
Contents
Hearing loss in children
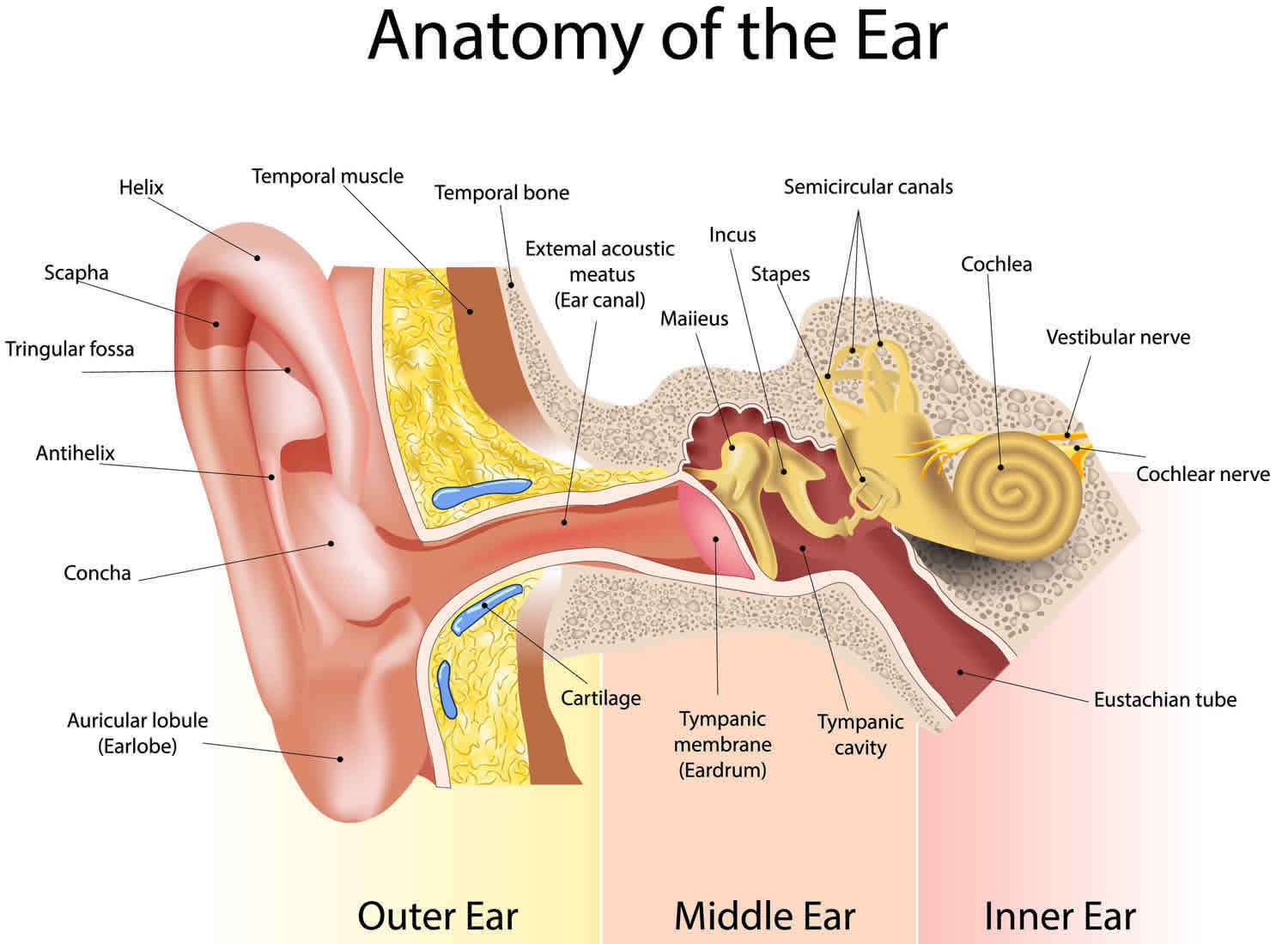
A hearing loss can happen when any part of the ear is not working in the usual way (Figure 1 below). This includes the outer ear, middle ear, inner ear, hearing (acoustic) nerve, and auditory system. As hearing is important for language development, early detection and treatment of any hearing loss is important. In the first few years of life, hearing is a critical part of kids’ social, emotional, and cognitive development. Hearing loss can affect a child’s ability to develop speech, language, and social skills. Even a mild or partial hearing loss can affect a child’s ability to develop speech and language properly. The earlier children with hearing loss start getting services, the more likely they are to reach their full potential. If you think that a child might have hearing loss, trust your instincts and ask the child’s doctor for a hearing screening as soon as possible.
