
Contents
Early miscarriage
Miscarriage also called early pregnancy loss is when a baby dies in the womb (uterus) before 20 weeks of pregnancy. A miscarriage is also known as the spontaneous abortion or unexpected loss of a pregnancy before the 20th week. For women who know they’re pregnant, about 10 to 15 in 100 pregnancies (10 to 15 percent) end in miscarriage. Most miscarriages happen in the first trimester before the 12th week of pregnancy. Miscarriage in the second trimester (between 13 and 19 weeks) happens in 1 to 5 in 100 (1 to 5 percent) pregnancies.
Miscarriage is a somewhat loaded term — possibly suggesting that something was amiss in the carrying of the pregnancy. This is rarely true. Most miscarriages occur because the fetus isn’t developing normally.
In some cases, the cause of your early miscarriage is unknown. Often, it is a random problem with chromosomes that happens at conception. You might be afraid that you did something that caused your miscarriage. But things like working, exercising, having sex, or morning sickness do not cause miscarriage. Any kind of fall or blow is rarely to blame. The research on the effects of alcohol, tobacco, and caffeine is unclear. So there is nothing you could have done to prevent it. It is not the result of anything you did or didn’t do. You should never blame yourself for a miscarriage.
As many as half of all pregnancies may end in miscarriage. But researchers don’t know the exact number because many miscarriages occur so early in pregnancy that a woman doesn’t realize she’s pregnant. Fortunately most women who miscarry go on to have a healthy pregnancy later.
The main sign of a miscarriage is vaginal bleeding. This may be followed by cramping or pain in the lower abdomen and fluid or tissue passing from the vagina. Most miscarriages happen very early in the pregnancy, often before a woman even knows she is pregnant. However, bear in mind that light vaginal bleeding is relatively common during the first trimester of pregnancy (the first 12 weeks) and doesn’t necessarily mean you’re having a miscarriage. To be sure, contact your health care provider right away if you have vaginal bleeding.
Factors that may contribute to miscarriage include:
- A genetic problem with the fetus
- Problems with the uterus or cervix
- Chronic diseases, such as polycystic ovary syndrome (PCOS)
Women who miscarry early in their pregnancy usually do not need any treatment. In some cases, there is tissue left in the uterus. Doctors use a procedure called a dilatation and curettage (D&C) or medicines to remove the tissue.
Miscarriage is a relatively common experience — but that doesn’t make it any easier. Take a step toward emotional healing by understanding what can cause a miscarriage, what increases the risk and what medical care might be needed.
Counseling may help you cope with your grief. Later, if you do decide to try again, work closely with your health care provider to lower the risks. Many women who have a miscarriage go on to have healthy babies.
What is recurrent miscarriage?
If you have recurrent miscarriages also called repeat miscarriages, you have two or more miscarriages in a row. About 1 in 100 women (1 percent) have repeat miscarriages. Most women who have recurrent miscarriages (50 to 75 in 100 or 75 percent) have an unknown cause. And most women with recurrent miscarriages with an unknown cause (65 in 100 women or 65 percent) go on to have a successful pregnancy.
Do I need any medical tests after a miscarriage or recurrent miscarriages?
If you miscarry in your first trimester, you probably don’t need any medical tests. Because doctors don’t often know what causes a miscarriage in the first trimester, tests may not be helpful in trying to find out a cause.
If you have recurrent miscarriages in the first trimester, or if you have a miscarriage in the second trimester, your doctor usually recommends tests to help find out the cause. Tests can include:
- Chromosome tests. You and your partner can have blood tests, like karyotyping, to check for chromosome problems. Karyotyping can count how many chromosomes there are and check to see if any chromosomes have changed. If tissue from the miscarriage is available, your provider can test it for chromosomal conditions.
- Hormone tests. You may have your blood tested to check for problems with hormones. Or you may have a procedure called endometrial biopsy that removes a small piece of the lining of the uterus to check for hormones.
- Blood tests to check your immune system. Your provider may test you for autoimmune disorders like, antiphospholipid syndrome (APS) and lupus (systemic lupus erythematosus or SLE).
- Looking at the uterus. You may have an ultrasound, a hysteroscopy (when your provider inserts a special scope through the cervix to see your uterus) or a hysterosalpingography (an X-ray of the uterus).
How long does it take to recover from a miscarriage?
It can take a few weeks to a month or more for your body to recover from a miscarriage. Depending on how long you were pregnant, you may have pregnancy hormones in your blood for 1 to 2 months after you miscarry. Most women get their period again 4 to 6 weeks after a miscarriage.
It may take longer to recover emotionally from a miscarriage. You may have strong feelings of grief about the death of your baby. Grief is all the feelings you have when someone close to you dies. Grief can make you feel sad, angry, confused or alone. It’s OK to take time to grieve after a miscarriage. Ask your friends and family for support, and find special ways to remember your baby. For example, if you already have baby things, like clothes and blankets, you may want to keep them in a special place. Or you may have religious or cultural traditions that you’d like to do for your baby. Do what’s right for you.
Certain things, like hearing names you were thinking of for your baby or seeing other babies, can be painful reminders of your loss. You may need help learning how to deal with these situations and the feelings they create. Tell your doctor if you need help to deal with your grief. And visit Share Your Story online community (https://share.marchofdimes.org) where you can talk with other parents who have had a miscarriage.
If I miscarry, when can you try to get pregnant again?
This is a decision for you to make with your partner and your doctor. It’s probably OK to get pregnant again after you’ve had at least one normal period. If you’re having medical tests to try to find out more about why you miscarried, you may need to wait until after you’ve had these tests to try to get pregnant again.
You may not be emotionally ready to try again so soon. Miscarriage can be hard to handle, and you may need time to grieve. It’s OK if you want to wait a while before trying to get pregnant again.
Miscarriage Facts
- As many as 1 in 4 pregnancies end in miscarriage 1).
- Among women who know they are pregnant, it is estimated that 1 in 6 pregnancies end in miscarriage.
- 1 in 4 women experience a miscarriage in their lifetime 2).
- The majority of miscarriages happen in the first trimester – about three in every four miscarriages happen during this period.
- Most miscarriages in the first trimester are caused by chromosomal abnormalities in the baby.
- The overall risk of miscarriage under 12 weeks in known pregnancies is 1 in 5.
- In women with a BMI (body mass index) over 30, the risk is 1 in 4.
- 1 in every 80-90 pregnancies is ectopic, which is around 12,000 pregnancies a year.
- About 1 in 100 women in the US experience recurrent miscarriages (three or more in a row) and more than 60% of these women go on to have a successful pregnancy.
Recurrent miscarriages
Many women who have a miscarriage worry they’ll have another if they get pregnant again. But most miscarriages are a one-off event.
About 1 in 100 women experience recurrent miscarriages (three or more in a row) and more than 60% of these women go on to have a successful pregnancy.
The age of the mother also influences the risk of miscarriage:
- In women under 30, 1 in 10 pregnancies will end in miscarriage.
- In women aged 35-39, this increases to up to 2 in 10 pregnancies.
