Contents
Hemispherectomy
Hemispherectomy involves removing or disconnecting one hemisphere or one side of the brain that is least used and the source of your child’s seizures. Hemispherectomy is considered when seizures have continued despite medications for at least two years and seizures are traced to several parts of one hemisphere of the brain. Side effects of this surgery include speech problems and loss of movement and/or sensation on one side of the body. Your child will be monitored closely to identify the long-term effects. Your child will need to rehabilitation in the hospital and at home to help manage these side effects.
Complete removal of one hemisphere has some associated complications, so some neurosurgeons prefer to perform a functional hemispherectomy, in which only some sections of the brain are removed and other sections are disconnected. The end result of a functional hemispherectomy is that half the brain is completely disconnected from the other half and totally inactive. Your child’s neurologist and neurosurgeon will discuss the best surgical procedure for your child.
The aim of a hemispherectomy is to remove or disconnect that hemisphere that is least used and the source of your child’s seizures. During this procedure, the corpus callosum is also cut (callosotomy) to prevent the spread of seizures from the dysfunctional hemisphere to the functional hemisphere.
The largest part of the brain, the cerebrum, is organized into two hemispheres. In most people, the two hemispheres perform distinct functions.
- The left hemisphere is dominant for language in most people, and plays an important role in language, verbal memory, reading, writing, and arithmetic. It is concerned with sensation and movement on the right side of the body.
- The right hemisphere plays a large part in interpreting what we see and touch, and in non-verbal memory, music, and emotions. It is concerned with sensation and movement on the left side of the body.
The left hemisphere dominates language in almost all right-handed people and in many left-handed people. In some people, though, the two hemispheres share the language function more equally, and in a few people the right hemisphere may be dominant for language function. Right hemisphere and bilateral (two-sided) language centres are more common in young children and children with epilepsy.
Patients with the following clinical and neuroimaging features may be appropriate for a hemispherectomy procedure:
- Medically intractable epilepsy with seizures arising from the pathological side.
- Weakness of one side of the body with loss of dexterity of the hand with, or without, peripheral visual loss.
- Developmental retardation or arrest of maturation due to intractable seizures.
- Diffuse abnormality of one cerebral hemisphere which is contributing to the intractable epilepsy.
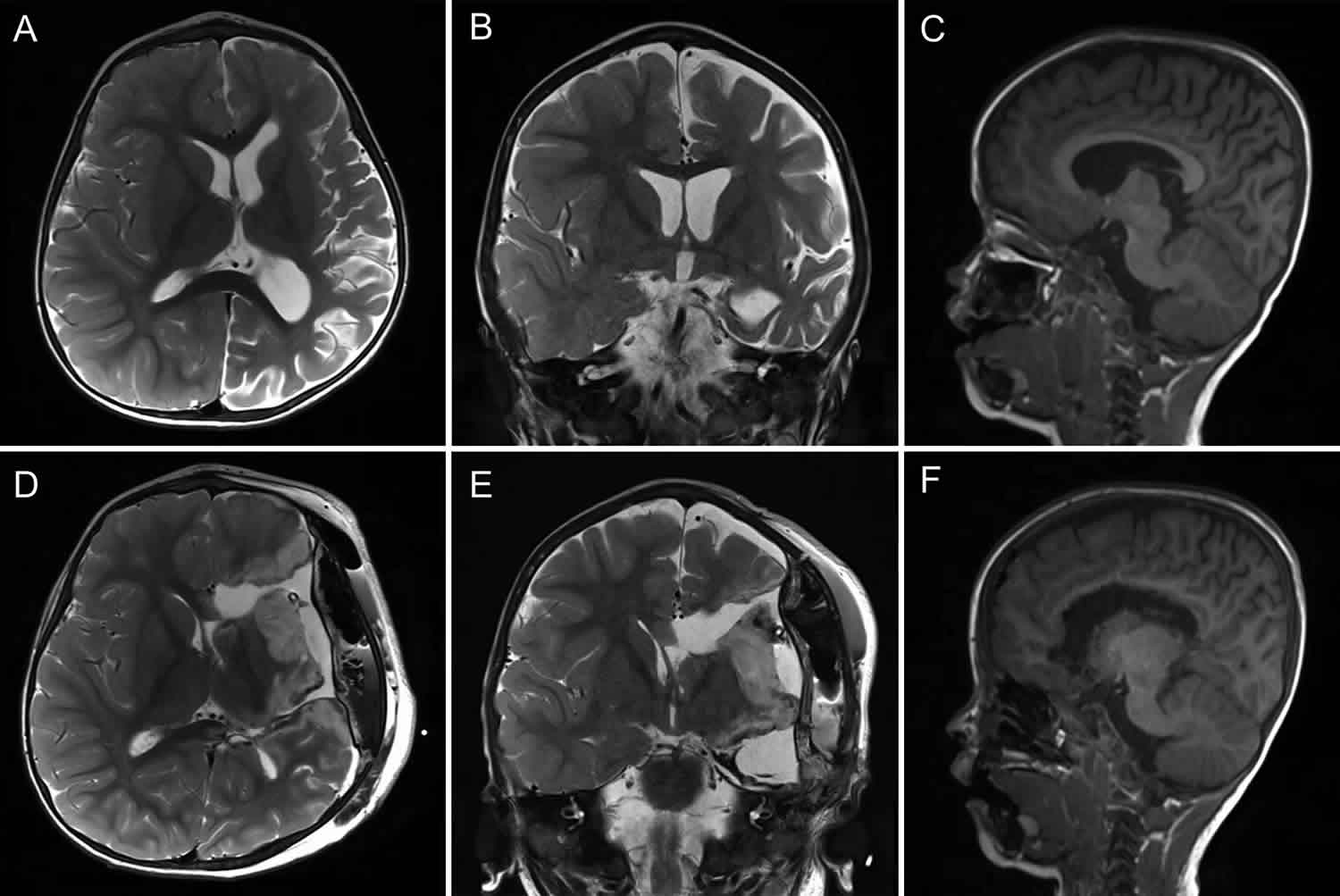