Having a hearing loss (impairment) means that a child has lost some hearing in one or both ears. Hearing loss may be partial – a child can’t hear certain sounds – or it can be complete. It may be temporary or permanent, and caused by a wide range of possible factors.
There are many types and degrees of hearing loss, and they are described according to how much hearing has been lost and which part of the ear is affected. Hearing loss is also explained as mild, moderate, moderate to severe, severe or profound. Hearing is measured in decibels (dB) and the severity of the hearing loss is graded by hearing thresholds. The normal hearing range is 0-20 decibels (dB) which equates to being able to perceive sound quieter than a whisper. Mild hearing loss corresponds to a range of 20-39 dB (a person with a mild hearing loss may hear some speech sounds but soft sounds are hard to hear), moderate 40-69 dB (a person with a moderate hearing loss may hear almost no speech when another person is talking at a normal level), severe 70-89 dB (a person with severe hearing loss will hear no speech when a person is talking at a normal level and only some loud sounds) and profound is greater than 90 dB (a person with a profound hearing loss will not hear any speech and only very loud sound).
Table 1. The table below shows a common way to classify hearing loss
| Degree of hearing loss | Hearing loss range (dB) |
|---|---|
| Normal | –10 to 15 |
| Slight | 16 to 25 |
| Mild | 26 to 40 |
| Moderate | 41 to 55 |
| Moderately severe | 56 to 70 |
| Severe | 71 to 90 |
| Profound | 91+ |
Hearing loss occurs in 1-3 newborns per 1000 births 2), with 1-2 per 1,000 suffering from permanent childhood hearing impairment 3). There is a slightly increased prevalence of hearing loss in boys compared to girls with a ratio of 1.16:1.0 4).
There are 2 main types of hearing impairment: ‘conductive’ and ‘sensorineural’. Having both types is called a ‘mixed loss’.
- Conductive hearing loss occurs when something interferes with sound waves travelling through the outer and middle parts of the ear to the inner ear. It can be caused by a wax blockage, middle ear infection (otitis media), a fluid build-up in the middle ear, or damage to the tiny bones in the middle ear. Conductive hearing loss may be either temporary or permanent.
- Sensorineural hearing loss is caused by a problem in the innermost part of the ear or in the nerve which carries hearing, the ‘auditory nerve’. It can be caused by abnormal inner ear development, a physical injury to the inner ear, damage to the ear from diseases such as meningitis and rubella, or a tumor. Despite being relatively uncommon in children as a whole, it is the primary cause of permanent hearing loss in the pediatric population. Sensorineural hearing losses are usually permanent. Sometimes the problem with the inner ear also causes problems with balance. Children with both hearing and balance problems may have delayed development of their motor skills.
- Mixed hearing loss occurs when there are both conductive and sensorineural components.
Ear anatomy
A hearing loss can happen when any part of the ear or auditory (hearing) system is not working in the usual way.
