- Most women who have a stillbirth and get pregnant again later can have a healthy pregnancy and a healthy baby.
Is stillbirth hereditary?
There is no evidence to reflect that stillbirth is hereditary. However, because 1 in 150 babies are stillborn, women within the same extended family may experience a stillbirth. It is important to note that these related women’s stillbirths may have no connection whatsoever.
What are the chances of a woman who has had one stillbirth to have another with her subsequent pregnancies?
Although all pregnancies can be considered a possibility for stillbirth to occur, 98% of all pregnancies result in the live birth of a healthy baby.
If you’ve had a stillbirth, can you have a healthy baby in another pregnancy?
Yes. For most women, the chances of having another stillbirth are very low. Less than 1 in 100 women (less than 1 percent) who’ve had a stillbirth go on to have another stillbirth.
If you had a stillbirth and are thinking about having another baby, give yourself time to heal physically and emotionally. Your doctor may recommend that you have medical tests to try to find out more about what caused your stillbirth. You may need to wait until after you’ve had these tests to try to get pregnant again.
If you had a stillbirth that was caused by a genetic condition, a genetic counselor can help you understand the condition and the chances of you having another stillbirth. A genetic counselor is a person who is trained to help you understand about how genes, birth defects and other medical conditions run in families, and how they can affect your health and your baby’s health. Your health care provider can help you find a genetic counselor.
What if my baby is stillborn?
- Autopsies on all stillborn babies are important in order to help us understand and prevent as many deaths as possible. Autopsies can provide a cause of death in 40-70 percent of all stillbirth deaths.
- An examination of the placenta can also provide information about the possible cause of death. An autopsy and placental exam may provide answers to you about why your baby died.
- Knowing the cause of death can help you understand that there was nothing you could have done differently that would have prevented your baby’s death. Finding a cause of death is also important for parents who would like to have another baby.
How is a stillbirth baby delivered?
Most mothers that experience a stillbirth death will deliver their baby vaginally, but C-sections are not uncommon. The health and well being of the mother, such as pain control options and supportive family members and birth assistants can help ease the overwhelming emotional and physical pain of stillbirth.
Will parents get to spend time with their stillborn baby?
It is encouraged that the parents and other family members spend some personal time together to hold the baby and say hello before saying goodbye. Many photographers offer their services to take photos that can be treasured in the years to come. Make decisions on what is best for you and any cultural beliefs you may have.
Should an autopsy be performed on a stillborn baby?
Medically speaking, autopsies on all stillborn babies are critical in order to obtain more definitive and comprehensive answers – and ultimately prevent as many stillbirth deaths as possible. Finding a cause of death through autopsy is also important for those parents that may consider another pregnancy.
Should parents have a funeral service for a stillborn baby?
Most states require that parents take responsibility for their child’s remains, whether that be by burial or by cremation. Having a funeral or memorial service for a stillborn baby helps many families say goodbye and brings closure that will help with the healing process.
Causes of stillbirth
Stillbirth can happen in any family. Scientists don’t always know why stillbirth affects certain women more than others. Stillbirth with an unknown cause is called “unexplained stillbirth.” Having an unexplained stillbirth is more likely to occur the further along a woman is in her pregnancy. Having an autopsy on the baby and other laboratory tests is important in trying to understand why the baby died before birth. Your health care provider can share more information about this.
Stillbirth can be caused by problems with the mother, baby, placenta or umbilical cord.
In stillbirths where a cause was identified by an autopsy, some common causes include:
Infections in the mother or baby. Some infections may not cause signs or symptoms and may not be diagnosed until they cause serious complications, like premature birth or stillbirth. Infections that can cause stillbirth include:
- Cytomegalovirus (CMV). This is a kind of herpes virus that you can get by coming in contact with body fluid (like saliva, semen, mucus, urine or blood) from a person who carries the virus. It’s a common infection in young children, but if you get it during pregnancy, it can cause serious problems, like stillbirth.
- Fifth disease also called erythema infectiosum. This is a common childhood illness that’s caused by a virus called parvovirus B19. It usually spreads through the air from an infected person’s cough or sneeze.
- Genital and urinary tract infections. These infections affect the urinary tract and genitals (sex organs), like the vagina or ovaries. The urinary tract is the system of organs (like the kidneys and bladder) that helps your body get rid of waste and extra fluids. Getting infected with genital herpes for the first time during pregnancy can lead to stillbirth. Genital herpes is a sexually transmitted infection (also called STI) you can get from having sex with someone who’s infected.
