
Contents
Postpartum thyroiditis
Postpartum thyroiditis is inflammation of the thyroid gland (thyroiditis) that occurs in women after the delivery of a baby or within the first year after childbirth. Postpartum thyroiditis occurs within 6 months (typically 2 to 4 months) after delivery 1). Thyroiditis can cause both thyrotoxicosis (high thyroid hormone levels in the blood) and hypothyroidism (low thyroid hormone levels in the blood). In postpartum thyroiditis, thyrotoxicosis occurs first followed by hypothyroidism 2). Not all women demonstrate evidence of going through both phases; approximately 1/3 of women will manifest both phases, while 1/3 of women will have only a thyrotoxic or hypothyroid phase. The thyrotoxic phase (high thyroid hormone levels in the blood) lasts for 1-3 months and is associated with symptoms including anxiety, insomnia, palpitations (fast heart rate), fatigue, weight loss, and irritability. The hypothyroid phase (low thyroid hormone levels in the blood) typically occurs 1-3 months after the thyrotoxic phase and may last up to 9 – 12 months. Typical symptoms include fatigue, weight gain, constipation, dry skin, depression and poor exercise tolerance. Most women (~80%) will have return of their thyroid function to normal within 12 to 18 months after the onset of symptoms. But some women develop permanent complications.
Postpartum thyroiditis can be difficult to recognize because its symptoms are often mistakenly thought to be the stress of having a newborn and postpartum mood disorders.
In the United Status, postpartum thyroiditis occurs in approximately 5-10% of women. The incidence can be greater in certain high-risk populations.
Women at risk for developing postpartum thyroiditis include:
- Autoimmune disorders (such as Type 1, or juvenile onset, Diabetes Mellitus)
- Positive anti-thyroid antibodies (risk correlates with antibody levels, the higher the antibody the higher the risk)
- History of previous thyroid dysfunction
- History of previous postpartum thyroiditis (20% of women will have recurrence of thyroiditis with additional pregnancies)
- Family history of thyroid dysfunction.
Postpartum thyroiditis key points
- Postpartum thyroiditis happens when a woman’s thyroid becomes inflamed after having a baby. It may first cause the thyroid to be overactive. But in time it can lead to an underactive thyroid.
- Experts don’t know what causes postpartum thyroiditis.
- You are more likely to get it if you had antithyroid antibodies before pregnancy. Other risk factors include having type 1 diabetes or a history of thyroid problems.
- A blood test can often tell if you have an overactive or underactive thyroid.
- Treatment is based on how severe your symptoms are.
Thyroid gland
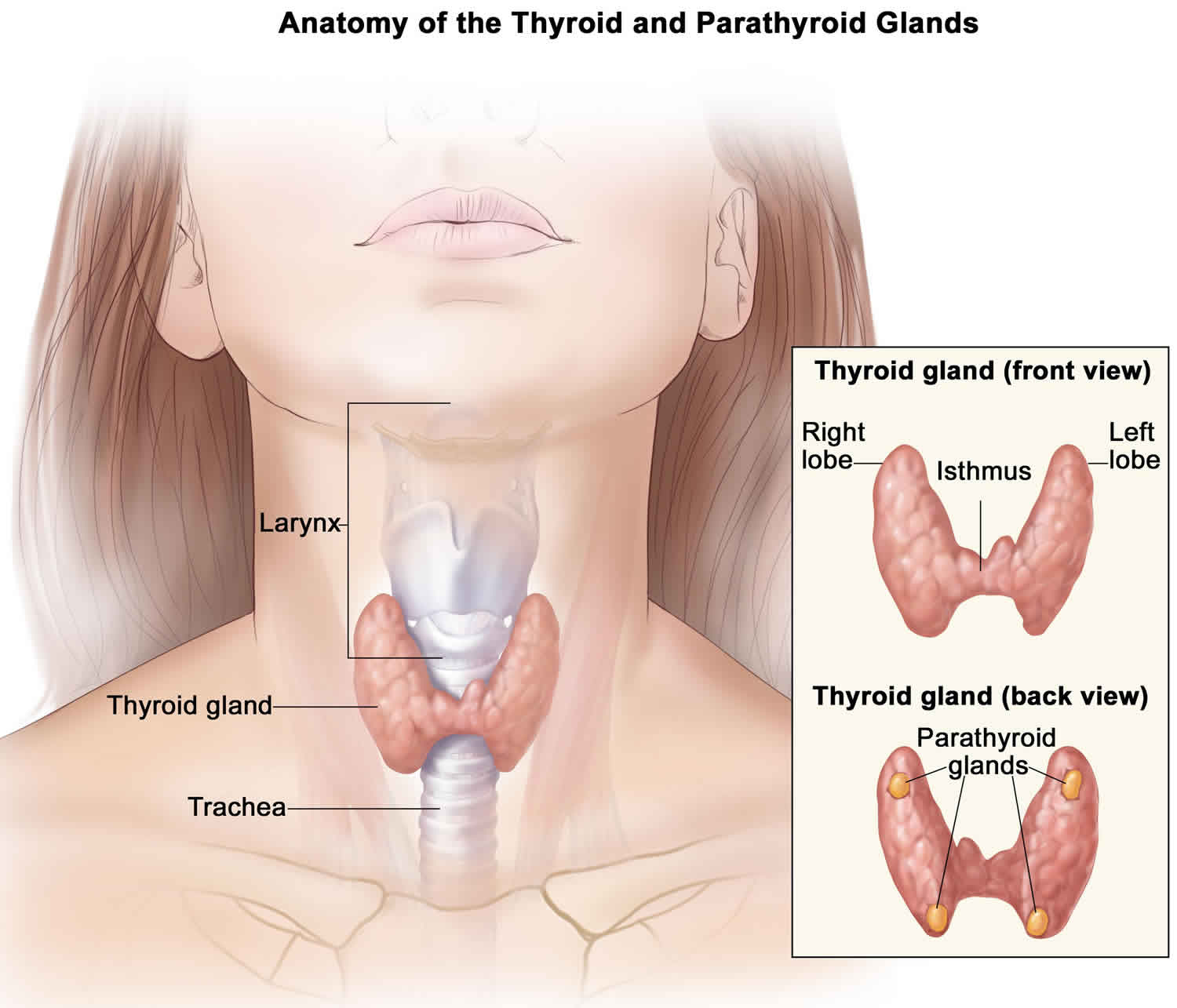
The thyroid gland is a butterfly-shaped endocrine gland that is normally located in the lower front of the neck. The thyroid’s job is to make thyroid hormones, which are secreted into the blood and then carried to every tissue in the body. Thyroid hormones help the body use energy, stay warm and keep the brain, heart, muscles, and other organs working as they should.
Figure 1. Thyroid gland
Postpartum thyroiditis causes