Diseases presenting with these symptoms include malformations of cortical development, perinatal infarction (stroke), hemimegalencephaly, Sturge-Weber-Dimitri disease, and Rasmussen’s encephalitis. Most of these patients start having seizures and weakness early in life. Once the diagnosis of epilepsy is suspected, the patient should be referred to a center specialized in the evaluation and management of pediatric epilepsy.
Figure 1. Human brain
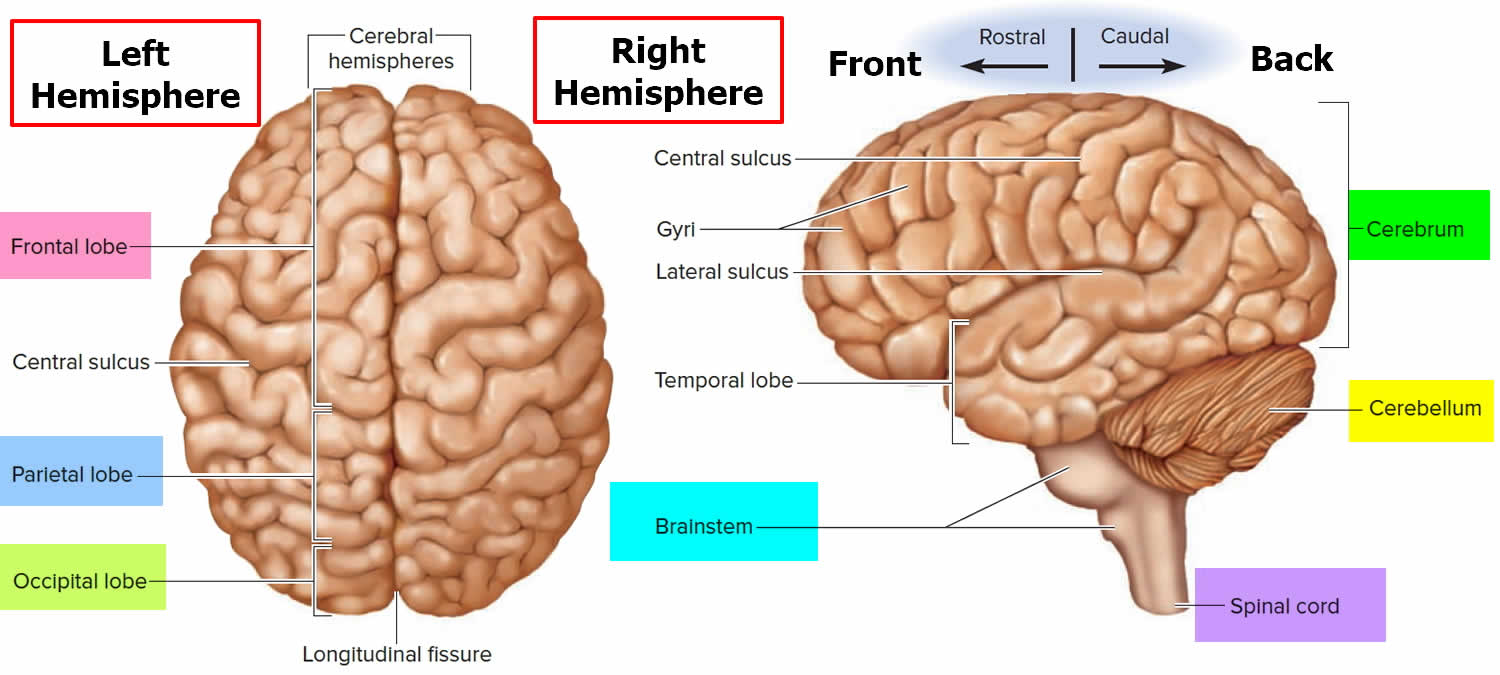
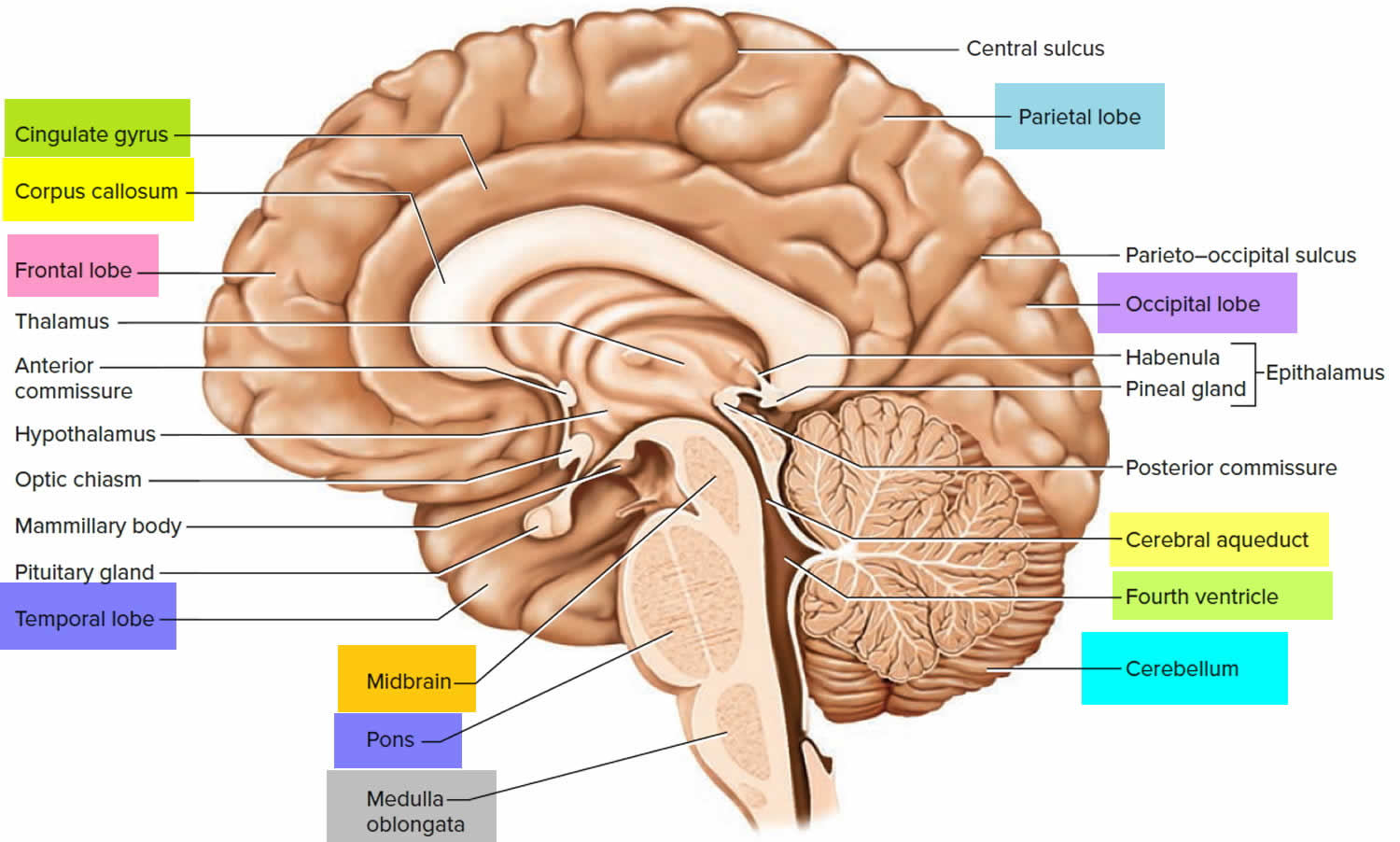
Figure 2. Medial aspect of the human brain
What can I expect from the hemispherectomy?
Every child is different. Depending on the nature of your child’s seizures and the location of the epileptogenic region, hemispherectomy may result in complete seizure control or “partial” seizure control with less need for medication. There may also be some chance that the surgery will not improve things. Talk to your child’s doctor about what you and your child can realistically expect as a result of the surgery.
How hemispherectomy affects the global functioning of a child (such as whether they walk, speak, and read) is known as functional outcomes. Unfortunately, functional outcomes are poorly addressed in published research papers.
Approximately 71% percent of children who have this procedure are seizure-free afterwards; however, the procedure leaves the child with physical and sensory deficits that are unavoidable. In this largest study to date, it was found that 1):
- 42% over the age of 6 have satisfactory reading skills;
- 60% participate in mainstream schools with assistance;
- 70% have satisfactory speaking skills;
- 83% are able to walk independently;
- 24% of adults who had the procedure in childhood are gainfully employed.