- In women over 45, more than half of all pregnancies will end in miscarriage.
- In 2016, the average age of mothers increased to 30.4 years, compared with 30.3 years in 2015.
Misconceptions about miscarriage
What does NOT cause miscarriage:
- a mother’s emotional state during pregnancy, such as being stressed or depressed
- having a shock or fright during pregnancy
- exercise during pregnancy, including high-intensity activities such as jogging and cycling – but discuss with your doctor or midwife what type and amount of exercise is suitable for you during pregnancy
- lifting or straining during pregnancy
- working during pregnancy – or work that involves sitting or standing for long periods. Provided you’re not exposed to harmful chemicals or radiation. Talk with your doctor if you are concerned about work-related risks.
- having sex during pregnancy
- traveling by air
- eating spicy food
Miscarriage types
- Threatened miscarriage. If you’re bleeding but your cervix hasn’t begun to dilate, there is a threat of miscarriage. Such pregnancies often proceed without any further problems.
- Inevitable miscarriage. If you’re bleeding, cramping and your cervix is dilated, a miscarriage is considered inevitable.
- Incomplete miscarriage. If you pass fetal or placental material but some remains in your uterus, it’s considered an incomplete miscarriage.
- Missed miscarriage. In a missed miscarriage, the placental and embryonic tissues remain in the uterus, but the embryo has died or was never formed.
- Complete miscarriage. If you have passed all the pregnancy tissues, it’s considered a complete miscarriage. This is common for miscarriages occurring before 12 weeks.
- Septic miscarriage. If you develop an infection in your uterus, it’s known as a septic miscarriage. This can be a severe infection and demands immediate care.
- Recurrent miscarriage. If you have 3 or more miscarriages in your first trimester.
Miscarriage complications
Some women who miscarry develop a uterine infection, also called a septic miscarriage. Signs and symptoms of this infection include:
- Fever
- Chills
- Lower abdominal tenderness
- Foul-smelling vaginal discharge
When is the best time for pregnancy after miscarriage?
Miscarriage can cause intense feelings of loss. You and your partner might also experience anger, sadness or guilt. Don’t rush the grieving process.
Typically, sex is not recommended for two weeks after a miscarriage to prevent an infection. Talk to your health care provider about any recommendations or restrictions. Your period will likely return within six weeks; however, it’s possible to become pregnant if you have sex before your period returns.
Once you feel ready for pregnancy after miscarriage, ask your health care provider for guidance. Also, consider these guidelines if you’ve had:
- 1 miscarriage. Some research has shown that women who conceived within six months of having a miscarriage in their first pregnancy had fewer complications than did those who waited longer to conceive. If you’re healthy and feel ready, there might be no need to wait to conceive after miscarriage.
- 2 or more miscarriages. If you’ve had two or more miscarriages, talk to your health care provider. He or she might recommend testing to determine any underlying issues, as well as possible treatments, before attempting another pregnancy.
Is there anything that can be done to improve the chances of a healthy pregnancy?
Often, there’s nothing you can do to prevent a miscarriage. However, making healthy lifestyle choices before conception and during pregnancy is important for you and your baby. Take a daily prenatal vitamin or folic acid supplement, ideally beginning a few months before conception. Maintain a healthy weight and limit caffeine. Avoid alcohol, smoking and illegal drugs.
If you’ve had multiple miscarriages, future pregnancies need to be carefully planned and monitored. Consult your health care provider before conceiving again and see your doctor as soon as you think you might be pregnant.
What emotions are likely during subsequent pregnancies?
Once you become pregnant again after miscarriage, you’ll likely feel joyful — as well as anxious and scared. You might be hesitant to share your good news until later in your pregnancy. Feelings of grief over your loss also might return after you give birth. This is normal.
Talk about your feelings and allow yourself to experience them fully. Turn to your partner, family and friends for comfort. If you’re having trouble coping, consult your health care provider or a counselor for extra support.
Causes of miscarriage
There are probably many reasons why a miscarriage may happen, although the cause isn’t usually identified. The majority aren’t caused by anything the mother has done.
It’s thought most miscarriages are caused by abnormal chromosomes in the baby. Chromosomes are genetic “building blocks” that guide the development of a baby. If a baby has too many or not enough chromosomes, it won’t develop properly.
- If a miscarriage happens during the first trimester of pregnancy (the first three months), it’s usually caused by problems with the unborn baby (fetus). About three in every four miscarriages happen during this period.
- If a miscarriage happens during the second trimester of pregnancy (between weeks 14 and 26), it’s sometimes the result of an underlying health condition in the mother.
- These late miscarriages may be caused by an infection around the baby, which leads to the bag of waters breaking before any pain or bleeding. In rare cases, they can be caused by the neck of the womb opening too soon.
For most women, a miscarriage is a one-off event and they go on to have a successful pregnancy in the future.
Problems with chromosomes
About half of all miscarriages are caused when an embryo (fertilized egg) gets the wrong number of chromosomes. This usually happens by chance and not from a problem passed from parent to child through genes. Chromosomes are the structures in cells that holds genes. Each person has 23 pairs of chromosomes, or 46 in all. For each pair, you get one chromosome from your mother and one from your father. Examples of chromosome problems that can cause miscarriage include:
- Blighted ovum. This is when an embryo implants in the uterus but doesn’t develop into a baby. If you have a blighted ovum, you may have dark-brown bleeding from the vagina early in pregnancy. If you’ve had signs or symptoms of pregnancy, like sore breasts or nausea (feeling sick to your stomach), you may stop having them.
- Intrauterine fetal demise. This is when an embryo stops developing and dies.
- Molar pregnancy. This is when tissue in the uterus forms into a tumor at the beginning of pregnancy. But it still causes regular pregnancy symptoms. These include a missed period, positive pregnancy test, and nausea.
- Translocation. This is when part of a chromosome moves to another chromosome. Translocation causes a small number of repeat miscarriages.
Problems with the uterus or cervix
The cervix is the opening to the uterus that sits at the top of the vagina. Problems with the uterus and cervix that can cause miscarriage include:
- Septate uterus. This is when a band of muscle or tissue (called a septum) divides the uterus in two sections. If you have a septate uterus, your provider may recommend surgery before you try to get pregnant to repair the uterus to help reduce your risk of miscarriage. Septate uterus the most common kind of congenital uterine abnormality. This means it’s a condition that you’re born with that affects the size, shape or structure of the uterus. Septate uterus is a common cause of repeat miscarriages.
- Asherman syndrome. If you have this condition, you have scars or scar tissue in the uterus that can damage the endometrium (the lining of the uterus). Before you get pregnant, your provider may use a procedure called hysteroscopy to find and remove scar tissue. Asherman syndrome may often cause repeat miscarriages that happen before you know you’re pregnant.
- Uterine fibroids (growths) in the uterus or scars from surgery on the uterus. Fibroids and scars can limit space for your baby or interfere with your baby’s blood supply. Before you try to get pregnant, you may need a surgery called myomectomy to remove them.