- Listeriosis. This is a type of food poisoning.
- Syphilis. This is an sexually transmitted infection (STI).
- Toxoplasmosis. This is an infection you can get from eating undercooked meat or touching cat poop.
Problems with the placenta or umbilical cord. Placental problems include infections, blood clots, inflammation (redness, pain and swelling), problems with blood vessels and other conditions, like placental abruption. Placental abruption is a serious condition in which the placenta separates from the wall of the uterus before birth. Placental problems cause about 24 in 100 stillbirths (24 percent). Problems with the umbilical cord include having a knot in the cord or the cord being pinched so that your baby doesn’t get enough oxygen. Problems with the umbilical cord may lead to about 10 in 100 stillbirths (10 percent).
Complications during pregnancy, including:
- Being pregnant longer than 42 weeks
- Diabetes, obesity, high blood pressure and preeclampsia
- Health conditions like lupus, thrombophilias and thyroid disorders. Lupus is an autoimmune disorder. Autoimmune disorders are health conditions that happen when antibodies (cells in the body that fight off infections) attack healthy tissue just about anywhere in the body by mistake. Thyroid disorders affect your thyroid, a gland in your neck that makes hormones that help your body store and use energy from food. Thrombophilias increase your chances of making abnormal blood clots.
- Preterm labor and preterm premature rupture of the membranes also called PPROM. Preterm labor is labor that begins early, before 37 weeks of pregnancy. PPROM is when the sac around the baby breaks early, causing labor to start.
- Fetomaternal hemorrhage. This is when your baby’s blood mixes with your blood during pregnancy or birth.
- Trauma or injuries (like from a car accident)
Conditions in the baby, including:
- Birth defects and genetic conditions. About 14 in 100 stillborn babies (14 percent) have one or more birth defects, including genetic conditions like Down syndrome.
- Fetal growth restriction
- Not getting enough oxygen during labor and birth
- Rh disease. Rh factor is a protein on the surface of red blood cells. Rh disease happens when a woman who doesn’t have the protein (called Rh-negative) is pregnant with a baby who does have the protein (called Rh-positive). Rh disease can be prevented.
Risk factors for stillbirth
Researchers are working to learn more about risk factors for stillbirth. Risk factors are things that make you at risk for (more likely than others to have) a condition. Having a risk factor for stillbirth doesn’t mean for sure that you will have stillbirth. But knowing about and reducing your risk factors may help prevent stillbirth from happening to your baby. Some risk factors are things you can’t change, such as having a stillbirth in a previous pregnancy. Other risk factors are things you can do something about, like quitting smoking. Talk to your health care provider about what you can do to help reduce your risk factors for stillbirth.
According to the Centers for Disease Control and Prevention (CDC) and other experts, risk factors for stillbirth include:
Medical conditions
- Being obese. If you’re obese, you have an excess amount of body fat and your body mass index also called BMI, is 30 or higher. BMI is a measure of body fat based on your height and weight.
- Diabetes. Diabetes is a condition in which your body has too much sugar (called glucose) in the blood.
- High blood pressure. Blood pressure is the force of blood that pushes against the walls of your arteries. Arteries are blood vessels that carry blood away from your heart to other parts of the body.
Pregnancy conditions and pregnancy history
- You’re pregnant with multiples (twins, triplets or more).
- You have intrahepatic cholestasis of pregnancy. This is the most common liver condition that happens during pregnancy.
- You had complications in a previous pregnancy, like premature birth, preeclampsia or fetal growth restriction. Premature birth is birth that happens too early, before 37 weeks of pregnancy. Preeclampsia is a condition that can happen after the 20th week of pregnancy or right after pregnancy. It’s when a pregnant woman has high blood pressure and signs that some of her organs, like her kidneys and liver, may not be working properly. Fetal growth restriction is when a baby doesn’t gain enough weight in the womb before birth.
- You’ve never given birth before.
- You had a miscarriage or stillbirth in a previous pregnancy. Miscarriage is when a baby dies in the womb before 20 weeks of pregnancy.
Age, race and social factors
- You’re younger than 20 or older than 35.
- You’re black. Black women have a higher risk for stillbirth compared to other women. African American mothers (2-3 times greater risk). African American mothers over 35 years of age (4-5 times greater risk). Scientists don’t know why stillbirth affects black women more than other women, but researchers are working to learn more about it.
