Contents
In toe walking
In-toe walking also called “pigeon-toed” or having “intoeing”, is when children who walk with their feet pointing inward. According to Columbia Orthopedics, 2 out of every 1,000 children will in-toe. In-toeing affects boys and girls equally, and is often noted to both legs and it occurs for a variety of reasons, but most cases are corrected on their own as the child grows up. This is why there aren’t many pigeon-toed adults. Parents of children who in-toe often report that their children fall over more frequently than expected.
Most children learn to walk with their feet pointing straight ahead. Some children (and a few adults) walk with their toes pointing in.
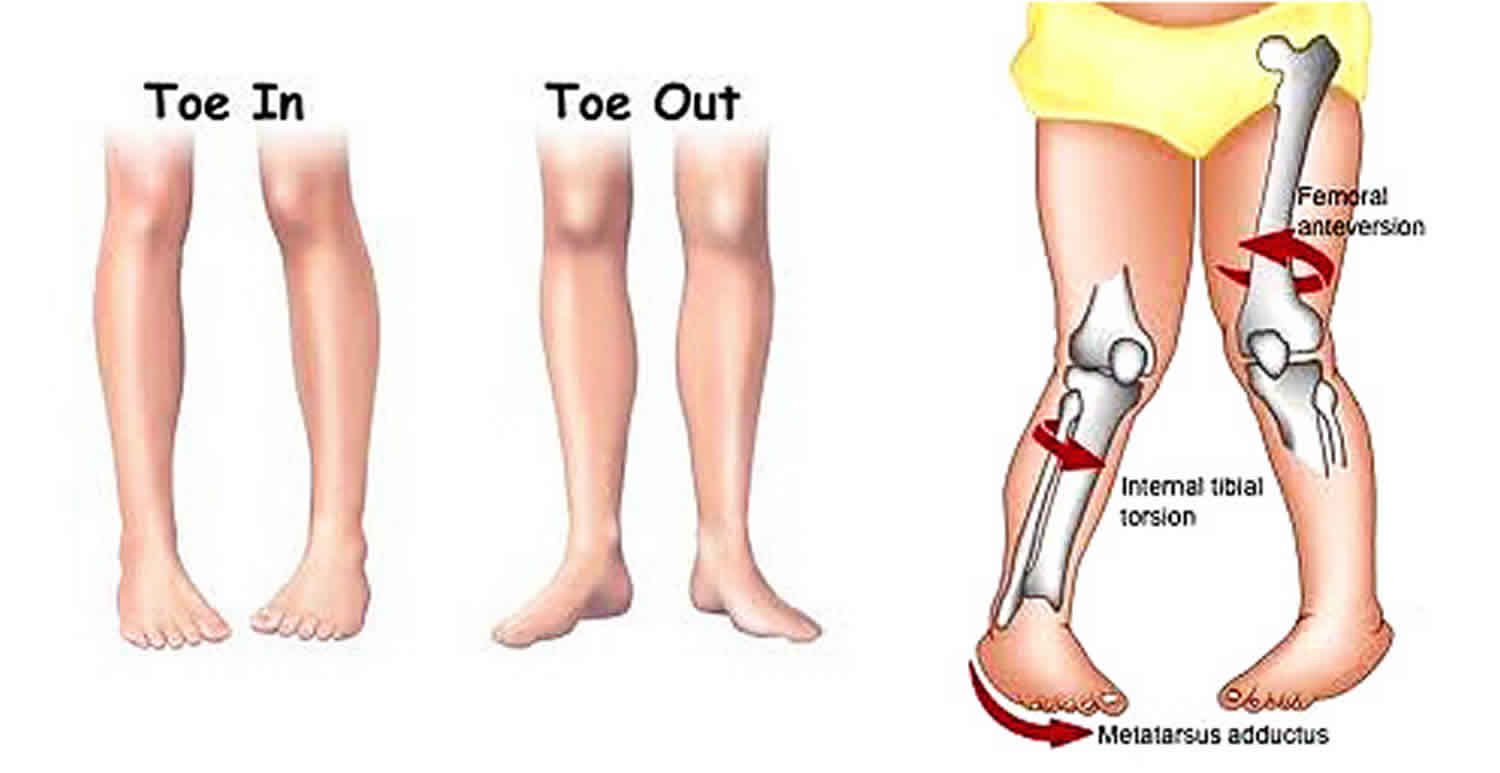
There are 3 main causes of in-toe walking:
- Femoral anteversion: A condition where the hip turns in.
