
Contents
Glue ear
Glue ear also called otitis media with effusion, is a build-up of sticky fluid (or glue) in your middle ear that can cause problems with hearing. This can cause temporary hearing loss. Glue ear is common in children. It usually clears up within 3 months and then gets better on its own without treatment, but see a doctor about any hearing problems. If glue ear hasn’t clear up within 3 months, and you or your child develops severe hearing problems, then an operation may help.
Glue ear can affect hearing because the middle ear can’t move freely, but the level of hearing loss is mild. Some children have recurrent glue ear, meaning it returns after treatment over a long period. Because of the hearing problems that come with glue ear, this can cause speech and language development problems.
Around eight out of 10 children have glue ear at least once by the time they reach the age of 10. Glue ear tends to affect children under the age of seven and your child is most likely to get it between the ages of two and five. They’re more likely to get it during the winter months and it often comes and goes.
Some children develop glue ear after a cold, so it can be more common during the winter months. It’s also more common in boys than girls, but scientists don’t know why yet.
When the tube between your middle ear and the back of your throat, the Eustachian tube, becomes blocked, air can’t get in and it starts to fill with fluid. This makes it harder for sounds to pass through the middle ear to the inner ear, which is what affects your child’s hearing.
Glue ear usually gets better over a few months and most children will no longer have it after a year. For a few children it carries on longer and can cause hearing loss, which can affect their education, language development and behavior.
There are lots of things you can do to help your child. If you smoke, then your child is more likely to develop glue ear so now is a good time to stop or to smoke outside, well away from your children.
See a doctor if you or your child are having hearing problems.
Your child may be struggling to hear if they often:
- speak more loudly or quietly than usual
- are difficult to understand
- ask people to repeat what they say
- ask for the TV or music to be turned up loud
- struggle to hear people far away
- become easily distracted when people are talking
- seem tired and irritable because it’s harder to listen
How do you hear?
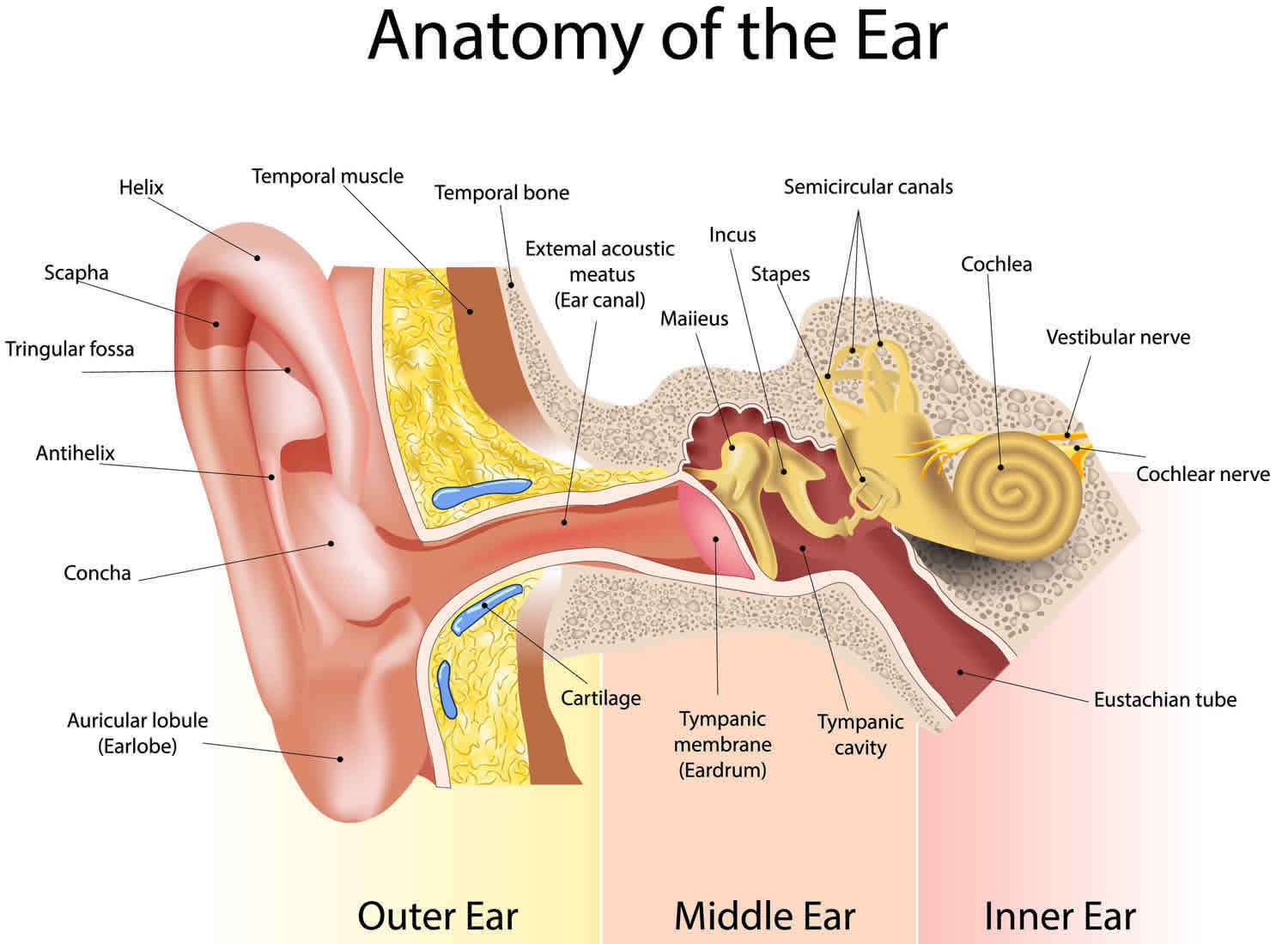
The ear consists of three parts, the outer ear, the middle ear and the inner ear. Sound waves enter the ear canal and cause the eardrum to vibrate. The sound then passes through the middle ear through the three small bones of hearing (ossicles) on to the inner ear, which is filled with fluid.
The movement of the fluid in the cochlea stimulates the hair cells inside it to trigger a nerve impulse, which is carried to the brain by the auditory nerve. The brain then interprets these nerve impulses as sound.
Figure 1. Ear anatomy
Glue ear in adults