- Cervical insufficiency also called incompetent cervix. This is when your cervix opens (dilates) too early during pregnancy, usually without pain or contractions. Contractions are when the muscles of your uterus get tight and then relax to help push your baby out during labor and birth. Cervical insufficiency may lead to miscarriage, usually in the second trimester. To help prevent this, your provider may recommend cerclage. This is a stitch your provider puts in your cervix to help keep it closed.
Infections
Infections, like sexually transmitted infections also called STIs and listeriosis, can cause miscarriage. An sexually transmitted infection, like genital herpes and syphilis, is an infection you can get from having sex with someone who is infected. If you think you may have an sexually transmitted infection, tell your health care provider right away. Early testing and treatment can help protect you and your baby. Listeriosis is a kind of food poisoning. If you think you have listeriosis, call your provider right away. Your provider may treat you with antibiotics to help keep you and your baby safe. Having certain infections may cause miscarriage, but they’re not likely to cause repeat miscarriages.
First trimester miscarriages (early miscarriage)
Most first trimester miscarriages are caused by problems with the chromosomes of the fetus.
Chromosomes are blocks of DNA. They contain a detailed set of instructions that control a wide range of factors, from how the cells of the body develop to what color eyes a baby will have.
Sometimes something can go wrong at the point of conception and the fetus receives too many or not enough chromosomes. The reasons for this are often unclear, but it means the fetus won’t be able to develop normally, resulting in a miscarriage.
It’s estimated up to two-thirds of early miscarriages are associated with chromosome abnormalities. This is very unlikely to recur and doesn’t mean there’s any problem with the mother or father’s chromosomes.
Abnormal genes or chromosomes
Most miscarriages occur because the fetus isn’t developing normally. About 50 percent of miscarriages are associated with extra or missing chromosomes. Most often, chromosome problems result from errors that occur by chance as the embryo divides and grows — not problems inherited from the parents.
Chromosomal abnormalities might lead to:
- Blighted ovum. Blighted ovum occurs when no embryo forms.
- Intrauterine fetal demise. In this situation, an embryo forms but stops developing and dies before any symptoms of pregnancy loss occur.
- Molar pregnancy and partial molar pregnancy. With a molar pregnancy, both sets of chromosomes come from the father. A molar pregnancy is associated with abnormal growth of the placenta; there is usually no fetal development. A partial molar pregnancy occurs when the mother’s chromosomes remain, but the father provides two sets of chromosomes. A partial molar pregnancy is usually associated with abnormalities of the placenta, and an abnormal fetus. Molar and partial molar pregnancies are not viable pregnancies. Molar and partial molar pregnancies can sometimes be associated with cancerous changes of the placenta.
- Translocation. This is when part of a chromosome moves to another chromosome. Translocation causes a small number of repeat miscarriages.
Placental problems
The placenta is the organ linking the mother’s blood supply to her baby’s. If there’s a problem with the development of the placenta, it can also lead to a miscarriage.
Things that increase your risk:
An early miscarriage may happen by chance. But there are several things known to increase your risk of problems happening.
The age of the mother has an influence:
- in women under 30, 1 in 10 pregnancies will end in miscarriage
- in women aged 35-39, up to 2 in 10 pregnancies will end in miscarriage
- in women over 45, more than half of all pregnancies will end in miscarriage
Other risk factors include:
- obesity
- smoking during pregnancy
- drug misuse during pregnancy
- drinking more than 200mg of caffeine a day – one mug of tea contains around 75mg of caffeine, and one mug of instant coffee contains around 100mg of caffeine; caffeine is also found in some fizzy drinks, energy drinks and chocolate bars
- drinking more than two units of alcohol a week – one unit is half a pint of bitter or ordinary strength lager, or a 25 ml measure of spirits, and a small 125 ml glass of wine is 1.5 units
Second trimester miscarriages
Maternal health conditions
In a few cases, a mother’s health condition might lead to miscarriage. Examples include:
- Uncontrolled diabetes
- Infections
- Hormonal problems
- Uterus or cervix problems
- Thyroid disease
- Severe high blood pressure
- Lupus
- Kidney disease
- An overactive thyroid gland (hyperthyroidism)
- An underactive thyroid gland (hypothyroidism)
- Autoimmune disorders
- Obesity
Preexisting diabetes (also called type 1 or type 2 diabetes). Diabetes is when you have too much sugar (also called glucose) in your blood. Preexisting diabetes means you have diabetes before you get pregnant.
Thyroid problems, including hypothyroidism and hyperthyroidism. They thyroid is a butterfly-shaped gland in your neck. Hypothyroidism is when the thyroid gland doesn’t make enough thyroid hormones. Hyperthyroidism is when the thyroid gland makes too many thyroid hormones.
Autoimmune disorders. These are health conditions that happen when antibodies (cells in the body that fight off infections) attack healthy tissue by mistake. Autoimmune disorders that may increase your risk of miscarriage include antiphospholipid syndrome (also called APS) and lupus (also called systemic lupus erythematosus or SLE). If you have APS, your body makes antibodies that attack certain fats that line the blood vessels; this can sometimes cause blood clots. If you have APS and have had repeat miscarriages, your provider may give you low-dose aspirin and a medicine called heparin during pregnancy and for a few weeks after you give birth to help prevent another miscarriage. Lupus can cause swelling, pain and sometimes organ damage. It can affect your joints, skin, kidneys, lungs and blood vessels. If you have lupus, your provider may treat you with low-dose aspirin and heparin during pregnancy.
Obesity. This means you have too much body fat and your body mass index (also called BMI) is 30 or higher. BMI is a measure of body fat based on your height and weight. If you’re obese, your chances of having a miscarriage may increase.
Womb structure
Problems and abnormalities with your womb can also lead to second trimester miscarriages. Possible problems include:
- non-cancerous growths in the womb called uterine fibroids
- an abnormally shaped womb
Septate uterus. This is when a band of muscle or tissue (called a septum) divides the uterus in two sections. If you have a septate uterus, your provider may recommend surgery before you try to get pregnant to repair the uterus to help reduce your risk of miscarriage. Septate uterus the most common kind of congenital uterine abnormality. This means it’s a condition that you’re born with that affects the size, shape or structure of the uterus. Septate uterus is a common cause of repeat miscarriages.
Asherman syndrome. If you have this condition, you have scars or scar tissue in the uterus that can damage the endometrium (the lining of the uterus). Before you get pregnant, your provider may use a procedure called hysteroscopy to find and remove scar tissue. Asherman syndrome may often cause repeat miscarriages that happen before you know you’re pregnant.
Weakened cervix
In some cases, the muscles of the cervix (neck of the womb) are weaker than usual. This is known as a weakened cervix or cervical incompetence.
A weakened cervix may be caused by a previous injury to this area, usually after a surgical procedure. This is when your cervix opens (dilates) too early during pregnancy, usually without pain or contractions, leading to a miscarriage. Contractions are when the muscles of your uterus get tight and then relax to help push your baby out during labor and birth. Cervical insufficiency may lead to miscarriage, usually in the second trimester. To help prevent this, your provider may recommend cerclage. This is a stitch your provider puts in your cervix to help keep it closed.