- Tibial torsion: Where the lower leg turns (shin bone) in when compared to the upper leg.
- Metatarsus adductus: The bones in the foot turn in.
The most common cause of femoral anteversion is tibial torsion. Tibial torsion usually starts in-utero and disappears by the time the child is 5 or 6 years old. Femoral anteversion can also be started in-utero, and is usually corrected by age 9 or 10. Most of the time, in-toeing corrects itself with no intervention. Special shoes and braces used to be quite common in treating femoral anteversion, however, these have been proven to not be helpful in treating in-toeing.
Most of the time, in-toeing does not cause any problems with sports or leading a normal, healthy lifestyle. It has not been proven to cause arthritis in life, which is a common mis-conception. However, some children fall or trip more often when they are younger secondary to in-toeing. Physical therapy can help with balance reactions, safety awareness and strengthening to decrease the tripping and falling and help promote proper alignment.
If you are worried about your child’s in-toeing, or suspect that it is getting worse, talk with you pediatrician or contact a licensed pediatric physical therapist.
In-toe walking or intoeing key points
- Most children with intoeing do not need treatment as they will self-correct over time.
- Special shoes and braces aren’t usually needed and are only recommended by doctors for rare cases.
- Orthotics are not useful for correcting intoeing.
Figure 1. In toe walking
In-toe walking during infancy
Infants are sometimes born with their feet turning in. This turning occurs from the front part of their foot, and is called metatarsus adductus. It most commonly is due to being positioned in a crowded space inside the uterus before the baby is born.
You can suspect that metatarsus adductus may be present if:
- The front portion of your infant’s foot at rest turns inward.
- The outer side of the child’s foot is curved like a half- moon. This condition is usually mild and will resolve before your infant’s first birthday. Sometimes it is more severe, or is accompanied by other foot deformities that result in a problem called clubfoot.
This condition requires a consultation with a pediatric orthopedist and treatment with early casting or splinting.
In-toe walking in later childhood
When a child is intoeing during her second year, this is most likely due to inward twisting of the shinbone (tibia). This condition is called internal tibial torsion. When a child between ages three and ten has intoeing, it is probably due to an inward turning of the thighbone (femur), a condition called medial femoral torsion. Both of these conditions tend to run in families.
In-toe walking causes
There are three common causes of in-toe walking or intoeing:
- Tibial torsion –The shinbone (tibia) is the most common twisted bone. The twist can be caused by the way your baby lay in the womb while the bones were still soft. The bone slowly untwists as the child grows. Usually the twist is gone by school age.
- Femoral anteversion – The thigh bone (femur) can also be twisted inwards. This usually corrects itself, more slowly, by age nine or ten. In some children this doesn’t correct fully and these are the people who walk pigeon-toed as adults.
- Metartasus adductus – The feet are curved inwards. Most of these children also get better without treatment, but for those few children who have very curved feet, some bracing or special shoes may help in the first few years of life.