Adults can get glue ear, though it’s much less common than in children. Treatment is generally the same as for children. You’re likely to notice some hearing loss, but may also hear popping sounds.
If you think you may have glue ear as an adult, get it checked out by your doctor.
What are grommets?
Grommets are tiny tubes inserted into the eardrum. They allow air to pass through the eardrum, keeping the air pressure on either side equal. The surgeon makes a tiny hole in the eardrum and inserts the grommet into the hole. It usually stays in place for six to 12 months and then falls out. This is normal and won’t affect your child.
What care should I take with grommets?
Your surgeon is likely to ask you to keep your child’s ears dry for a few weeks after the operation. This helps to stop water getting into the ear and causing an infection while it’s healing.
You’ll be asked to take care when bathing, showering or washing your child’s hair. You’ll also be asked not to take your child swimming.
Surgeons give different advice about how long you’ll need to do this, so ask for information. After the first few weeks, there’s no evidence that wearing earplugs or not swimming or bathing will make any difference to the likelihood of getting an infection.
My child has glue ear and we’re going on holiday, will we be able to fly?
It’s usually OK to fly if your child has glue ear. However, if your child has an ear infection it can sometimes cause problems.
As an airplane takes off, the air pressure in the cabin drops and that causes gases to expand. As the airplane comes down to land, the air pressure increases and gases contract. These changes affect the air in your middle ear and if your child has a middle ear infection, it can be painful and can cause injury. It’s a good idea to check with your doctor before your child travels. They may prescribe decongestant nose drops to use before take-off and landing.
Glue ear causes
Doctors aren’t completely sure why glue ear happens. Different factors are involved, but in more than a half of children glue ear follows an infection of the middle ear.
Other possible causes include:
- problems with the Eustachian tube – the tube between the middle ear and the back of the throat
- an infection (a virus or bacteria)
- inflamed middle ear
- infected adenoids
Your child is more likely to get glue ear if they:
- live with someone who smokes
- have repeated colds and throat infections
- have allergies
- are fed from a bottle when lying down
- have contact with lots of children, such as at a nursery, or have older siblings
- have a cleft palate or Down’s syndrome
Glue ear symptoms
The most common symptom of glue ear is temporary hearing loss. It can affect both ears at the same time. But sometimes the symptoms of glue ear can be hard to spot, especially if your child is very young.
Other symptoms may include:
- earache or ear pain
- hearing sounds like ringing or buzzing (tinnitus)
Glue ear is much more common in children, but adults with glue ear have the same symptoms.
You might see this as some of the following behavior in kids.
