
Contents
Small for gestational age
Small for gestational age (SGA) means that a fetus or an infant is smaller or less developed than normal for the baby’s gender and gestational age. Small for gestational age generally describes any infant whose birth weight and/or birth length is less than the 10th percentile for babies of the same gestational age (that means the SGA baby’s weight and/or length falls below that of 90 percent of unborn babies of the same gestational age), adjusted for prematurity (gestational age) 1). This means that the baby is smaller than many other babies of the same gestational age. Many babies normally weigh more than 5 pounds, 13 ounces by the 37th week of pregnancy. Babies born weighing less than 5 pounds, 8 ounces are considered low birth weight. Gestational age is the age of a fetus or baby that starts on the first day of the mother’s last menstrual period. Severe SGA is defined as an estimated fetal weight or abdominal circumference less than the 3rd percentile 2).
Between 3% and 10% of live births each year are diagnosed as small for gestational age. In addition, when ultrasound evidence demonstrated poor fetal growth while in-utero, an infant may also be described as intrauterine growth restriction (IUGR), which means the fetus experienced intrauterine growth restriction.
SGA babies may appear physically and neurologically mature but are smaller than other babies of the same gestational age. SGA babies may be proportionately small (equally small all over) or they may be of normal length and size but have lower weight and body mass. Small for gestational age babies may be premature (born before 37 weeks of pregnancy), full term (37 to 41 weeks), or post term (after 42 weeks of pregnancy).
Although many SGA babies have low birthweight, they are not all premature and may not experience the problems of premature babies. Other SGA babies, especially those with IUGR, appear thin, pale, and with loose, dry skin. The umbilical cord is often thin, and dull-looking rather than shiny and fat.
The factors behind why an infant is born small for gestational age can be quite complex. The factors include fetal (such as genetic syndrome), maternal (such as substance use or infection), placental, and/or demographic (mother’s age, income level – these are both rare).
But setting aside these possible causes, 9 out of 10 infants born small for gestational age do experience catch-up growth by the age of 2 years, and usually by 6 months of age. Catch-up growth typically means that the child’s length curve moves upward, crossing the 3rd percentile line at a minimum and ideally getting closer to the percentile curve the child should be at based on his or her parents. It is the smaller subset of small for gestational age children, the 1 of 10 who fail to achieve catch-up growth by age 2, that are often referred to as “short small for gestational age” and who are our focus.
This group of short small for gestational age children typically include “idiopathic” small for gestational age children – children who remain small for unknown reasons…parents who are of normal height, there is a history of non-smoking/non-drinking, and lab tests have ruled out known causative factors. It can be frustrating to be the parent of such an small for gestational age child – you want answers to why your child isn’t growing. Here we hope to offer information on small for gestational age children and to answer some of the possible questions you may have.
Key points about small for gestational age babies
- Small for gestational age means a baby is smaller than expected for the number of weeks of pregnancy.
- Although some babies are small because their parents are small, most babies who are small for gestational age have growth problems that happen during pregnancy.