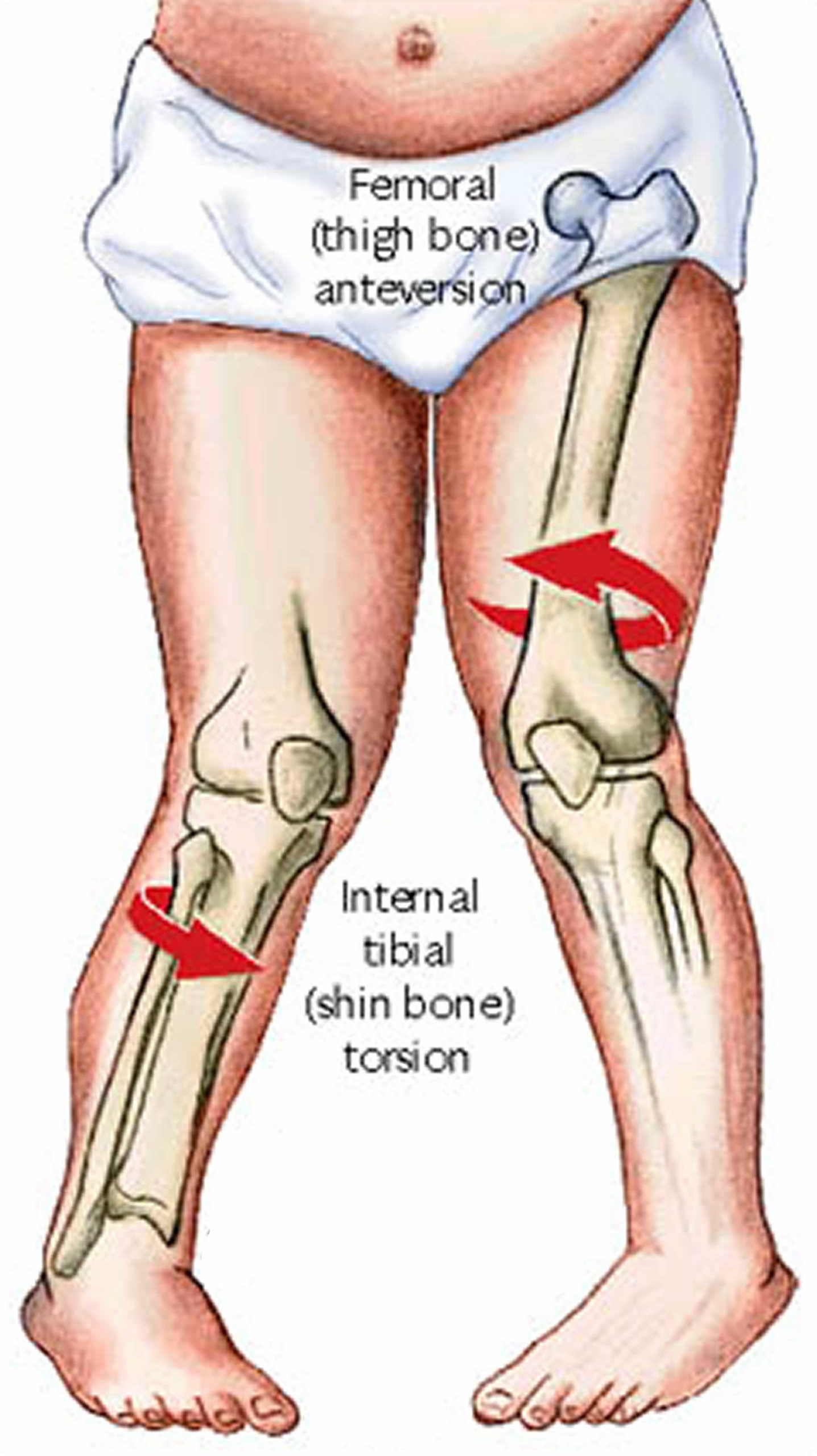
Two thirds of children with in-toe walking have an inwards twist to the top of their femur (thigh bone) at the hip. This is called femoral anteversion.
Some children may have an inwards twist to their tibia (shin bone). This is called internal tibial torsion.
In some children in-toe walking may be due to the shape their feet which are curved and tend to hook inwards. This is called metatarsus adductus.