- Mishearing what you say.
- Not responding when you talk to them, especially from behind.
- Having the television volume up high.
- Having trouble concentrating.
- Preferring to play on their own, rather than in a group.
- Becoming tired.
- A change in behavior.
Other symptoms include feeling like the inside of the ear is blocked, mild ear pain and hearing ‘popping’ in the ear. Some children have repeated ear infections, coughs and colds before they get glue ear.
If hearing loss is severe, or it’s been a symptom for a while, your child may have problems with speech and language. Their listening skills can also be affected and these things together can affect their progress at nursery or school.
Glue ear diagnosis
Your doctor will ask about your child’s symptoms and medical history. Your doctor can usually diagnose glue ear by looking for fluid inside your or your child’s ear and eardrum.
They’ll use a small scope with a magnifying glass and a light called the otoscope. This should not be painful.
If your child has had glue ear for more than 3 months, they may be referred to a specialist for hearing tests. There are two main types of hearing test. Tympanometry assesses how well their eardrum reacts to sound and audiometry tests their hearing. The type of test your child has will depend on how old they are and their stage of development.
Hearing tests can help find out how severe any hearing loss is and what’s causing it.
Your doctor may monitor your child for three months and then order another hearing test.
If after three months your child’s symptoms haven’t got any better, your doctor may refer them to an ear, nose and throat (ENT) specialist. If your child has Down’s syndrome or a cleft palate, they’re likely to be referred to a specialist straightaway.
Glue ear treatment
Non-surgical treatments
Glue ear is not always treated. Your doctor will usually wait and see if the symptoms get better on their own. This is because there’s no effective medicine for glue ear, and it often clears up on its own within 3 months.
They may still monitor your child for up to a year in case the symptoms change or get worse.
Your doctor may suggest trying a treatment called autoinflation, while waiting for symptoms to improve. Autoinflation helps to open the Eustachian tube to let air into the middle ear so fluid in the middle ear can drain out.
Autoinflation is done by either:
- blowing up a special balloon using one nostril at a time
- swallowing while holding the nostrils closed
As autoinflation has to be done several times a day, it’s not usually recommended for children under 3 years old.
Your child may need to wear hearing aids if they have hearing loss in both ears and surgery isn’t an option. Wearing a hearing aid can make some children anxious, so your doctor will talk to you about your choices.
If glue ear causes an ear infection, your doctor may prescribe antibiotics.
Antihistamines, steroids and decongestants don’t work as treatments for glue ear. There is also no evidence that complementary therapies such as homeopathy or special diets will help.
Nasal balloon instructions
The nasal balloon comes in a treatment pack (Otovent) containing 5 medical balloons, a connecting nozzle and a small carrying case.
Watch videos demonstration of nasal balloon autoinflation.
Step by step instructions:
- Take one of the balloons and stretch it using your hands or blow it up with your mouth to release some of the tension, otherwise the first inflation may be quite difficult.
- Attach the balloon to the connecting nozzle.
- To make sure your child understands what they need to do either show them the instruction video or demonstrate the nasal balloon yourself.
- Ask your child to hold the nozzle up to one nostril and close off the other nostril with their fingers.