Outer Ear
The outer ear is made up of:
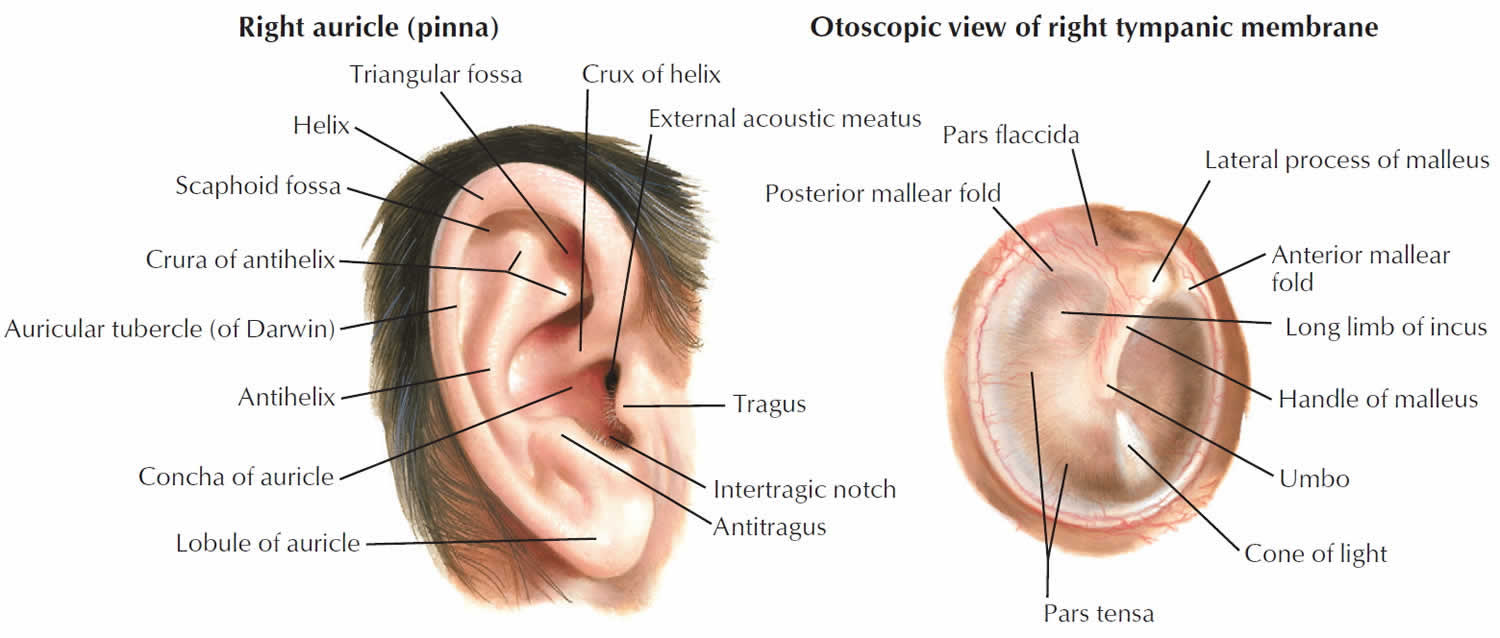
- the part we see on the sides of our heads, known as pinna
- the ear canal
- the eardrum, sometimes called the tympanic membrane, which separates the outer and middle ear
Middle Ear
The middle ear is made up of:
- the eardrum
- three small bones called ossicles that send the movement of the eardrum to the inner ear
Inner Ear
The inner ear is made up of:
- the snail shaped organ for hearing known as the cochlea
- the semicircular canals that help with balance
- the nerves that go to the brain
Auditory (ear) Nerve
This nerve sends sound information from the ear to the brain.
Auditory (Hearing) System
The auditory pathway processes sound information as it travels from the ear to the brain so that our brain pathways are part of our hearing.
Figure 1. Ear anatomy
Types of hearing loss
There are four types of hearing loss:
- Conductive hearing loss: Hearing loss caused by something that stops sounds from getting through the outer or middle ear. This type of hearing loss can often be treated with medicine or surgery.
- Sensorineural hearing loss: Hearing loss that occurs when there is a problem in the way the inner ear or hearing nerve works.
- Mixed hearing loss: Hearing loss that includes both a conductive and a sensorineural hearing loss.
- Auditory Neuropathy Spectrum Disorder: Hearing loss that occurs when sound enters the ear normally, but because of damage to the inner ear or the hearing nerve, sound isn’t organized in a way that the brain can understand.
Hearing loss can also be described as:
- Unilateral or Bilateral: Hearing loss is in one ear (unilateral) or both ears (bilateral).
- Pre-lingual or Post-lingual: Hearing loss happened before a person learned to talk (pre-lingual) or after a person learned to talk (post-lingual)
- Symmetrical or Asymmetrical: Hearing loss is the same in both ears (symmetrical) or is different in each ear (asymmetrical).
- Progressive or Sudden: Hearing loss worsens over time (progressive) or happens quickly (sudden).
- Fluctuating or Stable: Hearing loss gets either better or worse over time (fluctuating) or stays the same over time (stable).
- Congenital or Acquired/Delayed Onset: Hearing loss is present at birth (congenital) or appears sometime later in life (acquired or delayed onset).
Hearing loss in children causes
Hearing loss can be broadly characterized as congenital or acquired in the pediatric population.