Vision
All children after surgery will have homonymous hemianopsia which is the permanent loss of the visual field opposite the removed hemisphere. This is more than a loss of peripheral vision – it is loss of half the visual field in each eye, including half the central (foveal) vision.
Hearing
Because one temporal lobe is removed or disconnected, mild-to-severe listening impairments (known as central auditory processing disorder) can occur. This affects hearing and listening in various environments, especially loud environments or with multiple speakers.
Movement
Because the surgery removes or disconnects the upper motor neurons from one side of the brain that are responsible for intentional movement on the opposite side of the body, the child is left with hemiparesis – a significant weakness of the opposite side of the body. Existing connections to the motor neurons of the remaining part of the brain, however, make it possible for the child to recover some movement, including the ability to walk and use the affected hand as an assist or for some bimanual activities. Although fine motor of the hand will be impaired greatly, the child should be able to move their shoulder, upper arm, and sometimes wrist over time. Some finger movement, especially closing of the hands, can occur after appropriate interventions.
The weakness is most significant in the days and weeks after surgery, with the opposite arm and leg often totally floppy (flaccid). This is known as hypotonia (decreased activity of spinal circuits because of sudden deprivation of input from the brain). After the hypotonic phase is over, some of the movements will return most at the shoulder and hips. Some children do not experience a hypotonic phase at all.
Hemiparesis is associated with clonus, spasticity, and contracture. Children should be monitored closely as spasticity almost always increases over time, and can eventually lead to permanent contracture of the muscles. Shortened, contracted muscles can pull out bones from their sockets and lead to hip dysplasia and subluxation, painful shoulder subluxation, and other issues which often require surgery.
Children with hemiparesis often have difficulties maintaining their balance due to weakness. Performing daily living tasks such as dressing, eating, grabbing objects, or using the bathroom may be difficult for some children. Most require the use of orthotic devices to keep the feet in proper alignment.
Hemiparesis is part of the upper motor neuron syndrome, which includes weakness of the opposite side of the body, decreased speed, accuracy, and dexterity of the hand, altered muscle tone, decreased endurance, and exaggerated deep tendon reflexes including spasticity and contracture. Surgery also causes some reduced dexterity, strength, and fine motor skills in the “unaffected” hand. This may later cause difficulty with writing, drawing, force production, and pressure sensitivity.
Speech
In approximately 95% of typically-developing children, speech and language is a function of the left hemisphere of the brain; however, after left hemispherectomy surgery, approximately 44 – 76% of children have expressive and receptive language skills depending on the underlying condition which caused the seizures. Some are even bilingual.
Expressive speech can be challenging after hemispherectomy. Children who spoke prior to the surgery may take several years to fully return to baseline. Additionally, children who did not speak prior to hemispherectomy have been known to speak afterwards, even when surgery occurred as late as nine years old.
Because the surgery removes parts of the brain responsible for motor planning and intentional movement, many children after hemispherectomy are diagnosed with apraxia. Apraxia is a motor speech disorder where the child has problems saying sounds, syllables, and words; the child knows what he/she wants to say, but the brain has difficulty the muscle movements necessary to say it.
Many children have challenges with articulation (making clear speech sounds) and prosody (patterns of stress and intonation) which may be caused by motor planning challenges or motor deficits related to hemiplegia, which can also affect the oral muscles used in speech.
Sensation
Research 2) shows that sensitivity to heat, cold, and pain will be impaired in the hand, forearm, and upper arm opposite the removed hemisphere, and will vary in severity from child to child. The reduced sensitivity is most significant in the hand. This puts children at risk of unknown broken bones after falls because their pain reaction is significantly reduced, or burns. Also, sensitivity to hot and cold is impaired in the arm on the same side of the removed hemisphere in the upper arm area.
Eating and Drinking
Approximately 26% of children will have difficulty eating and drinking right after surgery. Very limited research shows that symptoms lasted a median of 19 days. Anecdotally, some children require a gastric tube to be placed for several years and sometimes months.
Headaches
Except in cases of true anatomical hemispherectomy, the disconnected hemisphere will continue to seize. Research indicates that these disconnected seizures can cause headaches. Headaches can also be caused by the craniotomy and in 30% of individuals who have craniotomy, the headaches can be ongoing. Headaches are also a sign of hydrocephalus, which should be ruled out.
What are the chances of total seizure control after hemispherectomy?
A recent systemic review of 15 studies which address seizure outcomes across several different hemispherectomy procedures shows that the long-term seizure control rate at five years or more after surgery is 71%.
What factors affect seizure control?
Children whose seizures began after 3 1/2 months of age have a higher chance of long-term seizure control. Also, children who have abnormal MRI findings prior to surgery also have higher rates of control. Sturge-Weber syndrome, Rasmussen’s encephalitis, and pediatric stroke syndrome have the highest seizure control rate of approximately 80%.