- You smoke, drink alcohol or use street drugs or prescription painkillers, like opioids.
- You’re not married.
Other possible risk factor
A recent study says that being exposed to certain kinds of air pollution (mainly ozone) may increase your risk for stillbirth. Ozone is a gas that comes from car exhaust, gasoline and fumes from factories and chemicals. More research is needed to find out how ozone and other air pollution affects pregnancy and stillbirth. If you’re worried about air pollution and your pregnancy, talk to your healthcare provider.
How do you know if your baby is stillborn?
Signs of a condition are things someone else can see or know about you, like you have a rash or you’re coughing. Symptoms are things you feel yourself that others can’t see, like having a sore throat or feeling dizzy.
The most common symptom of stillbirth is when you stop feeling your baby moving and kicking. Others include cramps, pain or bleeding from the vagina. Call your health care provider right away or go to the emergency room if you have any of these conditions.
Your doctor uses ultrasound to see if your baby’s heart has stopped beating. An ultrasound uses sound waves and a computer screen to show a picture of your baby in the womb.
What are your options for giving birth if your baby is stillborn?
If your baby is stillborn, your doctor talks with you about options for giving birth. When and how you give birth depends on how far along you are in your pregnancy, your medical condition and what you think is best for you and your family. Some women need to give birth right away for medical reasons, but it’s often safe to wait until you go into labor on your own. Labor usually starts within 2 weeks after a baby dies in the womb.
Your doctor may recommend:
- Inducing labor. This is when your provider gives you medicine or breaks your water (amniotic sac) to make your labor start. Most women with a stillbirth have their providers induce labor soon after they learn of their baby’s death. If you decide to wait to go into labor on your own and it doesn’t happen by 2 weeks after your baby’s death, your provider may induce labor to help prevent dangerous blood clots from developing.
- Dilation and evacuation (also called D&E). During this surgical procedure, your provider dilates (opens) the cervix to remove tissue from the lining of the uterus. The cervix is the opening to the uterus (womb) that sits at the top of the vagina. Having a D&E may limit the information your provider can get about your baby’s condition. For example, if you have a D&E, your baby’s provider can’t do an autopsy on your baby.
- Cesarean birth also called C-section. This is surgery in which your doctor makes a cut in your belly and uterus to deliver your baby.
What tests do you get after a stillbirth?
Your doctor checks your baby, the placenta and the umbilical cord to try to find out why your baby died. The placenta grows in your uterus and supplies the baby with food and oxygen through the umbilical cord. Your doctor may ask to do certain tests to try find out what caused the stillbirth. Tests may include:
- Amniocentesis also called amnio. In this test, your provider takes some amniotic fluid from around your baby in the uterus. If your provider thinks a genetic condition or an infection in your baby may have caused the stillbirth, she may recommend an amnio before you give birth. Genetic conditions are health conditions that are passed from parents to children through genes.
- Autopsy. This is a physical exam of your baby’s body after death. During an autopsy, a provider checks your baby’s organs for signs of birth defects or other conditions. This may help your provider find out what caused your baby’s death and if you may be at risk of having another stillbirth in the future. Birth defects are health conditions that are present at birth. They change the shape or function of one or more parts of the body. Birth defects can cause problems in overall health, how the body develops or how the body works.
- Genetic tests to check for genetic conditions in your baby
- Tests for infections on your baby or on the placenta
In addition to checking your baby for medical and genetic conditions, your doctor reviews your family health history and any problems or illnesses you had during pregnancy. Your family health history is a record of any health conditions you, your partner and members of both your families have had. Your doctor may want to test you for infections, genetic conditions and other medical conditions, like lupus or thyroid problems.
Information from tests on you and your baby may help you if you’re thinking about getting pregnant again. Test results may help your doctor find out if there’s a chance that you could have another stillbirth. Even if your doctor doesn’t find out what caused your stillbirth, having the tests may help you better understand and cope with your baby’s death. If you have questions about the tests, including their cost, talk to your health care provider.
Preventing stillbirth
At this time, there is no way to predict or prevent all stillbirths. But there are many things that pregnant mothers can do to reduce the risk of stillbirth.
Here’s what you can do help to lower your risk of having a stillbirth in another pregnancy:
- Get a preconception checkup. Good prenatal care is important! This is a medical checkup you get before pregnancy. It helps make sure you’re healthy when you get pregnant. Start seeing a doctor as soon as you think you might be pregnant. Keep all appointments and follow your doctor’s advice.