Congenital causes
Congenital hearing loss can be classified as genetic and non-genetic in origin. Genetic cause of hearing loss is responsible for 50% to 60% of congenital causes and can be due to either an autosomal dominant, recessive or sex-linked mutation 5). Genetic causes are often further subdivided into syndromic versus non-syndromic categories based on whether the patient suffers from an underlying genetic syndrome. About 70% of all mutations causing hearing loss are non-syndromic. This means that the person does not have any other symptoms. About 30% of the mutations causing hearing loss are syndromic. This means that the person has other symptoms besides hearing loss. For example, some people with hearing loss are also blind 6). The most common cause of congenital hearing loss is autosomal recessive non-syndromic hearing loss.
There are also a number of things in the environment that can cause hearing loss. 25% or more of hearing loss in babies is due to “environmental” causes such as maternal infections during pregnancy and complications after birth. Sometimes both genes and environment work together to cause hearing loss. For example, there are some medicines that can cause hearing loss, but only in people who have certain mutations in their genes.
Genes contain the instructions that tell the cells of people’s bodies how to grow and work. For example, the instructions in genes control what color a person’s eyes will be. There are many genes that are involved in hearing. Sometimes, a gene does not form in the expected manner. This is called a mutation. Some mutations run in families and others do not. If more than one person in a family has hearing loss, it is said to be “familial”. That is, it runs in the family.
The cochlea (the part of the ear that changes sounds in the air into nerve signals to the brain) is a very complex and specialized part of the body that needs many instructions to guide its development and function. These instructions come from genes. Changes in any one of these genes can result in hearing loss. The GJB2 gene is one of the genes that contains the instructions for a protein called connexin 26; this protein plays an important role in the functioning of the cochlea. In some populations about 40% of newborns with a genetic hearing loss who do not have a syndrome, have a mutation in the GJB2 gene.
TORCH organisms (toxoplasmosis, rubella, cytomegalovirus [CMV] and herpes) have been identified as key infective causative agents. Cytomegalovirus (CMV) is the most common cause of congenital non-genetic hearing loss in the developed world 7). Other congenital causes include trauma, ototoxic medications used in the antenatal period and several perinatal risk factors such as prematurity, low birth weight, and hyperbilirubinemia.
Acquired hearing loss
Otitis media with effusion is the number one cause of acquired hearing loss in children. It is beyond the scope of this article to cover this in detail, but it classically has a bimodal beak at 2 years and 5 years of age and is characterized by a conductive hearing loss associated with flattened tympanogram 8). It typically resolves without intervention as the eustachian tube matures or following the insertion of a ventilation tube in the middle ear 9). Adenoidal hypertrophy can contribute to this clinical picture 10). Infections also present another major category for acquired hearing loss, with a particularly strong link with bacterial meningitis, mumps, and measles. Other reasons include primary otological pathologies such as cholesteatoma, impacted wax and otosclerosis as well as trauma.
High-risk factors in neonates:
- Congenital infections
- Family history
- Craniofacial anomalies
- Hyperbilirubinemia
- Birth weight 1500 g
- Low Apgar score
- Bacterial meningitis
- Prolonged intubation.
Risk factors for hearing problems in children
Hearing loss can happen any time during life – from before birth to adulthood.
Following are some of the things that can increase the chance that a child will have hearing loss:
- A genetic cause: About 1 out of 2 cases of hearing loss in babies is due to genetic causes. Some babies with a genetic cause for their hearing loss might have family members who also have a hearing loss. About 1 out of 3 babies with genetic hearing loss have a “syndrome.” This means they have other conditions in addition to the hearing loss, such as Down syndrome or Usher syndrome.
- 1 out of 4 cases of hearing loss in babies is due to maternal infections during pregnancy, complications after birth, and head trauma. For example, the child:
- Was exposed to infection, such as , before birth
- Spent 5 days or more in a hospital neonatal intensive care unit (NICU) or had complications while in the NICU
- Needed a special procedure like a blood transfusion to treat bad jaundice
- Has head, face or ears shaped or formed in a different way than usual
- Has a condition like a neurological disorder that may be associated with hearing loss
- Had an infection around the brain and spinal cord called meningitis
- Received a bad injury to the head that required a hospital stay
- For about 1 out of 4 babies born with hearing loss, the cause is unknown.
Hearing loss in children prevention
Following are tips for parents to help prevent hearing loss in their children:
- Have a healthy pregnancy.
- Make sure your child gets all the regular childhood vaccines.