Children with hemimegalencephaly have the lowest at seizure control rate at approximately 66%.
Hemispherectomy indications
Hemispherectomy is considered when:
- seizures have persisted, despite trying medication (monotherapy and polytherapy) for at least two years
- pre-surgical evaluation shows multifocal epileptic activity (seizures arising from several areas of the brain) restricted to one hemisphere.
Hemispherectomy is often used for intractable seizures associated with hemimegalencephaly (overgrowth of one side of the brain). Hemispherectomy is also used in children with a dysfunctional hemisphere as a result of Rasmussen’s encephalitis or Sturge-Weber syndrome.
Generally, the earlier in life that this operation is done the more likely the child is to compensate for the loss of one hemisphere. The younger the child, the more flexible (plastic) the brain is and the better the remaining side can compensate for the operated side. However, the child must be at least several months old before they can have the surgery.
Patients who have congenital hemiplegia and atrophy or poor development of one cerebral hemisphere may also have broad areas of almost continuous seizure discharges over that hemisphere. Often, seizures in these individuals are refractory to medication. In some of these patients, the seizure discharges cross the corpus callosum and interfere with the function of the opposite, normal hemisphere as well. Cognitive function may be severely handicapped, as is normal fine movement of the foot and hand on the side opposite the affected hemisphere.
If the affected cerebral cortex, which is propagating significant seizure discharges but is not mediating useful neurologic function, is removed surgically, these patients will often experience dramatic improvement not only in seizure control, but also in overall neurologic function. This improvement is the result of eliminating the negative effect of the impaired hemisphere on the unaffected, normal side of the brain.
Patients are considered for hemispherectomy if they have one of a variety of neurologic disorders that typically affect one half of the brain, including:
- Rasmussen’s encephalitis
- Sturge-Weber syndrome
- Hemimegalencephaly
- Porencephalic cyst from a large congenital stroke
About 85% to 90% of patients undergoing hemispherectomy experience arrest of their seizures, accompanied in most cases by dramatic improvement in function, including further cognitive development.
Hemispherectomy types
There are several different types of hemispherectomy procedures. They include the anatomical hemispherectomy, subtotal hemispherectomy, the functional hemispherectomies, and the hemispherotomies. There are also other procedures which fall under this category which include hemidecortication and other newer procedures. Surgeons are not trained in all techniques and some techniques are more complicated than others. Most surgeons perform only the procedures they have been trained to perform and are familiar with.
Two types of hemispherectomies commonly performed include anatomic hemispherectomy and functional (disconnective) hemispherectomy as shown in Figures 3 and 4. Anatomic hemispherectomy involves the removal of the frontal, parietal, temporal, and occipital lobes. The deeper structures, such as the basal ganglia, thalamus and brain stem are left in place. The anatomic hemispherectomy has a slightly higher risk of blood loss and delayed hydrocephalus. It is typically performed for patients with hemimegalencephaly. The functional technique involves removing a smaller area of the affected hemisphere and disconnecting the remaining brain tissue. This disconnection includes a corpus callosotomy and allows for electrical isolation of the hemisphere that is left in place. This technique involves less risk of blood loss and hydrocephalus but is not appropriate for all patients. Outcomes after both types of epilepsy surgery are reported to be equal and approach 70% seizure freedom.
Anatomical hemispherectomy
A true anatomical hemispherectomy is when all four lobes of one hemisphere of the cerebral cortex are removed in their entirety. They may be removed “en bloc” (all together) or in pieces. Because of where they are located within the brain, the amygdala and hippocampus on the affected side are removed. Sometimes the surgeon removes the thalamus and basal ganglia on the affected side as well. Technically, this is the least complicated of all the hemispherectomy procedures.
Anatomical hemispherectomy is often used today in many surgical facilities, usually for cases such as hemimegalencephaly where functional hemispherectomy can sometimes be unsuccessful.
There are significant short- and long-term complications that are associated with this procedure:
- Hydrocephalus: Hydrocephalus is a common side effect of anatomical hemispherectomy, with this study 3) of 690 patients finding it in 30% of cases. Hydrocephalus is a risk throughout the lifespan, with 27% of children developing hydrocephalus three or more months after surgery;
- Superficial hemosiderosis is an extremely rare condition caused by chronic iron deposits on brain tissue. This was reported as a late complication of anatomical hemispherectomy in the early research papers. Blood product in the cerebrospinal fluid, whether left behind from the surgery or caused by blood leaking from tiny rips and tears in capillaries that can occur over time due to brain shift or dislodging of the hemisphere, is one possible cause of this condition. Symptoms of superficial hemosiderosis include gait imbalance, progressive loss of hearing which sometimes begins as ringing of the ears (tinnitus), vertigo, and other symptoms. Because the delayed mortality rate was reported as high as 40% for those with superficial hemosiderosis after hemispherectomy, anatomical hemispherectomy was largely abandoned in the early 1970s by many facilities. It is now believed that the high mortality rate may have been due to untreated hydrocephalus rather than superficial hemosiderosis in many of the early cases. Superficial hemosiderosis has not been reported in medical literature in over 30 years; however, there are anecdotal reports from parents of adults who had childhood anatomical hemispherectomy. It has also been reported many years after functional hemispherectomy;
- Brain shift into the resection cavity, microvascular tearing, and dislodging of the remaining hemisphere. The incidence of these risks is unknown.