- When the unborn baby does not get enough oxygen or nutrients during pregnancy, he or she does not grow as much as normal.
- Small for gestational age is often suspected before birth.
- Prenatal care is important in all pregnancies. It is especially helpful to see any growth problems of the developing baby.
Figure 1. Small for gestational age chart
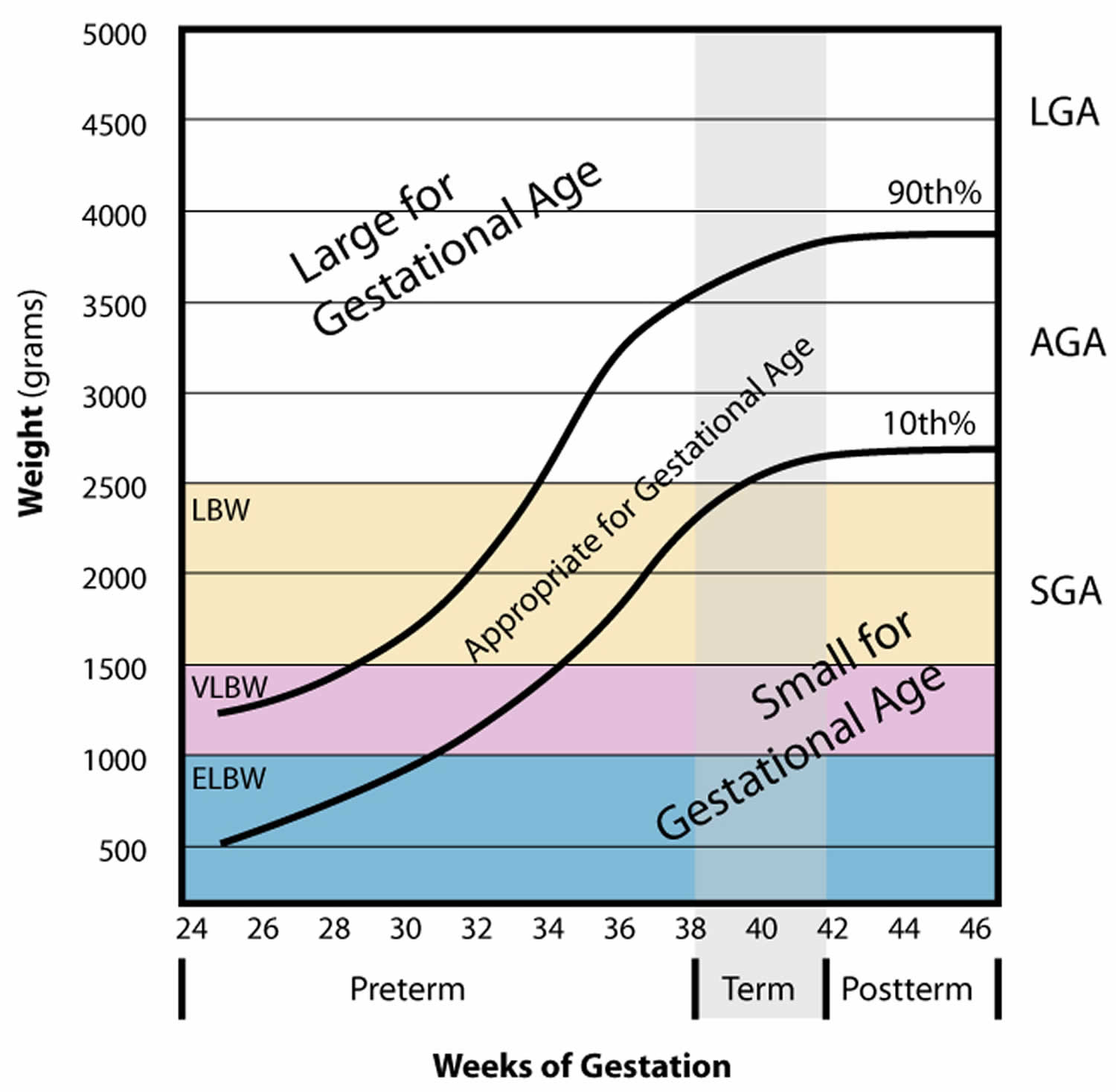
Footnote: Gestational age and birth weight of infants born at 24 to 46 weeks’ gestation. Infants are classified as large for gestational age (LGA), appropriate for gestational age (AGA), or small for gestational age (SGA). Another classification which takes in consideration only the weight and not the gestational age, is low body weight (LBW) = birth weight of less than 2500 g (5 lb 8 oz), very low birth weight (VLBW) = birth weight less than 1500 g and extremely low birth weight (ELBW) which is birth weight less than 1000 g.
Small for gestational age causes
Although some babies are small because of genetics (because their parents are small), most SGA babies are small because of fetal growth problems that occur during pregnancy. Many babies with SGA have a condition called intrauterine growth restriction (IUGR). IUGR occurs when the fetus does not receive the necessary nutrients and oxygen needed for proper growth and development of organs and tissues. IUGR can begin at any time in pregnancy. Early-onset IUGR is often due to chromosomal abnormalities, maternal disease, or severe problems with the placenta. Late-onset growth restriction (after 32 weeks) is usually related to other problems.
When the unborn baby doesn’t get enough oxygen or nutrients during pregnancy, the baby’s body and organs don’t grow as much as they should. Some of the problems that cause babies to be small for gestational age limit how much blood flows through the placenta. This can cause the baby to get less oxygen than normal. This increases the baby’s risks during pregnancy and delivery, and later. Things that can cause babies to be small for gestational age are listed below.
Some factors that may contribute to SGA and/or IUGR include the following:
- Maternal factors:
- High blood pressure
- Chronic kidney disease
- Advanced diabetes
- Heart or respiratory disease
- Malnutrition or anemia
- Infection
- Substance use (alcohol, drugs)
- Cigarette smoking
- Weighing less than 100 pounds
- Factors involving the uterus and placenta:
- Decreased blood flow in the uterus and placenta
- Placental abruption (placenta detaches from the uterus)
- Placenta previa (placenta attaches low in the uterus)
- Infection in the tissues around the fetus
- Factors related to the developing baby (fetus):
- Multiple gestation (for example, twins, triplets, and more)
- Infection
- Birth defects
- Inherited metabolic diseases
- Genetic diseases
- Chromosomal abnormality.
Small for gestational age prevention
Prenatal care is important in all pregnancies, and especially to identify problems with fetal growth. Stopping smoking and use of substances such as drugs and alcohol are essential to a healthy pregnancy and can reduce the risk for sudden infant death syndrome (SIDS) and other sleep-related infant deaths. Eating a healthy diet in pregnancy may also help.
Small for gestational age signs and symptoms
Small for gestational age babies may look mature, but they are smaller than other babies of the same gestational age. They may be small all over, or they may be of normal length and size but have lower weight and body mass. These babies may be born:
- Premature. Before 37 weeks of pregnancy.
- Full-term. Between 37 and 38 weeks (early term) through 41 weeks.