- Keep your child away from high noise levels, such as from very loud toys.
- If you think that your child might have hearing loss, ask your child’s doctor for a hearing screening as soon as possible. Don’t wait!
- If your child does not pass a hearing screening, ask your child’s doctor for a full hearing test as soon as possible.
- If your child has hearing loss, talk to your child’s doctor about treatment and intervention services.
Remember, hearing loss can affect a child’s ability to develop speech, language, and social skills. The earlier children with hearing loss start getting services, the more likely they are to reach their full potential. If you are a parent and you suspect your child has hearing loss, trust your instincts and speak with your child’s doctor.
Dangerous and safe noise levels
The noise chart below lists average decibel levels for everyday sounds around you.
Painful impulse noise—Not safe for any period of time
- 150 dBP = fireworks at 3 feet, firecracker, shotgun
- 140 dBP = firearms
Painful steady noise—Not safe for any period of time
- 130 dBA = jackhammer
- 120 dBA = jet plane takeoff, siren, pneumatic drill
Extremely loud—Dangerous to hearing; wear earplugs or earmuffs
- 112 dBA = maximum output of some MP3 players, rock concert, chainsaw
- 106 dBA = gas leaf blower, snow blower
- 100 dBA = tractor, listening with earphones
- 94 dBA = hair dryer, kitchen blender, food processor
Very loud—Dangerous to hearing; wear earplugs or earmuffs
- 91 dBA = subway, passing motorcycle, gas mower
Moderate—Safe listening for any time period
- 70 dBA = group conversation, vacuum cleaner, alarm clock
- 60 dBA = typical conversation, dishwasher, clothes dryer
- 50 dBA = moderate rainfall
- 40 dBA = quiet room
Faint—Safe listening for any time period
- 30 dBA = whisper, quiet library
Hearing loss in children signs and symptoms
The signs and symptoms of hearing loss are different for each child. If you think that your child might have hearing loss, ask the child’s doctor for a hearing screening as soon as possible. Don’t wait!
Even if a child has passed a hearing screening before, it is important to look out for the following signs.
Things to look out for, as they can be signs of possible hearing loss are:
- loud noises do not startle your child by 4 months of age, or your child does not turn towards the source of a sound
- your child notices you only when they see you
- your child does not make sounds other than gargles and other vibrating noises that they can feel
- speech development is delayed
- your child seems to not hear when called or doesn’t respond to their name or say simple words by 14 months
- your child can’t follow simple instructions by 24 months
- your child hears some sounds but not others
- your child has trouble holding their head steady, or is slow to sit up by themselves or walk
Signs in babies
- Does not startle at loud noises.
- Does not turn to the source of a sound after 6 months of age.
- Does not say single words, such as “dada” or “mama” by 1 year of age.
- Turns head when he or she sees you but not if you only call out his or her name. This sometimes is mistaken for not paying attention or just ignoring, but could be the result of a partial or complete hearing loss.
- Seems to hear some sounds but not others.
As a guide, here’s what you’d expect in a typically developing baby:
- At 0-4 months, your baby should startle at a loud noise, turn her head or move her eyes to locate the source of the sound. If she’s upset, she should calm down when she hears your voice.
- At 4-8 months, your baby should notice sounds around him, smile when spoken to, babble and understand simple words like ‘bye-bye’.
- At 8-14 months, your baby should respond to her name, say simple words like ‘mama’ and ‘dada’, copy simple sounds and use her voice to get attention from people nearby.
- At 14-24 months, your child will start to develop vocabulary, understand and follow simple instructions, and put two words together.
If your child isn’t doing these things, it might be a good idea to talk to your child’s doctor. Even if everything seems OK but you still feel worried, you should see your doctor. After all, you know your baby best.
Signs in children
- Speech is delayed.
- Speech is not clear.
- Does not follow directions. This sometimes is mistaken for not paying attention or just ignoring, but could be the result of a partial or complete hearing loss.
- Often says, “Huh?”
- Turns the TV volume up too high.
Babies and children should reach milestones in how they play, learn, communicate and act. A delay in any of these milestones could be a sign of hearing loss or other developmental problem.