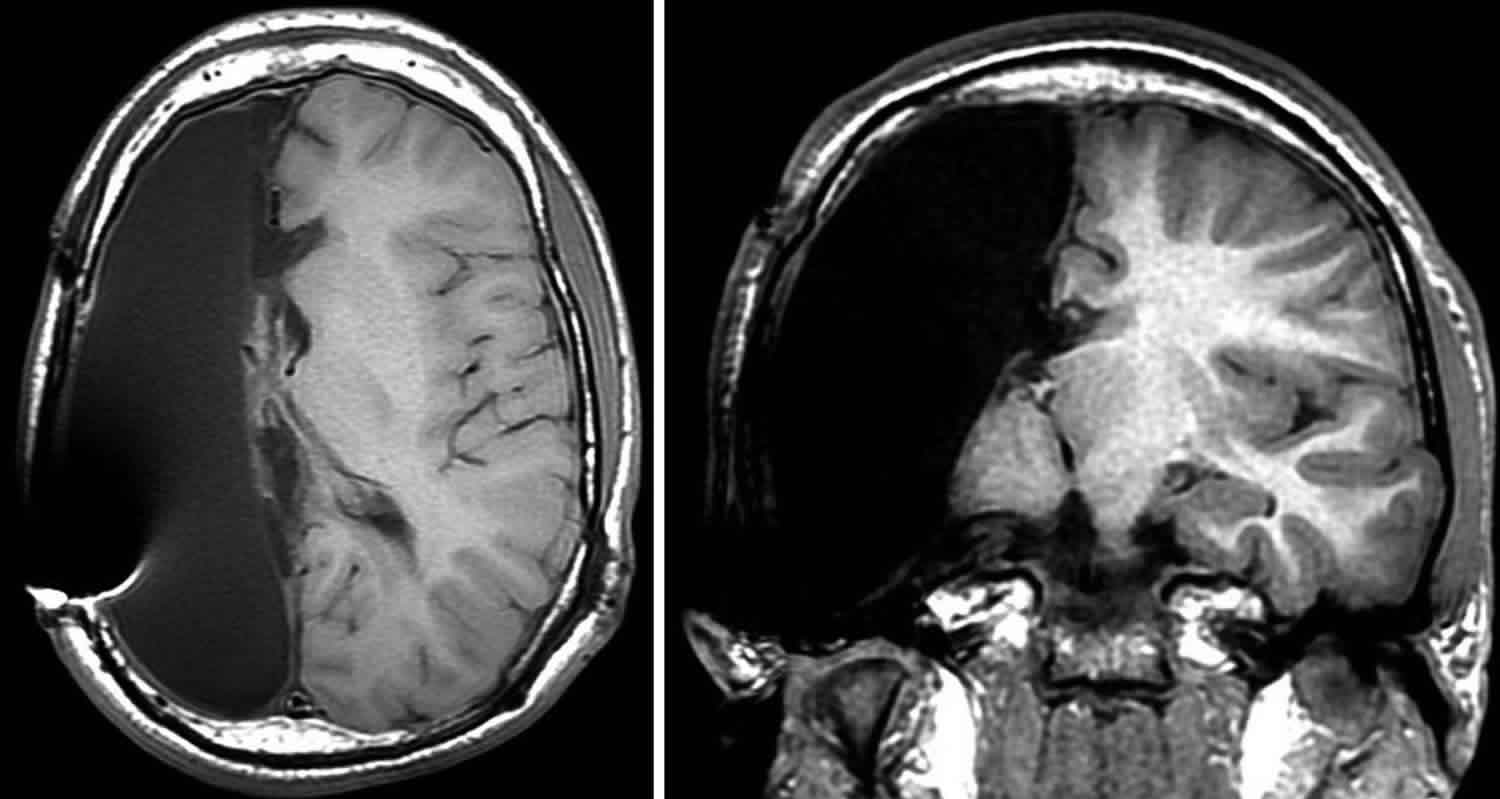
Figure 3. Right anatomic hemispherectomy
Functional hemispherectomy
Functional hemispherectomy is any procedure which disables the function of one cerebral hemisphere but does not remove the hemisphere itself.
Rasmussen was the first epilepsy surgeon to develop the functional hemispherectomy technique and is the most common technique today. The temporal lobe is removed but the frontal pole and occipital pole are preserved. This provides access to connections in the front and back of the hemisphere and the midbrain which the surgeon cuts and allows the surgeon to perform a complete corpus callosotomy. The brain that is left behind is living because the veins and arteries which provide its blood supply are not cut. For this reason, the remaining part of the brain may still seize, but because the axonal connections are severed, the seizures do not spread and have no effect.