Polycystic ovary syndrome
Polycystic ovary syndrome (PCOS) is a condition where the ovaries are larger than normal. It’s caused by hormonal changes in the ovaries.
PCOS is known to be a leading cause of infertility as it can lower the production of eggs. There’s some evidence to suggest it may also be linked to an increased risk of miscarriages in fertile women.
However, the exact role polycystic ovary syndrome plays in miscarriages is unclear. No treatment has been proven to make a difference and the majority of women with PCOS have successful pregnancies with no increased risk of miscarriage.
Infections
The following infections may also increase your risk:
- rubella (German measles)
- cytomegalovirus
- bacterial vaginosis
- HIV
- chlamydia
- gonorrhea
- syphilis
- malaria
An sexually transmitted infection (STI), like genital herpes and syphilis, is an infection you can get from having sex with someone who is infected. If you think you may have an sexually transmitted infection (STI), tell your health care provider right away. Early testing and treatment can help protect you and your baby.
Food poisoning
Food poisoning, caused by eating contaminated food, can also increase the risk of miscarriage. For example:
- listeriosis – most commonly found in unpasteurized dairy products, such as blue cheese
- toxoplasmosis – which can be caught by eating raw or undercooked infected meat, particularly lamb, pork or venison
- salmonella – most often caused by eating raw or partly cooked eggs
Listeriosis is a kind of food poisoning. If you think you have listeriosis, call your provider right away. Your provider may treat you with antibiotics to help keep you and your baby safe. Having certain infections may cause miscarriage, but they’re not likely to cause repeat miscarriages.
Foods to avoid in pregnancy
There are some foods to avoid or take care with when you’re pregnant as they might make you ill or harm your baby.
Make sure you know the important facts about which foods you should avoid or take precautions with when you’re pregnant.
AVOID some raw or partially cooked eggs if you’re pregnant
AVOID all types of pâté, including vegetable pâtés, as they can contain listeria.
Liver can harm your unborn baby. Don’t eat liver or products containing liver, such as liver pâté, liver sausage or haggis, as they may contain a lot of vitamin A. Too much vitamin A can harm your baby.
Raw or undercooked meat is risky in pregnancy
Do not eat raw or undercooked meat, including meat joints and steaks cooked rare, because of the potential risk of toxoplasmosis.
Cook all meat and poultry thoroughly so it’s steaming hot and there’s no trace of pink or blood – especially with poultry, pork, sausages and minced meat, including burgers.
Wash all surfaces and utensils thoroughly after preparing raw meat to avoid the spread of harmful bugs. Wash and dry your hands after touching or handling raw meat.
Toxoplasmosis is an infection caused by a parasite found in raw and undercooked meat, unpasteurised goats’ milk, soil, cat poo, and untreated water.
If you’re pregnant, the infection can damage your baby, but it’s important to remember toxoplasmosis in pregnancy is very rare.
Toxoplasmosis often has no symptoms, but if you feel you may have been at risk, discuss it with your doctor, midwife or obstetrician. If you’re infected while you’re pregnant, treatment for toxoplasmosis is available.
Game
It’s best to avoid eating game that has been shot with lead pellets while you’re pregnant, as it may contain higher levels of lead. Venison and other large game sold in supermarkets is usually farmed and contains no or very low levels of lead. If you’re not sure whether a product may contain lead shot, ask a retailer.
Cheeses to AVOID in pregnancy
- Soft cheeses with white rinds
Don’t eat mould-ripened soft cheese (cheeses with a white rind) such as brie and camembert. This includes mould-ripened soft goats’ cheese, such as chèvre. These cheeses are only safe to eat in pregnancy if they’ve been cooked.
- Soft blue cheeses
You should also avoid soft blue-veined cheeses such as danish blue, gorgonzola and roquefort. Soft blue cheeses are only safe to eat in pregnancy if they’ve been cooked.
It’s advised pregnant women avoid some soft cheeses because they’re less acidic than hard cheeses and contain more moisture, which means they can be an ideal environment for harmful bacteria, such as listeria, to grow in.
Although infection with listeria (listeriosis) is rare, it’s important to take special precautions in pregnancy – even a mild form of the illness in a pregnant woman can lead to miscarriage, stillbirth or severe illness in a newborn baby.
Cheeses that are SAFE TO EAT in pregnancy
All hard cheeses are safe in pregnancy
You can eat hard cheeses, such as cheddar, parmesan and stilton, even if they’re made with unpasteurized milk. Hard cheeses don’t contain as much water as soft cheeses, so bacteria are less likely to grow in them. It’s possible for hard cheese to contain listeria, but the risk is considered to be low.
Soft cheeses that are safe to eat in pregnancy
Other than mold-ripened soft cheeses, all other soft types of cheese are OK to eat, provided they’re made from pasteurized milk.
These include:
- cottage cheese
- mozzarella
- feta
- cream cheese
- paneer
- ricotta
- halloumi
- goats’ cheese
- processed cheeses, such as cheese spreads
Cooked soft cheeses that are safe to eat in pregnancy
Thorough cooking should kill any bacteria in cheese, so it should be safe to eat cooked mold-ripened soft cheese, such as brie, camembert and chèvre, and cooked soft blue cheese, such as roquefort or gorgonzola, or dishes that contain them.
It’s important to make sure the cheese is thoroughly cooked until it’s steaming hot all the way through.
Be cautious with cold cured meats in pregnancy
Many cold meats, such as salami, prosciutto, chorizo and pepperoni, are not cooked, they’re just cured and fermented. This means there’s a risk they contain toxoplasmosis-causing parasites.
It’s best to check the instructions on the pack to see whether the product is ready to eat or needs cooking first.
For ready-to-eat meats, you can reduce any risk from parasites by freezing cured or fermented meats for four days at home before you eat them. Freezing kills most parasites and makes the meat safer to eat.
If you’re planning to cook the meat – for instance, pepperoni on pizza – you don’t need to freeze it first.
If you’re eating out in a restaurant that sells cold cured or fermented meats, they may not have been frozen. If you’re concerned, ask the staff or avoid eating it.
Pre-packed meat is safe to eat if you’re pregnant
Pre-packed meats such as ham and corned beef are safe to eat in pregnancy. Some websites based in other countries may suggest that you avoid pre-packed meats when pregnant.
Vitamin and fish oil supplements
Don’t take high-dose multivitamin supplements, fish liver oil supplements, or any supplements containing vitamin A.
Fish in pregnancy
You can eat most types of fish when you’re pregnant. Eating fish is good for your health and the development of your baby, but you should avoid some types of fish and limit the amount you eat of some others.