The exact cause of postpartum thyroiditis is not known but it is believed to be an autoimmune disease very similar to Hashimoto’s thyroiditis. As in Hashimoto’s thyroiditis, postpartum thyroiditis is associated with the presence of anti-thyroid antibodies (anti-thyroid peroxidase, anti-thyroglobulin) in early pregnancy and after childbirth. Women with positive antithyroid antibodies are at a much higher risk of developing postpartum thyroiditis than women who do not have have positive antibodies.
Risk factors for developing postpartum thyroiditis
You might be at increased risk of postpartum thyroiditis if you have:
- An autoimmune disorder, such as type 1 diabetes
- A history of postpartum thyroiditis
- High concentrations of anti-thyroid antibodies
- A history of previous thyroid problems
- A family history of thyroid problems
While further research is needed, some studies have also shown a link between postpartum thyroiditis and postpartum depression. As a result, if you have postpartum depression your doctor will likely check to see how your thyroid is functioning.
Postpartum thyroiditis prevention
While you might not be able to prevent postpartum thyroiditis, you can take steps to care for yourself in the months after childbirth. If you have any unusual signs or symptoms after childbirth, don’t assume they’re related to the stress of caring for a newborn. If you’re at increased risk of postpartum thyroiditis, talk to your health care provider about how to monitor your health.
Postpartum thyroiditis symptoms
During postpartum thyroiditis, you might experience two phases. The classic description of postpartum thyroiditis includes thyrotoxicosis (high thyroid hormone levels in the blood) followed by hypothyroidism (low thyroid hormone levels in the blood). Not all women appear to go through both phases; approximately 1/3 of patients will manifest both, while 1/3 of patients will have only a thyrotoxic or only a hypothyroid phase. Keep in mind, however, that some women who have postpartum thyroiditis develop symptoms of only hyperthyroidism or only hypothyroidism.
The thyrotoxic phase occurs 1-4 months after delivery of a child and lasts for 1-3 months.
The inflammation and release of thyroid hormone might first cause mild signs and symptoms similar to those of an overactive thyroid (hyperthyroidism), including:
- Anxiety
- Irritability
- Rapid heartbeat or palpitations (fast heart rate)
- Unexplained weight loss
- Increased sensitivity to heat
- Fatigue
- Tremor
- Insomnia
These signs and symptoms typically occur one to four months after delivery and last one to three months. Since these symptoms may often be attributed to changes after delivery and the stress of having a new baby, the thyrotoxic phase of post-partum thyroiditis is often overlooked.
Later, as thyroid cells become impaired, mild signs and symptoms of underactive thyroid (hypothyroidism) might develop, including:
- Lack of energy
- Fatigue
- Increased sensitivity to cold
- Constipation
- Dry skin
- Weight gain
- Poor exercise tolerance
- Depression
These signs and symptoms typically begin four to six weeks after the symptoms of hyperthyroidism resolve and can last six to 12 months.
It is much more common for women to present during the hypothyroid phase. This typically occurs 4-8 months after delivery and may last up to 9 –12 months. Most women will regain normal thyroid function within 12-18 months after the onset of symptoms. However, approximately 20% of those that go into a hypothyroid phase will remain hypothyroid.