Risk of this procedure include incomplete disconnection. Incomplete disconnection rates have been reported between 7 – 52%, thus requiring reoperation.
Figure 4. Left Functional Hemispherectomy
Hemispherotomy
Although often classified as a type of functional hemispherectomy, hemispherotomies are technically different than functional hemispherectomy. As with functional hemispherectomy, living brain is left behind with an intact blood supply, but the diseased/affected hemisphere of the brain is disconnected from healthy brain. In the last 25 years, there has been a shift towards the functional hemispherectomy and hemispherotomy due to the significant risks of a true anatomical hemispherectomy.
The distinction between hemispherotomy and functional hemispherectomy is that in hemispherotomy less brain tissue is removed than in functional hemispherectomy in order to reduce the chances of excessive bleeding during surgery, hydrocephalus, and tearing of very small blood vessels and veins over time which can lead to superficial hemosiderosis. Because so little brain tissue is removed, the surgeon is really making a hole (or holes) in the hemisphere (-otomy) rather than removing large sections of brain (-ectomy).
The different hemispherotomy techniques were introduced in the 1990s and include the modified lateral hemispherotomy, the vertical parasagittal hemispherotomy, and the peri-insular hemispherotomy. These techniques are continually refined today and are the main technique used at most epilepsy centers in the 21st century. It is important to note that techniques may vary from center to center.
Peri-Insular Hemispherotomy
First described in 1995, there have been several modifications to this technique over the years. In this technique, the surgeon will disconnect the affected hemisphere through the ventricles of the brain (the areas in red below). Because the ventricles are very deep within the brain, the surgeon must create several “windows” or holes through the brain so the ventricles can be accessed. These holes are cut through the affected hemisphere above and below the insular cortex (thus the name peri (around) insular hemispherotomy.) Very little brain matter is removed during surgery.
What are the benefits of peri-insular hemispherotomy?
Generally, the benefits of this procedure are shorter time in surgery and less intraoperative blood loss than other hemispherectomy techniques. Some children, however, may require blood transfusion during surgery.
What are the risks of peri-insular hemispherotomy?
The greatest risk of peri-insular hemispherotomy is incomplete disconnection.
Post-operative fevers, meningitis, and irritability are reported as less after peri-insular hemispherotomy than other techniques. Some research shows that the incidence of hydrocephalus after peri-insular hemispherotomy is as low as 0 – 4%; however, a recent large study of 690 children and adults who have had hemispherectomy shows the rate as high as 23% for functional hemispherectomy in general. Parents should continue to look out for symptoms of hydrocephalus throughout the lifespan.
Death is extremely rare after peri-insular hemispherotomy. Only two are reported in the literature. One was due to brain swelling from stroke in the disconnected hemisphere or bleeding. One case is believed to have been caused by brain shift.
Seizure control rates are reported as high as 90% after peri-insular hemispherotomy. The highest seizure control rates are reported where the condition which causes the seizures is stroke or Rasmussen’s encephalitis; the lowest seizure control rates are with cortical dysplasia and hemimegalencephaly
Modified Lateral Hemispherotomy
Modified lateral hemispherotomy is similar to peri-insular hemispherotomy, but differs because:
- the middle cerebral artery is severed to limit blood loss and
- a central block of cortex (the operculum) is removed to allow the surgeon access to the ventricles, remove the insula, and portions of the basal ganglia and thalamus. The anterior temporal lobe is also removed.
Hydrocephalus is also a post-operative risk, with 23% of children developing hydrocephalus after functional hemispherectomy.
Hemispherectomy procedure
Before hemispherectomy surgery
A thorough pre-surgical evaluation is essential to confirm that there is no other treatment option. This may include:
- EEG and MRI to help identify the dysfunctional hemisphere
- functional mapping using fMRI, a Wada test or MEG to determine which hemisphere is dominant for critical functions such as speech and memory (if the child is old enough)
- neuropsychological tests to establish your child’s baseline functioning.
The surgeon and the team will explain the surgery to you and discuss all related issues. They will instruct you on any specific steps to take prior to the operation.
They will also discuss post-operative symptoms, any intensive care and rehabilitation that will be required and possible ongoing deficits and care.
Hemispherectomy surgery
The operation will take about six hours and will require a general anaesthetic. Children are given a general anesthesia prior to the surgery. To prepare for the surgery, part of your child’s hair will be shaved.
An incision will be made and a craniotomy will be performed (removal of a piece of the skull that will be replaced at the end of the surgery). The surgeon may remove some parts of the brain and disconnect other parts. The corpus callosum will be cut to prevent the spread of seizures to the functional side of the brain.