Recommendations from the Dietary Guidelines for Americans: The 2015–2020 Dietary Guidelines for Americans states that women who are pregnant or breastfeeding should consume 8–12 ounces of seafood per week, choosing from varieties that are higher in EPA and DHA and lower in methyl mercury, such as salmon, herring, sardines, and trout. These women should not consume certain types of fish, such as king mackerel, shark, swordfish, and tilefish that are high in methyl mercury, and they should limit the amount of white (albacore) tuna they consume to 6 ounces a week. The American Academy of Pediatrics has similar advice for breastfeeding women, recommending intakes of 200–300 mg DHA per day by consuming one to two servings of fish per week to guarantee a sufficient amount of DHA in breast milk 3).
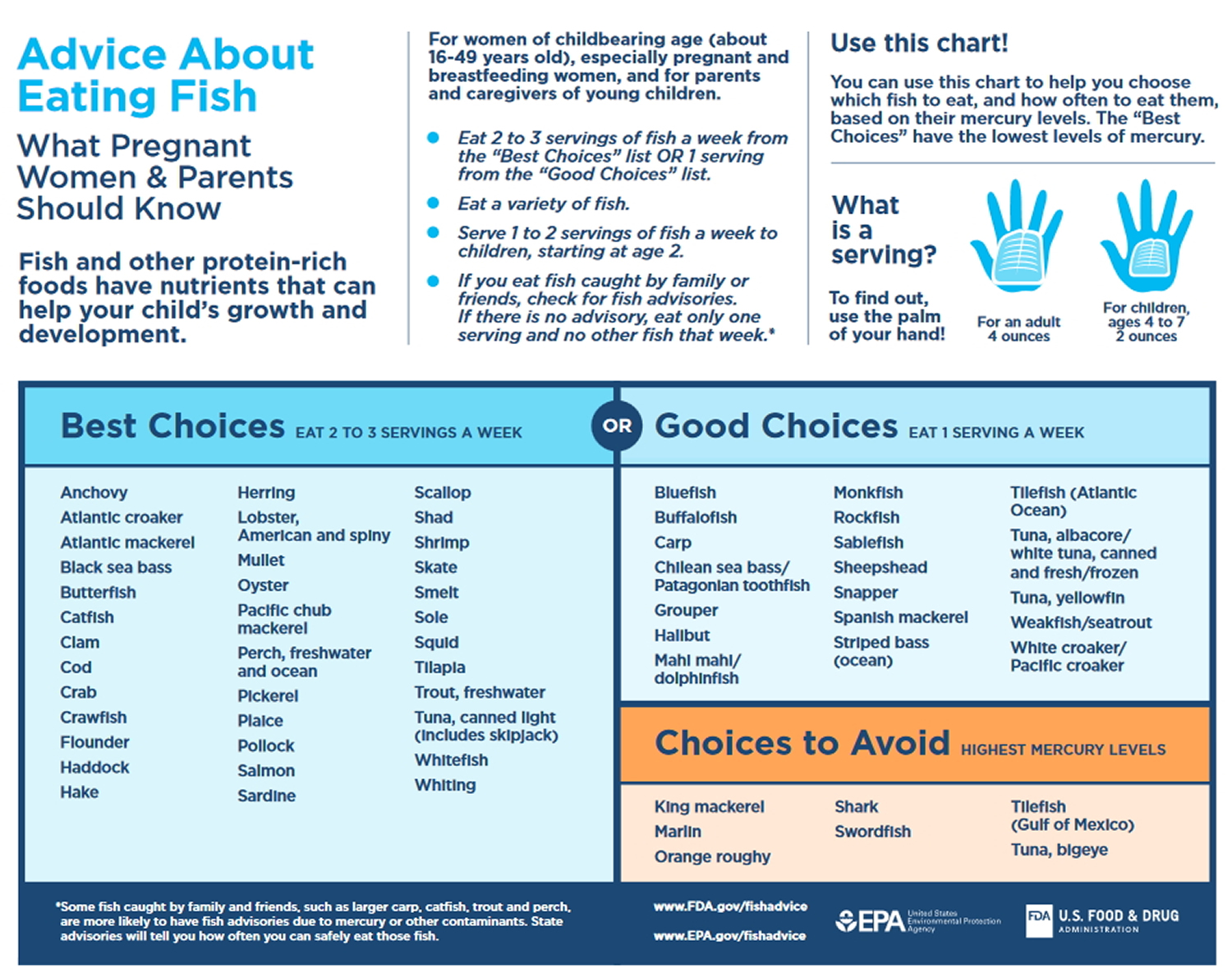
Fish to avoid:
When you’re pregnant or planning to get pregnant, you shouldn’t eat shark, swordfish or marlin.
Fish to restrict:
You should also limit the amount of tuna you eat to:
- no more than two tuna steaks a week (about 140g cooked or 170g raw each), or
- four medium-sized cans of tuna a week (about 140g when drained)
This is because tuna contains more mercury than other types of fish. The amount of mercury you get from food isn’t harmful for most people, but could affect your baby’s developing nervous system if you take in high levels of mercury when you’re pregnant.
When you’re pregnant, you should also avoid having more than two portions of oily fish a week, such as salmon, trout, mackerel and herring, as it can contain pollutants like dioxins and polychlorinated biphenyls (PCBs).
Remember, fresh tuna is an oily fish, so if you eat two fresh tuna steaks in one week, you shouldn’t eat any other oily fish that week.
Tinned tuna doesn’t count as oily fish, so you can eat this on top of the maximum amount of two portions of oily fish (as long as it’s not fresh tuna).
But remember not to eat more than four medium-sized cans of tinned tuna a week when you’re pregnant or trying to get pregnant.
Fish that’s safe to eat:
There’s no need to limit the amount of white fish and cooked shellfish you eat when you’re pregnant or breastfeeding.
Shellfish in pregnancy
Always eat cooked, rather than raw, shellfish – including mussels, lobster, crab, prawns, scallops and clams – when you’re pregnant, as they can contain harmful bacteria and viruses that can cause food poisoning. Cold pre-cooked prawns are fine.
Smoked fish in pregnancy is safe
Smoked fish, which includes smoked salmon and smoked trout, is considered safe to eat in pregnancy.
Sushi and pregnancy
It’s fine to eat raw or lightly cooked fish in dishes like sushi when you’re pregnant, as long as any raw wild fish used to make it has been frozen first.
This is because, occasionally, wild fish contains small parasitic worms that could make you ill. Freezing kills the worms and makes raw fish safe to eat. Cooking will also kill them.
Certain farmed fish destined to be eaten raw in dishes like sushi, such as farmed salmon, no longer need to be frozen beforehand.
This is because farmed fish are very unlikely to contain parasitic worms as a result of the rearing methods used. If you’re unsure, contact the U.S. Food and Drug Administration 5) for advice.
Lots of the sushi sold in shops is not made at the shop. This type of sushi should be fine to eat – if a shop or restaurant buys in ready-made sushi, the raw fish used to make it will have been subject to an appropriate freezing treatment.
If you’re in any doubt, you might want to avoid eating the kinds of sushi that contain raw fish, such as tuna.