- Post-term. After 42 weeks of pregnancy.
Many small for gestational age babies have low birth weight. But not all are premature. They may not have the same problems as premature babies. Other babies, especially those with intrauterine growth restriction, may look thin and pale, and have loose, dry skin. The umbilical cord is often thin and dull-looking rather than shiny and fat.
The typical small for gestational age child is clearly thinner and shorter than his or her peers, but the range of other characteristics can vary. A list of possible characteristics can be found below:
Characteristics seen in almost all short SGA children:
- Low birth weight; probably low birth length
- Inadequate catch-up growth in first 2 years
- persistently low weight-for-height proportion
- Lack of muscle mass and/or poor muscle tone
Other common characteristics of short SGA children:
- Lack of interest in eating
- Fasting hypoglycemia & mild metabolic acidosis
- Generalized intestinal movement abnormalities:
- Esophageal reflux resulting in movement of food up from stomach into esophagus
- Delayed stomach emptying resulting in vomiting or frequent spitting up
- Slow movement of the small intestine &/or large intestine (constipation)
- Late closure of the anterior fontanel (soft spot)
- Frequent ear infections or chronic fluid in ears
- Congenital absence of the second premolars
- Delay of gross and fine motor development
- Delay of speech and oral motor development
- Kidney abnormalities
- Delayed bone age early, later fast advancement
- Early pubic hair and underarm odor (adrenarche) [associated with sudden bone age advancement]
- Early puberty or rarely true precocious puberty
- Classical or neurosecretory growth hormone deficiency
- ADHD and specific learning disabilities
- Blue sclera (bluish tinge in white of eye)
- Hypospadias (abnormal opening of the penis)
- Cryptorchidism (undescended testicles)
Small for gestational age complications
When the fetus does not receive enough oxygen or nutrients during pregnancy, overall body and organ growth is limited, and tissue and organ cells may not grow as large or as numerous. Some of the conditions that cause SGA and IUGR restrict blood flow through the placenta. This can cause the fetus to receive less oxygen than normal, increasing the risks for the baby during pregnancy, delivery, and afterwards.
Babies with SGA and/or intrauterine growth restriction (IUGR) may have problems at birth including the following:
- Decreased oxygen levels than normal
- Low Apgar scores (an assessment that helps identify babies with difficulty adapting after delivery)
- Meconium aspiration (inhalation of the first stools passed in utero) which can lead to difficulty breathing
- Hypoglycemia (low blood sugar)
- Low body temperature
- Difficulty maintaining normal body temperature
- Polycythemia (too many red blood cells)
Small for gestational age diagnosis
The baby with SGA is often identified before birth. During pregnancy, a baby’s size can be estimated in different ways. The height of the fundus (the top of a mother’s uterus) can be measured from the pubic bone. This measurement in centimeters usually corresponds with the number of weeks of pregnancy after the 20th week. If the measurement is low for the number of weeks, the baby may be smaller than expected.
Other diagnostic procedures may include the following:
- Ultrasound. Ultrasound (a test using sound waves to create a picture of internal structures) is a more accurate method of estimating fetal size. Measurements can be taken of the fetus’ head and abdomen and compared with a growth chart to estimate fetal weight. The fetal abdominal circumference is a helpful indicator of fetal nutrition.
- Doppler flow. Another way to interpret and diagnose IUGR during pregnancy is Doppler flow, which uses sound waves to measure blood flow. The sound of moving blood produces wave-forms that reflect the speed and amount of the blood as it moves through a blood vessel. Blood flow through blood vessels in both the fetal brain and the umbilical cord can be checked with Doppler flow studies.
- Mother’s weight gain. A mother’s weight gain can also indicate a baby’s size. Small maternal weight gains in pregnancy may correspond with a small baby
- Gestational assessment. Babies are weighed within the first few hours after birth. The weight is compared with the baby’s gestational age and recorded in the medical record. The birthweight must be compared to the gestational age. Some doctors use a formula for calculating a baby’s body mass to diagnose SGA.
Small for gestational age treatment
Treatment will depend on your child’s symptoms, age, and general health. It will also depend on how severe the condition is.
Babies with small for gestational age may be physically more mature than their small size would suggest. But they may be weak and less able to take large feedings or stay warm.
Specific treatment for SGA will be determined by your baby’s doctor based on:
- Your baby’s gestational age, overall health, and medical history
- Extent of the condition
- Your baby’s tolerance for specific medications, procedures, or therapies
- Expectations for the course of the condition
- Your opinion or preference
Babies with SGA may be physically more mature than their small size indicates. But they may be weak and less able to tolerate large feedings or to stay warm. Treatment of the SGA baby may include:
- Temperature controlled beds or incubators
- Tube feedings (if the baby does not have a strong suck)
- Checking for hypoglycemia (low blood sugar) through blood tests
- Monitoring of oxygen levels
Babies who are SGA and are also premature may have additional needs including oxygen and mechanical help to breathe.
References [ + ]





{kind=link}