Hearing loss in children diagnosis
Hearing loss can present in different ways depending on the age of the child. Hearing loss in neonates is almost exclusively picked up via newborn screening programme assessments. In older children, parents or other professionals such as school teachers, may notice delayed language skills, behavioral problems or listening to the television at raised volumes. In the history, it is important to ascertain whether there are any associated otological symptoms such as otorrhoea, otalgia, tinnitus, or vertigo. A thorough history is required including asking about any other neurological symptoms, medical history including drug history and precipitating events such as trauma, recent viral infections or new medications.
The examination will involve assessing the ear including the appearance of the pinna particularly inspecting for any deformities such as microtia or anotia. Otoscopic examination of the external auditory canal and tympanic membrane is crucial, with special attention on the attic for cholesteatoma. An examination should also include assessment of cranial nerves, a full neurological assessment, and assessment of balance depending on the age of the child.
With the implementation of Universal Newborn Hearing Screening program, today most patiets are identified within a few months after birth, with intervention started by 6 months.
Babies usually have their hearing tested in the first few weeks of life. Most newborns are tested before they leave hospital to help identify those who might require further hearing and middle ear function testing.
Babies with possible hearing loss are referred to a hearing specialist (audiologist) who will do more specialized testing to diagnose the type and extent of hearing loss. Understanding the cause helps determine the best treatment.
Hearing screening
Hearing screening can tell if a child might have hearing loss. Hearing screening is easy and is not painful. In fact, babies are often asleep while being screened. It takes a very short time — usually only a few minutes.
- Babies: All babies should have a hearing screening no later than 1 month of age. Most babies have their hearing screened while still in the hospital. If a baby does not pass a hearing screening, it’s very important to get a full hearing test as soon as possible, but no later than 3 months of age.
- Children: Children should have their hearing tested before they enter school or any time there is a concern about the child’s hearing. Children who are at risk for acquired, progressive, or delayed-onset hearing loss should have at least one hearing test by 2 to 2 1/2 years of age. Hearing loss that gets worse over time is known as acquired or progressive hearing loss. Hearing loss that develops after the baby is born is called delayed-onset hearing loss. Find out if a child may be at risk for hearing loss. Children who do not pass the hearing screening need to get a full hearing test as soon as possible.
Full hearing test
All children who do not pass a hearing screening should have a full hearing test. This test is also called an audiology evaluation. An audiologist, who is an expert trained to test hearing, will do the full hearing test. In addition, the audiologist will also ask questions about birth history, ear infection and hearing loss in the family.
There are many kinds of tests an audiologist can do to find out if a person has a hearing loss, how much of a hearing loss there is, and what type it is. The hearing tests are easy and not painful.
Hearing assessment in children is age and ability dependent and some of the tests the audiologist might use include 11):
- Auditory Brainstem Response (ABR) Test or Brainstem Auditory Evoked Response (BAER) Test: Auditory Brainstem Response (ABR) or Brainstem Auditory Evoked Response (BAER) is a test that checks the brain’s response to sound. Because this test does not rely on a person’s response behavior, the person being tested can be sound asleep during the test.
- Otoacoustic Emissions (OAE): Otoacoustic Emissions (OAE) is a test that checks the inner ear response to sound. Because this test does not rely on a person’s response behavior, the person being tested can be sound asleep during the test.
- Behavioral Audiometry Evaluation: Behavioral Audiometry Evaluation will test how a person responds to sound overall. Behavioral Audiometry Evaluation tests the function of all parts of the ear. The person being tested must be awake and actively respond to sounds heard during the test.
With the parents’ permission, the audiologist will share the results with the child’s primary care doctor and other experts, such as:
- An ear, nose and throat (ENT) doctor, also called an otolaryngologist
- An eye doctor, also called an ophthalmologist
- A professional trained in genetics, also called a clinical geneticist or a genetics counselor
Neonates
Otoacoustic emissions
All newborns and those who require less than 48 hours of special care in neonatal intensive care (NICU), are offered evoked otoacoustic emission testing within the first 4-5 weeks of birth as part of a Newborn Hearing Screening Program 12). Oto-acoustic emissions are outer hair vibrations that are detected in the external auditory canal in response to a click stimulus. This test is easy to perform and does not involve a general anesthetic.
Automated Auditory Brainstem Response (ABR)
This investigation is offered to all newborns who have spent over 48 hours in the neonatal intensive NICU and is also offered to those who do not pass two otoacoustic emission tests 13). It involves measuring brainstem electrophysiological responses to click stimuli using electrodes placed on the scalp. This assesses hearing throughout the entire hearing pathway; form the external ear through to the brainstem.