The safest way to enjoy sushi is to choose the fully cooked or vegetarian varieties, which can include:
- cooked seafood – for example, fully cooked eel (unagi) or shrimp (ebi)
- vegetables – for example, cucumber (kappa) maki
- avocado – for example, California roll
- fully cooked egg
If a shop or restaurant makes its own sushi on the premises, it must still be frozen first before being served. If you’re concerned, ask the staff.
If you make your own sushi at home, freeze the fish for at least four days before using it.
Peanuts are safe in pregnancy
You can eat peanuts or food containing peanuts, such as peanut butter, during pregnancy, unless you’re allergic to them or a health professional advises you not to.
You may have heard peanuts should be avoided during pregnancy. This is because the government previously advised women to avoid eating peanuts if there was a history of allergy – such as asthma, eczema, hay fever and food allergy – in their child’s immediate family.
This advice has now changed because the latest research has shown no clear evidence that eating peanuts during pregnancy affects the chances of your baby developing a peanut allergy.
Milk and yoghurt in pregnancy
Stick to pasteurized or ultra-heat treated (UHT) milk, which is sometimes called long-life milk.
If only raw (unpasteurized) milk is available, boil it first. Don’t drink unpasteurized goats’ or sheep’s milk, or eat foods made from them, such as soft goats’ cheese.
All types of yogurt, including bio, live and low fat, are fine. Just check that any homemade yoghurt is made with pasteurized milk, and, if not, avoid it.
Ice cream in pregnancy
Soft ice creams should be fine to eat when you’re pregnant, as they are processed products made with pasteurized milk and eggs, so any risk of salmonella food poisoning has been eliminated.
For homemade ice cream, use a pasteurized egg substitute or follow an egg-free recipe.
Foods with soil on them
Wash fruit, vegetables and salads to remove all traces of soil and visible dirt.
Caffeine in pregnancy
High levels of caffeine can result in babies having a low birthweight, which can increase the risk of health problems in later life. Too much caffeine can also cause miscarriage.
Caffeine is naturally found in lots of foods, such as coffee, tea (including green tea) and chocolate, and is added to some soft drinks and energy drinks.
Some cold and flu remedies also contain caffeine. Talk to your midwife, doctor or pharmacist before taking these remedies.
You don’t need to cut out caffeine completely, but don’t have more than 200mg a day.
The approximate amount of caffeine found in food and drinks is:
- one mug of instant coffee: 100mg
- one mug of filter coffee: 140mg
- one mug of tea: 75mg
- one can of cola: 40mg
- one 250ml can of energy drink: 80mg (larger cans of energy drink may have up to 160mg caffeine)
- one 50g bar of plain (dark) chocolate: most US brands contain less than 25mg
- one 50g bar of milk chocolate: most US brands contain less than 10mg
So, if you have one can of cola and one mug of filter coffee, for example, you have reached almost 200mg of caffeine. Don’t worry if you occasionally have more than this amount – the risks are small.
To cut down on caffeine, try decaffeinated tea and coffee, fruit juice or mineral water instead of regular tea, coffee, cola and energy drinks.
Herbal and green teas in pregnancy
There’s little information on the safety of herbal and green teas in pregnancy, so it’s best to drink them in moderation.
The food safety authority recommends drinking no more than around four cups of herbal or green tea a day during pregnancy, and to seek advice from your doctor or midwife if you’re unsure about which herbal products are safe to consume.
Bear in mind that green tea contains caffeine.
Liquorice
You can have moderate amounts of liquorice sweets or liquorice teas in pregnancy – there’s no recommendation to avoid them. However, you should avoid the herbal remedy liquorice root.
Medicines
Medicines that increase your risk include:
- misoprostol – used for conditions such as rheumatoid arthritis
- retinoids – used for eczema and acne
- methotrexate – used for conditions such as rheumatoid arthritis
- non-steroidal anti-inflammatory drugs (NSAIDs) – such as ibuprofen; these are used for pain and inflammation
To be sure a medicine is safe in pregnancy, always check with your doctor, midwife or pharmacist before taking it.
Risk factors for miscarriage
Some things may make you more likely than other woman to have a miscarriage. These are called risk factors. Risk factors for miscarriage include:
- Age. Women older than age 35 have a higher risk of miscarriage than do younger women. At age 35, you have about a 20 percent risk. At age 40, the risk is about 40 percent. And at age 45, it’s about 80 percent.
- Previous miscarriages. Women who have had two or more consecutive miscarriages are at higher risk of miscarriage.
- Chronic conditions. Women who have a chronic condition, such as uncontrolled diabetes, have a higher risk of miscarriage.
- Uterine or cervical problems. Certain uterine abnormalities or weak cervical tissues (incompetent cervix) might increase the risk of miscarriage.
- Smoking, alcohol and illicit drugs. Women who smoke during pregnancy have a greater risk of miscarriage than do nonsmokers. Heavy alcohol use and illicit drug use also increase the risk of miscarriage.
- Weight. Being underweight or being overweight has been linked with an increased risk of miscarriage.
- Invasive prenatal tests. Some invasive prenatal genetic tests, such as chorionic villus sampling and amniocentesis, carry a slight risk of miscarriage.
- Being exposed to harmful chemicals. You or your partner having contact with harmful chemicals, like solvents, may increase your risk of miscarriage. A solvent is a chemical that dissolves other substances, like paint thinner. Talk to your provider about what you can do to protect yourself and your baby.
Some health conditions may increase your risk for miscarriage. Treatment of these conditions before and during pregnancy can sometimes help prevent miscarriage and repeat miscarriages. If you have any of these health conditions, tell your health care provider before you get pregnant or as soon as you know you’re pregnant:
- Autoimmune disorders. These are health conditions that happen when antibodies (cells in the body that fight off infections) attack healthy tissue by mistake. Autoimmune disorders that may increase your risk of miscarriage include antiphospholipid syndrome also called APS and lupus also called systemic lupus erythematosus or SLE. If you have antiphospholipid syndrome, your body makes antibodies that attack certain fats that line the blood vessels; this can sometimes cause blood clots. If you have antiphospholipid syndrome and have had repeat miscarriages, your provider may give you low-dose aspirin and a medicine called heparin during pregnancy and for a few weeks after you give birth to help prevent another miscarriage. Lupus can cause swelling, pain and sometimes organ damage. It can affect your joints, skin, kidneys, lungs and blood vessels. If you have lupus, your provider may treat you with low-dose aspirin and heparin during pregnancy.
- Obesity. This means you have too much body fat and your body mass index (BMI) is 30 or higher. BMI is a measure of body fat based on your height and weight. If you’re obese, your chances of having a miscarriage may increase.
- Hormone problems, like polycystic ovary syndrome (PCOS) and luteal phase defect. Hormones are chemicals made by the body. PCOS happens when you have hormone problems and cysts on the ovaries. A cyst is a closed pocket of that contains air, fluid or semi-solid substances. If you’re trying to get pregnant, your provider may give you medicine to help you ovulate (release an egg from your ovary into the fallopian tubes). Luteal phase defect can cause repeat miscarriages. It’s when you have low levels of progesterone over several menstrual cycles. Progesterone is a hormone that helps regulate your periods and gets your body ready for pregnancy. If you have luteal phase defect, your provider may recommend treatment with progesterone before and during pregnancy to help prevent repeat miscarriages.