Femoral anteversion
Children are all born with an inward twist in the femur below the hip joint. Most of children grow out of this by the age of two years. Some children take longer and tend to walk with their knees and feet turned inwards. They often like to sit with their legs in the ‘W’ position. In the vast majority of these children, this twist in the bone gradually disappears by the age of 7-8 years.
Treatment with splints, plasters or braces does not affect it, but your doctor may advise you to discourage your child from sitting in the ‘W’ position.
In a very few children, femoral anteversion persists in the long-term. It is never a functional problem, however, and they can participate in sports or other physical activities without problems. In extremely rare cases of teenagers who have a severe twist that causes pain at the hips or knees, an operation may be considered to correct it.
Internal tibial torsion
In-toe walking can often be caused by an inward twist of the tibia (shin bone). This is very common in babies and toddlers and is due to ‘moulding’ of the baby during pregnancy.
It may persist for a few years but gradually disappears as the child grows. Treatment with splints, plasters or braces does not alter it and is unnecessary.
Tibial torsion does not cause any functional problems and children can participate in all physical activities without suffering any long-term problems.
Metatarsus adductus
In-toe walking can sometimes be seen in children who have feet that are curved inwards (pigeon toes). This can also be due to ‘moulding’ during pregnancy. It is often seen in children who tend to sleep face down.
More than 80 percent of children grow out of this by the age of 3-4 years.
If the foot is supple and flexible (the doctor will check that) treatment is not necessary. In some children with more pronounced problems and feet that are less flexible, the doctor may recommend special shoes, splints to be worn at night or, rarely, treatment with plaster casts.
Very few children need an operation for their feet to be straightened. The vast majority of children with metatarsus adductus do not complain of any symptoms, can participate in all physical activities and have no long-term problems.
In-toe walking symptoms
Children who have intoeing or in-toe walking tend to trip a little more at first, but later on are fine. Children with intoeing are just as good at sport and are no more likely to get arthritis or back problems than anyone else. Intoeing should not get worse and your child should be able to take part in all types of physical activity.
If you are concerned about your child’s intoeing, you can take photographs or videos of your child walking every six months to keep a record of the changes. If you think your child’s intoeing is getting worse, a doctor should see them again. Many parents worry that their child will always walk with their feet turned in, however this hardly ever happens. No treatment has been proven to improve a child’s intoeing – it is best to just let it correct itself as your child grows.
In-toe walking treatment
Some experts feel no treatment is necessary for intoeing in an infant under six months of age. For severe metatarsus adductus in infancy, early casting may be useful.
The bone twisting conditions cannot be fixed with braces, shoe inserts or special shoes. These methods were used in the past and have been shown to have no effect. It has been found that the bones correct themselves without any treatment. There is no need to try to modify your child’s walking or sitting. This will not alter their development and can lead to frustration for the child and parent for no reason. Very occasionally your doctor may recommend a brace for a special reason.
Studies show that most infants who have metatarsus adductus in early infancy will outgrow it with no treatment necessary. If your baby’s intoeing persists after six months, or if it is rigid and difficult to straighten out, your doctor may refer you to a pediatric orthopedist who may recommend a series of casts applied over a period of three to six weeks. The main goal is to correct the condition before your child starts walking.
Intoeing in early childhood often corrects itself over time, and usually requires no treatment. But if your child has trouble walking, discuss the condition with your pediatrician who may refer you to an orthopedist. A night brace (special shoes with connecting bars) was used in the past for this problem, but it hasn’t proven to be an effective treatment. Because intoeing often corrects itself over time, it is very important to avoid nonprescribed “treatments” such as corrective shoes, twister cables, daytime bracing, exercises, shoe inserts, or back manipulations. These do not correct the problem and may be harmful because they interfere with normal play or walking. Furthermore, a child wearing these braces may face unnecessary emotional strain from her peers.
Nevertheless, if a child’s intoeing remains by the age of nine or ten years old, surgery may be required to correct it.





{kind=link}