6-8 months
Distraction techniques
An assistant engages the child’s attention, and the tester, whilst placed behind and to the side of the child, makes sounds of different intensities. The child is assessed to see whether they turn to the side of the noise.
9 – 36 months
Visual Reinforcement Audiometry
The child is placed at a table with some toys with two speakers either side that produce sounds. If the child looks towards the speaker playing a sound they are delivered a visual reinforcement (such as a flashing light) 14).
24-60 months
Conditioned Play Audiometry
The child is conditioned to perform a task in response to an auditory stimulus such as placing a ball in a cup. Once the task is learned the sound volume is reduced in order to determine their hearing threshold.
Over 60 months
Pure Tone Audiometry
A 5 years of age most children can undergo pure tone audiometry. Hearing thresholds are determined by presenting sounds of various frequencies and at various intensities until the quietest sound is reliably detected 50% of the time. This test requires a higher level of attention and therefore is rarely done below the age of 5 years.
Other investigations
Additional investigations will be tailored to the precise clinical picture. In syndromic children, chromosomal testing is advised. There is also a role for imaging in the form of either computed tomography (CT) or magnetic resonance imaging (MRI)
Some authors advocate measurement of renal function and testing for connexin-26, which is a marker who sensorineural hearing loss. In some children, imaging studies may prove useful and detect abnormalities of the cochlea or the cochlear nerve. Finally, ECG may be useful in children with Jervell Lange Nelsen syndrome. The ECG will reveal a prolonged QT interval, which can lead to syncopal attacks and death.
Hearing loss in children treatment
Treatment for hearing loss depends on the type of hearing loss present, the underlying cause and often there is an element of patient/parent preference. Conductive hearing loss due to otitis media is treated with antibiotics. Some children may benefit from a myringotomy tube. Sensorineural loss cannot be treated with medical measures. Mild cases may be treated with amplifcation aids and speech therapy is useful. However, amplifcation of sound can result in ear pain and discomfort.
Treatment of hearing loss depends on its cause and severity but can include:
- medication, such as antibiotics for ear infections
- repeated ear infections may sometimes be treated with grommets
- removal of a foreign object or wax
- surgery, such as inserting tubes to help fluid drain out of the ears
- hearing aids, or other technology to amplify sounds or assist hearing
- a cochlear implant for severe or profound hearing loss
- speech therapy
- assistance from a specialist teacher of the deaf to help make the most of any residual hearing
The earlier that hearing loss is identified and treated, the better for a child’s language, learning and overall development.
The most important thing for your child’s development is being able to communicate. A range of options are available, including spoken language, sign language or a combination of sign and spoken language to talk.
Children with hearing loss need regular hearing, ear and eye examinations. Younger children need to be tested very regularly because their ear canals are growing and changing shape. Regular eye exams are important because your child’s main way to learn and communicate is through sight.
Conservative management
A key element to managing hearing loss is family support and advice. There are a number of behavioral measures that can be used to improve hearing without the need for adjuncts or surgical intervention. The principles of this are rooted in creating a deaf-friendly environment such as limiting background noise, talking face-on, and clear intonation. There are also a range of hearing assist devices that can be used such as television listeners. It is also crucial that the child educational support which could be in the form of special equipment or positioning in the classroom.
Hearing aids
There are a variety of hearing aid types that are used in specific situations.
Binaural air conduction hearing aids rely on at least a partially functioning inner ear and central auditory processing system. They work by converting sound detected by a microphone into digital signals which can then be amplified and re-converted into audible sounds that are transmitted to the ear. They can be classified based on whether these key parts are housed in an earpiece that sits externally (behind-the-ear), inside the canal (in-the-canal) or further inside the canal (in-the-ear).
Bone conduction hearing aids are used typically in a conductive hearing loss when there are ear problems that impede the use of a regular air conduction hearing aid such in children with external ear deformities (anotia, microtia) or when there are chronic ear infections. Bone-anchored hearing aids (BAHA) are fitted surgically under general anesthetic over two stages. A titanium implant is fixed into the temporal bone. Through this setup, a sound is conducted directly to the inner ear by way of the bone, bypassing the middle ear. Typically the BAHA is fitting from 4 years of age once the temporal bone has developed, however, soft-band bone conducting aids can be used from several weeks of age.