- Get treatment for any medical conditions you have. If you have diabetes or high blood pressure, work closely with your doctor to keep it under control.
- Get to a healthy weight before getting pregnant. Your provider can recommend ways to get to a weight that’s right for you.
- Don’t smoke, drink alcohol, use marijuana or other drugs that can be harmful to your pregnancy. Tell your doctor if you need help to quit.
- If you have any pain or bleeding from the vagina during pregnancy, see your doctor right away.
- During your last trimester, perform a ‘kick count” at the same time every day when your baby is most active. Kick counting is a great way for you and your partner to bond with your baby. By performing a kick count at the same time every day during your last trimester, you can also help your doctor monitor your baby’s health. Doctors recommend that parents start counting and keeping track of their baby’s kicks beginning with the 28th week of pregnancy (earlier for high-risk pregnancies.) By doing kick counting daily, you will get to know your baby’s normal movement pattern within a week or two. By using a kick count chart, you and your doctor will be able to tell if there are any changes in your baby’s normal pattern. Studies show that a major decrease in your baby’s normal amount of movement could be a signal that there’s a problem.
- If you are past your due date, talk with your doctor. Pregnancies longer than 42 weeks may be at greater risk for stillbirth.
- If you are concerned at anytime during your pregnancy, consider getting a second or third opinion.
If you get pregnant again, your doctor monitors you and your baby closely. At around 32 weeks of pregnancy, she may ask you to do kick counts to help you keep track of how often your baby moves. Your provider also may do medical tests to check your baby’s heart rate and movements.
Counting your baby’s kicks
Your baby moves many times a day. Your baby’s kicks are the best sign of his or her health. Thanks to ongoing research, kick counting is now being recognized as the first proactive strategy to help reduce your baby’s risk of stillbirth. Starting at week 28 (earlier for high-risk pregnancies) set aside time each day to count and keep track of your baby’s movements (kicks, twists, turns, swishes or rolls). This will help you know what the “normal” pattern for your baby is, so you can more easily notice any changes in the pattern of your baby’s movements. Experts agree that a change (increase or decrease) in your baby’s normal kicking pattern may be a signal that there is a problem.
- Pick a quiet time in your day when your baby is usually most active. If you think your baby is asleep, try pushing on your tummy or getting up and walking around for a few minutes to wake him. You can also try drinking something cold. Don’t start counting until you know your baby is awake.
- Sit with your feet up or lie on your side and start counting your baby’s movements until you reach 10 – it will take most moms less than 15 minutes to count kicks in this way.
- Count each of your baby’s movements as one kick. Kicks include twists, turns, swishes, rolls and jabs. Don’t count hiccups!
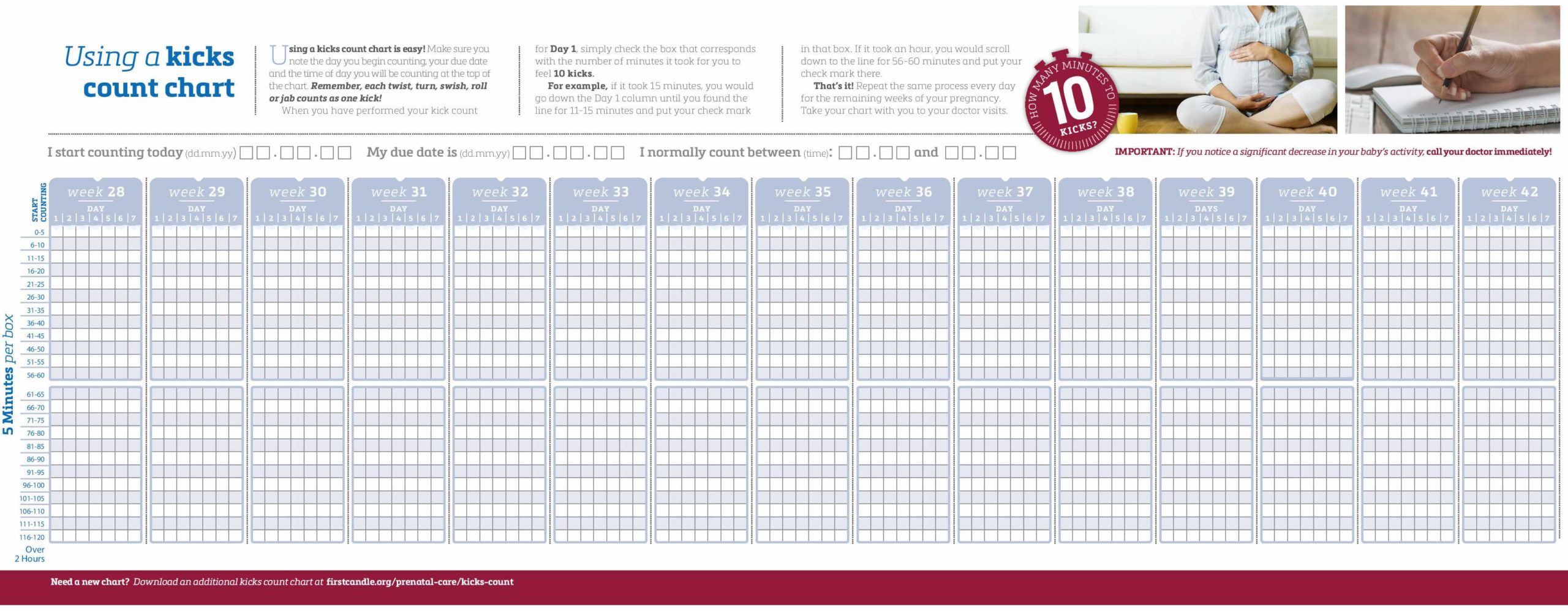
- Count until you reach 10 kicks and log the number of minutes it took on your kick count chart. It will take most moms less than 30 minutes to count 10 kicks, but could take up to two hours.
- Use a kick count chart to note the length of time it takes to feel 10 kicks.