- Preexisting diabetes also called type 1 or type 2 diabetes. Diabetes is when you have too much sugar (also called glucose) in your blood. Preexisting diabetes means you have diabetes before you get pregnant.
- Thyroid problems, including hypothyroidism (underactive thyroid) and hyperthyroidism (overactive thyroid). They thyroid is a butterfly-shaped gland in your neck. Hypothyroidism is when the thyroid gland doesn’t make enough thyroid hormones. Hyperthyroidism is when the thyroid gland makes too many thyroid hormones.
- Having certain prenatal tests, like amniocentesis and chorionic villus sampling. These tests have a slight risk of miscarriage. Your provider may recommend them if your baby is at risk for certain genetic conditions, like Down syndrome.
- Having an injury to your belly, like from falling down or getting hit, isn’t a high risk for miscarriage. Your body does a good job of protecting your baby in the early weeks of pregnancy.
You may have heard that getting too much caffeine during pregnancy can increase your risk for miscarriage. Caffeine is a drug found in foods, drinks, chocolate and some medicine. It’s a stimulant, which means it can help keep you awake. Some studies say caffeine may cause miscarriage, and some say it doesn’t. Until scientists know more about how caffeine can affect pregnancy, it’s best to limit the amount you get to 200 milligrams each day. This is what’s in about one 12-ounce cup of coffee.
How to prevent miscarriage
There is no conclusive research that says there is anything you can do to prevent a miscarriage. You didn’t cause it, so you couldn’t have prevented it. Often, there’s nothing you can do to prevent a miscarriage. Simply focus on taking good care of yourself and your baby:
- Seek regular prenatal care.
- Avoid known miscarriage risk factors — such as smoking, drinking alcohol and illicit drug use.
- Take a daily multivitamin.
- Limit your caffeine intake. A recent study found that drinking more than two caffeinated beverages a day appeared to be associated with a higher risk of miscarriage.
- Eating a healthy, balanced diet with at least five portions of fruit and vegetables a day
- Making attempts to avoid certain infections during pregnancy, such as rubella
- Avoiding certain foods during pregnancy, which could make you ill or harm your baby
- Being a healthy weight before getting pregnant
If you have a chronic condition, work with your health care team to keep it under control.
Your weight
Obesity increases your risk of miscarriage. A person is obese when they have a body mass index (BMI) of over 30. You can check your BMI using the healthy weight calculator. If you’re pregnant, your midwife or doctor may be able to tell you your BMI.
The best way to protect your health and your baby’s wellbeing is to lose weight before you become pregnant. By reaching a healthy weight, you cut your risk of all the problems associated with obesity in pregnancy. Contact your doctor for advice about how to lose weight. They may be able to refer you to a specialist weight-loss clinic.
As yet, there’s no evidence to suggest losing weight during pregnancy lowers your risk of miscarriage, but eating healthily and activities such as walking and swimming are good for all pregnant women.
If you weren’t active before becoming pregnant, you should consult your midwife or doctor before starting a new exercise regimen while you’re pregnant.
Treating an identified cause
Sometimes the cause of a miscarriage can be identified. In these cases, it may be possible to have treatment to prevent this causing any more miscarriages. Some treatable causes of miscarriage are outlined below.
Antiphospholipid syndrome
Antiphospholipid syndrome (APS), also known as Hughes syndrome, is a condition that causes blood clots. It can be treated with medication. Research has shown that a combination of aspirin and heparin (a medicine used to prevent blood clots) can improve pregnancy outcomes in women with the condition.
Treatment for antiphospholipid syndrome during pregnancy
Women diagnosed with antiphospholipid syndrome are strongly advised to plan for any future pregnancy. This is because treatment to improve the outcome of a pregnancy is most effective when it begins as soon as possible after an attempt to conceive. Some medications used to treat antiphospholipid syndrome can also harm an unborn baby.
If you don’t plan your pregnancy, it may be several weeks before you realize you’re pregnant. This may increase the risk of treatment to safeguard the pregnancy being unsuccessful.
Treatment during pregnancy involves taking daily doses of aspirin or heparin, or a combination of both. This depends on whether you have a history of blood clots and previous complications during pregnancy. Warfarin isn’t recommended during pregnancy because it carries a small risk of causing birth defects.
Treatment with aspirin and/or heparin is usually started at the beginning of the pregnancy and may continue for one to six weeks after you have given birth.
Lifestyle changes
If you’re diagnosed with antiphospholipid syndrome, it’s important to take all possible steps to reduce your risk of developing blood clots. Effective ways of achieving this include:
- not smoking
- eating a healthy, balanced diet – low in fat and sugar and containing plenty of fruit and vegetables
- taking regular exercise
- maintaining a healthy weight and losing weight if you are obese (have a body mass index of 30 or more)
Weakened cervix
A weakened cervix, also known as cervical incompetence, can be treated with an operation to put a small stitch of strong thread around your cervix to keep it closed. This is usually carried out after the first 12 weeks of your pregnancy, and is removed around week 37.
Miscarriage signs and symptoms
Most miscarriages occur before the 12th week of pregnancy.
Signs and symptoms of a miscarriage might include:
- Vaginal spotting or bleeding
- Pain or cramping in your abdomen or lower back
- Fluid or tissue passing from your vagina
If you have passed fetal tissue from your vagina, place it in a clean container and bring it to your health care provider’s office or the hospital for analysis.
Keep in mind that most women who experience vaginal spotting or bleeding in the first trimester go on to have successful pregnancies.
Miscarriage diagnosis
If you see your doctor or midwife because of vaginal bleeding or other symptoms of miscarriage, you may be referred to an early pregnancy unit at a hospital for tests.
If you’re more than 18 weeks pregnant, you’ll usually be referred to the maternity unit at the hospital.
Your health care provider might do a variety of tests:
- Pelvic exam. Your health care provider might check to see if your cervix has begun to dilate.
- Ultrasound. During an ultrasound, your health care provider will check for a fetal heartbeat and determine if the embryo is developing normally. If a diagnosis can’t be made, you might need to have another ultrasound in about a week.
- Blood tests. Your health care provider might check the level of the pregnancy hormone, human chorionic gonadotropin (HCG), in your blood and compare it to previous measurements. If the pattern of changes in your HCG level is abnormal, it could indicate a problem. Your health care provider might check to see if you’re anemic — which could happen if you’ve experienced significant bleeding — and may also check your blood type.
- Tissue tests. If you have passed tissue, it can be sent to a lab to confirm that a miscarriage has occurred — and that your symptoms aren’t related to another cause.
- Chromosomal tests. If you’ve had two or more previous miscarriages, your health care provider may order blood tests for both you and your partner to determine if your chromosomes are a factor.
Recurrent miscarriages
If you’ve had three or more miscarriages in a row (recurrent miscarriages), further tests are often used to check for any underlying cause. However, no cause is found in about half of cases. These further tests are outlined below.