Formerly, the entire cortical mantle was removed (also called “anatomic hemispherectomy”). However, this technique was associated with a late complication characterized by hemorrhage into the large resection cavity, which became filled with cerebrospinal fluid. Sensorineural hearing loss occurred as rising iron levels in the spinal fluid from the breakdown of blood gradually proved toxic to the eighth cranial nerve. Another complication was the occurrence of hydrocephalus.
Current techniques entail disconnecting the white matter fiber connections from the entire cortex to the opposite hemisphere and to the deeper brain structures, while leaving intact the brain substance and vascular structures supporting these cortical areas (also called “functional hemispherectomy”). This method has a similar success rate for most conditions, except for hemimegalencephaly. Because the empty postoperative cavity in the affected half of the cranium is minimized, the complications associated with anatomic hemispherectomy are greatly reduced.
At the end of the procedure, the skull will be replaced and the scalp will be sutured closed. The surgery takes about six hours.
What to expect after hemispherectomy surgery
Your child will be in the Intensive Care Unit (ICU) overnight or until he or she is medically stable enough to go to another nursing unit. While still in the ICU, your child will be observed continuously and blood pressure, pulse and respiration will be checked frequently.
Once out of the ICU your child will probably require an additional five to seven days of hospitalization. Inpatient or outpatient rehabilitation may be necessary to optimize your child’s recovery. Your child will be evaluated carefully over the next few months to see what effect surgery had on the seizures and whether there are persistent complications.
Hemispherectomy side effects
Most children have excellent long-term results following hemispherectomy with no unexpected adverse outcomes. Occasionally, however, some complications may occur.
- Early complications, which occur either during the intraoperative (complications from anaesthetic) or immediate postoperative period include intraoperative blood loss, electrolyte changes, hypothermia, cerebral edema (swelling) and aseptic meningitis.
- Late onset complications can occur months or years after the hemispherectomy. These hydrocephalus or accumulation of cerebrospinal fluid within the ventricles of the brain and recurrence of seizures, though rare, can be life threatening and need to be treated urgently. Hydrocephalus may require insertion of a shunt, which diverts the fluid to another compartment of the body, where it is absorbed naturally.
Hydrocephalus is the most significant risk after hemispherectomy surgery. This risk is across the lifespan, with cases reported ten or more years after surgery. Approximately 23% of patients will develop hydrocephalus, with 27% of those children developing hydrocephalus 90 days or more after surgery. The risk of developing hydrocephalus is 20% after functional hemispherectomy and 30% after anatomical hemispherectomy. Children with hemimegalencephaly have a higher chance of developing hydrocephalus – about 40%.
Blood loss requiring transfusion is also risk, especially for babies and infants. In very rare cases, stroke, brain swelling (cerebral edema), or other complications can occur.
Post-operative fevers are common after surgery and may occur for several months later. This is because blood product and protein in the cerebrospinal fluid from the surgery can irritate the brain, causing the body to respond as though there is an infection. Most surgeons use an external ventricular drain to evacuate blood product and other matter from the cerebrospinal fluid, as well as to monitor intracranial pressure. The use of this drain can also reduce the incidence of fevers after surgery.
Potential complications of hemispherectomy in children:
- Scalp numbness
- Nausea
- Fatigue
- Depression
- Headache
- Difficulty with speech and memory
- Developmental problems
- Loss of peripheral vision
Neuropsychological tests will be performed to detect any changes in your child’s function.
As with any surgery, there is a potential for complications. The major problems that could develop are bleeding and infection. Other risks of this procedure include developmental problems and loss of peripheral vision.
Weakness on the opposite side from the operation site may occur. But children can function with only half a brain because the remaining side takes over many of the functions of the half that was removed. If the surgery is done early in childhood, the child is more likely to compensate for the loss of one side of the brain.
Hemispherectomy recovery
After hemispherectomy surgery, children will spend 2-3 days in the pediatric intensive care unit (PICU) for close monitoring of their neurological status. Antiepileptic medications are continued at previous doses. Antiepileptic drug levels in the blood for some anti-epileptics, like carbamazepine and oxcarbazepine, are monitored during this period because of the drug interaction with anesthesia. An MRI is performed on the first postoperative morning to assess the brain after resection. Once the surgical drains are removed, the patient will be transferred to a regular pediatric nursing floor. Physical therapy, occupational therapy and speech therapy will be consulted based on the child’s needs. An average hospital stay slightly varies between patient to patient and usually ranges from 5 to 7 days. Length of stay decisions are made by the surgical team and are based on the child’s condition and recovery.
What happens after being discharged from hemispherectomy?
Upon discharge, rehabilitation services are often required to enhance recovery from a hemispherectomy. If medically indicated, the child may be transferred to a rehab facility for intensive physical, occupational and speech therapy. This is usually followed by home or outpatient services. If inpatient rehabilitation is not required, home or outpatient therapy visits are often indicated. Outpatient therapy can be provided through hospitals and free-standing facilities and schools. Parents should check with individual school systems to see if this is a service provided.
References [ + ]





{kind=link}