- After a week or two, you will see that the kicking varies from day to day, but for the most part the days seem similar. This will continue to be the case for a healthy baby.
- If you notice a sudden change (increase or decrease) in your baby’s kicks, or you do not feel 10 kicks within two hours, call your doctor immediately.
- If you continue to be concerned do not hesitate to go to the emergency room or maternity ward or seek a second opinion.
Figure 1. Baby kick count chart
Coping with feelings of grief after a stillbirth
After the loss, you might be stunned or shocked. You might be asking, “Why me?” You might feel guilty that you did or didn’t do something to cause your pregnancy to end. You might feel cheated and angry. Or you might feel extremely sad as you come to terms with the baby that will never be. These emotions are all normal reactions to loss. With time, you will be able to accept the loss and move on. You will never forget your baby. But you will be able to put this chapter behind you and look forward to life ahead.
Grief is all the feelings you have when someone close to you dies. Having a stillborn baby is a painful loss for a family. But there are things you can do to help you grieve, heal and remember your baby.
After birth, do what feels right for you and your family. You may want to spend time alone with your baby and other family members. You can name your baby, hold your baby, bathe and clothe her and take part in cultural or religious traditions, like baptism. Some families take pictures of their baby, make footprints or save locks of hair. You may be able to keep things from the hospital, like blankets, that were used with your baby. Keepsakes like these can help you and your family remember your baby.
Parents who have a stillbirth need time to grieve. You and your partner may cope with grief in different ways, and you may need help dealing with others as you grieve.
After you leave the hospital, certain things, like hearing names you were thinking of for your baby, seeing the baby’s nursery at home or having your breast milk come in can be painful reminders of your loss. You may need help learning how to deal with these situations and the feelings they create. Ask your health care provider to help you find a grief counselor to help you cope with your baby’s death. Or your hospital may have a loss and grief program for families. Getting counseling can be really helpful to you and your family.
Talking about your feelings with other parents who have had a stillbirth may help you deal with your grief. Sharing your story may ease your pain and help you heal.
Having a stillbirth may make you at risk for postpartum depression. Postpartum depression is a kind of depression that some women get after having a baby. Tell your provider if you have signs or symptoms of postpartum depression, like feeling depressed most of the day every day, having little interest in things you normally like to do, or having trouble eating or sleeping.
To help get you through this difficult time, try some of these ideas:
- Turn to loved ones and friends for support. Share your feelings and ask for help when you need it.
- Talk to your partner about your loss. Keep in mind that men and women cope with loss in different ways.
- Take care of yourself. Eating healthy foods, keeping active, and getting enough sleep will help restore energy and well-being.
- Join a support group. A support group might help you to feel less alone.
- Do something in remembrance of your baby.
- Seek help from a grief counselor, especially if your grief doesn’t ease with time.
References [ + ]





{kind=link}