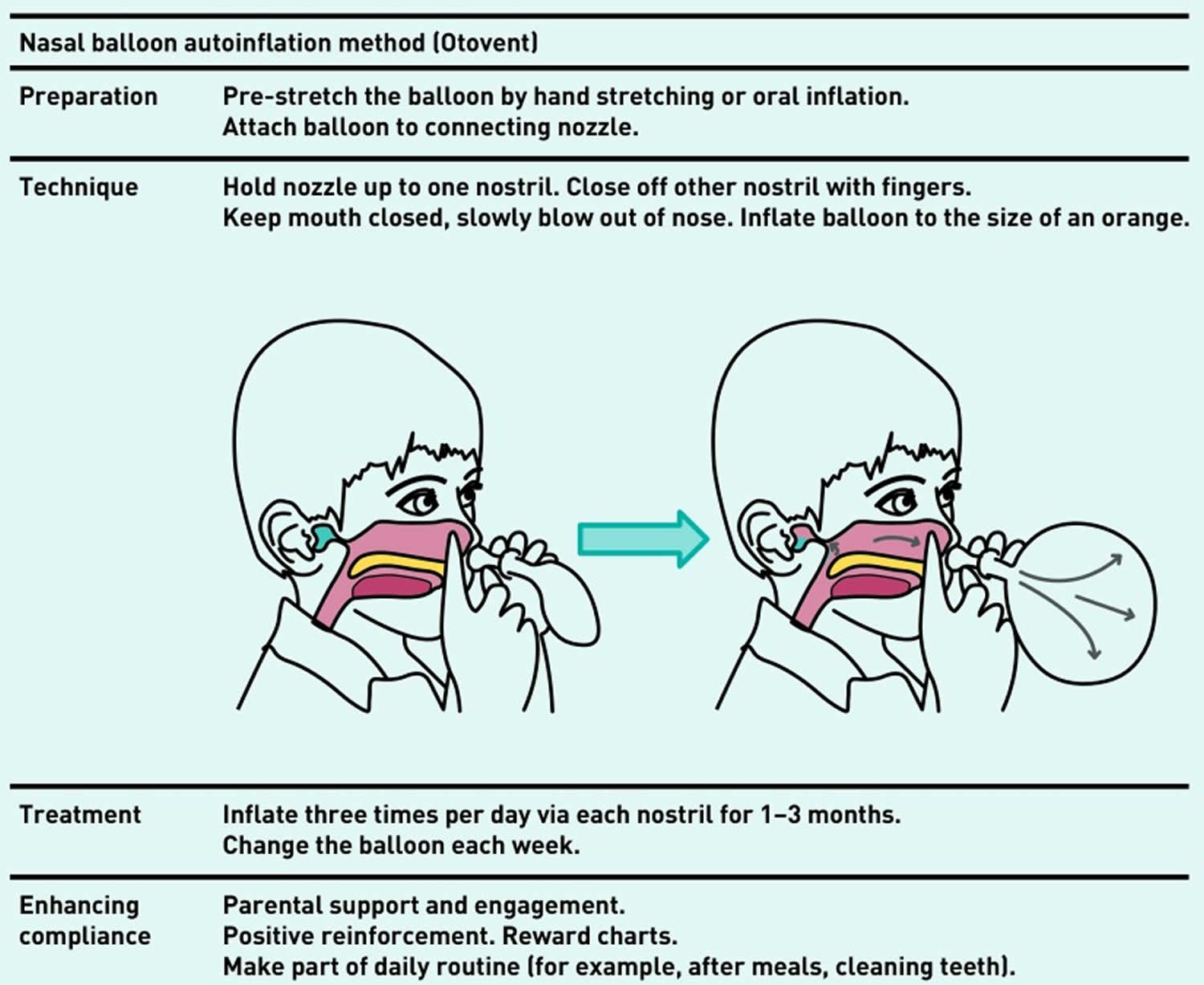
- Instruct your child to keep their mouth closed, slowly blow out of the nose and inflate the balloon to about the size of a large orange. Repeat with the other nostril.
- Give lots of feedback and encouragement. Using a sticker chart can help you and your child to remember to use the balloon regularly
Figure 2. Nasal balloon autoinflation method
Surgery for glue ear
Your child may be referred to a specialist in hospital if:
- glue ear symptoms are affecting their learning and development
- they already had severe hearing loss before glue ear
- they have been diagnosed with Down’s syndrome or a cleft lip and palate, as glue ear is less likely to get better by itself
Your doctor may suggest surgery if the glue ear is no better after three months and your child has severe hearing loss. Surgery is also an option if your child’s learning or development is affected.