Contralateral routing of sound (CROS) hearing aids are used when there is a unilateral sensorineural hearing loss. The sound in the problem ear is diverted to the better hearing ear without amplification. In cases where neither ear has normal hearing but one side is significantly better, a variation on this can be used called a BiCROS.
Cochlear implant
Cochlear implants work by converting sound into digital signals that are transmitted directly to the auditory nerve via an electrode array. The National Institue of Clinical Excellence (NICE) recommends cochlear implants in children who have severe to profound deafness in one or two ears with minimal benefit from conventional hearing aids after 3 months of use 15).
Intervention services
No single treatment or intervention is the answer for every child or family. Good intervention plans will include close monitoring, follow-ups and any changes needed along the way. There are many different options for children with hearing loss and their families.
Some of the treatment and intervention options include:
- Working with a professional (or team) who can help a child and family learn to communicate.
- Getting a hearing device, such as a hearing aid.
- Joining support groups.
- Taking advantage of other resources available to children with a hearing loss and their families.
Early intervention and special education
Early Intervention (0-3 years)
Hearing loss can affect a child’s ability to develop speech, language, and social skills. The earlier a child who is deaf or hard-of-hearing starts getting services, the more likely the child’s speech, language, and social skills will reach their full potential.
Early intervention program services help young children with hearing loss learn language skills and other important skills. Research shows that early intervention services can greatly improve a child’s development.
Babies that are diagnosed with hearing loss should begin to get intervention services as soon as possible, but no later than 6 months of age.
There are many services available through the Individuals with Disabilities Education Improvement Act 2004 (https://sites.ed.gov/idea). Services for children from birth through 36 months of age are called Early Intervention or Part C services. Even if your child has not been diagnosed with a hearing loss, he or she may be eligible for early intervention treatment services. The Disabilities Education Improvement Act 2004 says that children under the age of 3 years (36 months) who are at risk of having developmental delays may be eligible for services. These services are provided through an early intervention system in your state. Through this system, you can ask for an evaluation.
Special Education (3-22 years)
Special education is instruction specifically designed to address the educational and related developmental needs of older children with disabilities, or those who are experiencing developmental delays. Services for these children are provided through the public school system. These services are available through the Individuals with Disabilities Education Improvement Act 2004 (IDEA 2004), Part B.
Early Hearing Detection and Intervention Program
Every state has an Early Hearing Detection and Intervention (EHDI) program. Early Hearing Detection and Intervention works to identify infants and children with hearing loss. Early Hearing Detection and Intervention also promotes timely follow-up testing and services or interventions for any family whose child has a hearing loss. If your child has a hearing loss or if you have any concerns about your child’s hearing, contact your local Early Hearing Detection and Intervention Program (http://www.infanthearing.org/status/cnhs.php) to find available services in your state.
Other options
Ventilation tubes are indicated in conductive hearing loss secondary to flue ear, or less frequently in the context of recurrent otitis media. They are inserted surgically and typically self-extrude on average a year of insertion. Children found to have cholesteatoma invariably require surgical clearance of disease via a mastoidectomy.
Other assistive devices
Besides hearing aids, there are other devices that help people with hearing loss. Following are some examples of other assistive devices:
- Frequency modulated (FM) system: An FM system is a kind of device that helps people with hearing loss hear in background noise. FM stands for frequency modulation. It is the same type of signal used for radios. FM systems send sound from a microphone used by someone speaking to a person wearing the receiver. This system is sometimes used with hearing aids. An extra piece is attached to the hearing aid that works with the FM system.
- Captioning: Many television programs, videos, and DVDs are captioned. Television sets made after 1993 are made to show the captioning. You don’t have to buy anything special. Captions show the conversation spoken in soundtrack of a program on the bottom of the television screen.
There are many other devices available for children with hearing loss. Some of these include:
- Text messaging
- Telephone amplifiers
- Flashing and vibrating alarms
- Audio loop systems
- Infrared listening devices
- Portable sound amplifiers
- TTY (Text Telephone or teletypewriter)
Hearing loss in children prognosis
Prognosis of hearing loss will vary considerably based on the underlying aetiology. Congenital sensorineural hearing loss left untreated will invariably not improve or can progress, such as in the case of congenital cytomegalovirus (CMV). On the other side of the spectrum, glue ear shows an excellent prognosis with resolution of symptoms even without intervention 16).
References [ + ]





{kind=link}