Postpartum thyroiditis complications
For most women who develop postpartum thyroiditis, thyroid function eventually returns to normal — typically within 12 to 18 months of the start of symptoms. However, some women who experience postpartum thyroiditis don’t recover from the hypothyroid phase. As a result, they develop hypothyroidism, a condition in which the thyroid gland doesn’t produce enough of certain important hormones.
Postpartum thyroiditis diagnosis
If you have signs and symptoms of postpartum thyroiditis, your doctor will check to see how your thyroid is functioning. He or she will use blood tests that measure the level of thyroid-stimulating hormone (TSH) and the level of the thyroid hormone thyroxine.
If you have risk factors for postpartum thyroiditis, your doctor will likely test the functioning of your thyroid three and six months after delivery.
If your thyroid test results are abnormal, your doctor will likely recommend further testing within one to two weeks.
In addition, if you develop postpartum thyroiditis, your doctor will likely check your thyroid annually afterward to see if you develop hypothyroidism.
Postpartum thyroiditis treatment
Treatment of postpartum thyroiditis depends on the phase of thyroiditis and degree of symptoms that a patient has. Most women who develop postpartum thyroiditis don’t need treatment during the hyperthyroid or hypothyroid phases of their condition. However, your doctor will likely monitor how your thyroid is functioning through blood tests every four to eight weeks. This will help him or her track whether abnormalities resolve themselves or detect the development of hypothyroidism.
If you develop severe signs and symptoms of hyperthyroidism (thyrotoxicosis), your doctor will likely recommend treatment with a drug that blocks the effects of thyroid hormone on the body (beta blocker) to decrease symptoms such as palpitations and tremors. Beta blockers typically aren’t recommended for women who are breast-feeding. However, the beta blocker propranolol (Inderal) might be recommended because in breast milk it’s not as concentrated as other beta blockers. As your symptoms improve, the medication can be reduced and stopped since the thyrotoxic phase is transient. Antithyroid medications are not used for the thyrotoxic phase since the thyroid is not overactive.
The hypothyroid phase may be treated with thyroid hormone replacement. If the hypothyroidism is mild, and the patient has few, if any, symptoms, no therapy may be necessary. If thyroid hormone therapy is started, treatment should be continued for approximately 6-12 months and then reduced to see if thyroid hormone is required permanently. This treatment involves daily use of the synthetic thyroid hormone levothyroxine (Levo-T, Synthroid, others).
When you stop taking the thyroid replacement medication your doctor will monitor you for the development of hypothyroidism. You might need blood tests after six weeks, three months, and then, if your test results remain normal, annually.
Thyroid hormone treatment
Thyroid hormone is used in two situations:
- to replace the function of the thyroid gland, which is no longer functioning normally (“replacement therapy“) and
- to prevent further growth of thyroid tissue (“suppression therapy“). Suppression therapy is used primarily in patients with thyroid cancer to prevent recurrence or progression of their cancer.
Many people have a thyroid gland that cannot make enough thyroid hormone for the body’s needs. This is called hypothyroidism and may be caused by a nonfunctioning thyroid gland (for example postpartum thyroiditis), by destruction of thyroid gland by surgery or radiation treatment or by a non-functioning pituitary gland. Hypothyroidism, is the most common reason for needing thyroid hormone replacement.
The goal of thyroid hormone treatment is to closely replicate normal thyroid functioning. Pure, synthetic thyroxine (T4) works in the same way as your own thyroid hormone would. Thyroid hormone is necessary for the health of all the cells in the body. Therefore, taking thyroid hormone is different from taking other medications, because its job is to replace a hormone that is missing. The only safety concerns about taking thyroid hormone are taking too much or too little. Your thyroid function will be monitored by your physician to make sure this does not happen.
When someone is first started on thyroid hormone the initial dose is carefully selected based on information such as a person’s weight, age, and other medical conditions. The dose will then need to be adjusted by a physician to keep the thyroid function normal. The physician will make sure the thyroid hormone dose is correct by performing a physical examination and checking thyroid stimulating hormone (TSH) levels.
There are several brand names of thyroid hormone available. Although these all contain the same synthetic T4 (thyroxine), there are different inactive ingredients in each of the brand names. In general, it is best for you to stay on the same brand name. If a change in brand name is unavoidable, you should be sure your physician is aware of the change, so that your thyroid function can be rechecked. If your pharmacy plan changes your thyroid hormone to a generic preparation, it is important for you to inform your physician.
Postpartum thyroiditis prognosis
Postpartum thyroiditis typical course is characterized by three sequential phases: the thyrotoxic, the hypothyroid and recovery phase. The thyrotoxic phase occurs 1–3 months after parturition and lasts for a few months, followed by hypothyroidism at 3–6 months after delivery. Finally, normal thyroid function is usually achieved within a year. Most patients have a complete remission, but some develop persistent hypothyroidism.
References [ + ]





{kind=link}