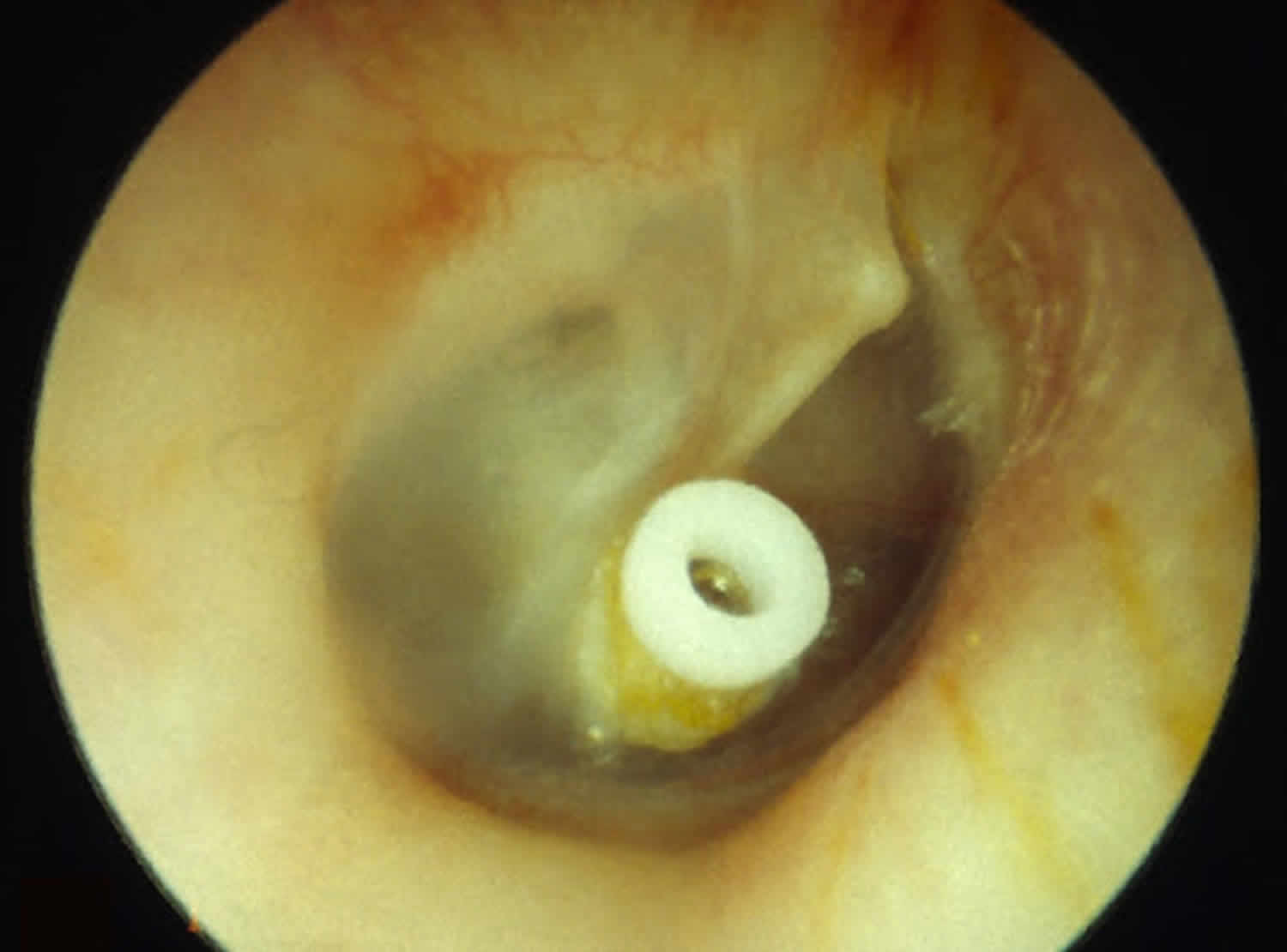
The main surgery for glue ear is to make a tiny cut in the ear drum and put in a plastic tube called a grommet. These work by allowing air to get in and out of the middle ear, which helps to drain the fluid. Grommets are usually put in with a general anesthetic, which means your child will be asleep during the procedure.
Grommets can improve hearing for up to nine months, but they have little effect on speech or language development in the long term. Different grommets stay in for different lengths of time, but eventually they fall out and the eardrum closes.
In rare cases, surgery may be recommended to remove some glands at the back of the nose (adenoids). This is known as an adenoidectomy.
The specialist in hospital will help you decide on the best treatment option.
Figure 3. Glue ear grommets
Grommets for treating glue ear
Grommets are small temporary tubes that are placed in your child’s ear during surgery. They help drain fluid away and keep the eardrum open.
The grommet should fall out naturally within 6 to 12 months as your child’s ear gets better.
Are there any risks to grommets?
Every operation carries some risk of infection and bleeding but the hole in the eardrum is tiny, so this risk is reduced. Your ear, nose and throat (ENT) surgeon give your child a course of antibiotic eardrops to reduce the risk of infection further. Around one in every 100 children may develop a perforated eardrum. If this continues, your surgeon can repair it later. Every anesthetic carries a risk, but it’s very small. Modern anesthetics are safe and your child’s anesthetist will be an experienced doctor trained to deal with any complications.
Glue ear prognosis
Once your child’s glue ear is diagnosed and treated glue ear, the outlook is good. Most children with speech and language delays catch up and go on to have a normal school life. A small proportion of children may need extra help from a speech and language therapist.





{kind=link}