If you become pregnant, most units offer an early ultrasound scan and follow-up in the early stages to reassure and support parents.
Karyotyping
If you’ve had a third miscarriage, it’s recommended that the foetus is tested for abnormalities in the chromosomes (blocks of DNA).
If a genetic abnormality is found, you and your partner can also be tested for abnormalities with your chromosomes that could be causing the problem, which is the rarest of known causes. This type of testing is known as karyotyping.
If karyotyping detects problems with your or your partner’s chromosomes, you can be referred to a clinical geneticist (gene expert).
They’ll be able to explain your chances of a successful pregnancy in the future and whether there are any fertility treatments, such as in vitro fertilisation (IVF), that you could try. This type of advice is known as genetic counseling.
Ultrasound scans
A transvaginal ultrasound can be used to check the structure of your womb for any abnormalities. A second procedure may be used with a 3D ultrasound scanner to study your lower abdomen and pelvis to provide a more accurate diagnosis.
The scan can also check if you have a weakened cervix. This test can usually only be carried out when you become pregnant again, in which case you’ll usually be asked to come for a scan when you are between 10 and 12 weeks pregnant.
Blood testing
Your blood can be checked for high levels of the antiphospholipid (aPL) antibody and lupus anticoagulant. This test should be done twice, six weeks apart, when you’re not pregnant.
Antiphospholipid (aPL) antibodies are known to increase the chance of blood clots and alter the way the placenta attaches. These blood clots and changes can reduce the blood supply to the foetus, which can cause a miscarriage.
Missed or delayed miscarriage
Sometimes a miscarriage is diagnosed during a routine scan carried out as part of your antenatal care. A scan may reveal your baby has no heartbeat, or that your baby is too small for the date of your pregnancy. This is called a missed or delayed miscarriage.
Miscarriage treatment
If there’s no pregnancy tissue left in your womb, no treatment is required.
Threatened miscarriage
For a threatened miscarriage, your health care provider might recommend resting until the bleeding or pain subsides. Bed rest hasn’t been proved to prevent miscarriage, but it’s sometimes prescribed as a safeguard. You might be asked to avoid exercise and sex, too. Although these steps haven’t been proved to reduce the risk of miscarriage, they might improve your comfort.
In some cases, it’s also a good idea to postpone traveling — especially to areas where it would be difficult to receive prompt medical care. Ask your doctor if it would be wise to delay any upcoming trips you’ve planned.
Miscarriage
With ultrasound, it’s now much easier to determine whether an embryo has died or was never formed. Either finding means that a miscarriage will definitely occur. In this situation, you might have several choices:
Expectant management
If you have no signs of infection and the embryo has died, you might choose to let the miscarriage progress naturally. It’s usually recommended you wait 7 to 14 days after a miscarriage for the tissue to pass out naturally. This is called expectant management. Unfortunately, it might take up to three or four weeks. This can be an emotionally difficult time. If expulsion doesn’t happen on its own, medical or surgical treatment will be needed.
If the pain and bleeding have lessened or stopped completely during this time, this usually means the miscarriage has finished. You should be advised to take a home pregnancy test after three weeks.
If the test shows you’re still pregnant, you may need to have further tests to make sure you don’t have a molar pregnancy or an ectopic pregnancy.
If the pain and bleeding haven’t started within 7 to 14 days or are continuing or getting worse, this could mean the miscarriage hasn’t begun or hasn’t finished. In this case, you should be offered another scan.
Contact your hospital immediately if the bleeding becomes particularly heavy, you develop a high temperature (fever), or you experience severe pain.
After this scan, you may decide to either continue waiting for the miscarriage to occur naturally, or have drug treatment or surgery. If you choose to continue to wait, your healthcare professional should check your condition again up to 14 days later.
Medical treatment
If, after a diagnosis of certain pregnancy loss, you’d prefer to speed the process, medication can cause your body to expel the pregnancy tissue and placenta. The medication can be taken by mouth or by insertion in the vagina. Your health care provider might recommend inserting the medication vaginally to increase its effectiveness and minimize side effects such as nausea and diarrhea. For about 70 to 90 percent of women, this treatment works within 24 hours.
You’ll experience symptoms similar to a heavy period, such as cramping and heavy vaginal bleeding. You may also experience vaginal bleeding for up to three weeks.
In most units, you’ll be sent home for the miscarriage to complete. This is safe, but ring your hospital if the bleeding becomes very heavy.
You should be advised to take a home pregnancy test three weeks after taking this medication. If the pregnancy test shows you’re still pregnant, you may need to have further tests to make sure you don’t have a molar pregnancy or an ectopic pregnancy.
You may be advised to contact your healthcare professional to discuss your options if bleeding hasn’t started within 24 hours of taking the medication.
Surgical treatment
Another option is a minor surgical procedure called suction dilation and curettage (D&C). During this procedure, your health care provider dilates your cervix with a small tube known as a dilator and removing any remaining tissue with a suction device. You should be offered a choice of general anesthetic or local anesthetic if both are suitable. Complications are rare, but they might include damage to the connective tissue of your cervix or the uterine wall.
In some cases, surgery is used to remove any remaining pregnancy tissue. You may be advised to have immediate surgery if:
- you experience continuous heavy bleeding
- there’s evidence the pregnancy tissue has become infected
- medication or waiting for the tissue to pass out naturally has been unsuccessful
If your blood group is RhD negative, you should be offered injections of a medication called anti-D immunoglobin afterwards. This is necessary to prevent rhesus disease.
Physical recovery
In most cases, physical recovery from miscarriage takes only a few hours to a couple of days. In the meantime, call your health care provider if you experience heavy bleeding, fever or abdominal pain.
You may ovulate as soon as two weeks after a miscarriage. Most women get their period again 4 to 6 weeks after a miscarriage. You can start using any type of contraception immediately after a miscarriage. However, avoid having sex or putting anything in your vagina — such as a tampon — for two weeks after a miscarriage.
Coping and support
Emotional healing can take much longer than physical healing. A miscarriage can have a profound emotional impact, not only on the woman herself, but also on her partner, friends and family. Your emotions might range from anger and guilt to despair. Give yourself time to grieve the loss of your pregnancy, and seek help from loved ones.
You may have strong feelings of grief about the death of your baby. Grief is all the feelings you have when someone close to you dies. Grief can make you feel sad, angry, confused or alone. It’s OK to take time to grieve after a miscarriage. Ask your friends and family for support, and find special ways to remember your baby. For example, if you already have baby things, like clothes and blankets, you may want to keep them in a special place. Or you may have religious or cultural traditions that you’d like to do for your baby. Do what’s right for you.
You’ll likely never forget your hopes and dreams surrounding this pregnancy, but in time acceptance might ease your pain. Talk to your health care provider if you’re feeling profound sadness or depression.
It’s usually possible to arrange a memorial and burial service if you want one. In some hospitals or clinics, it may be possible to arrange a burial within the grounds.
You can also arrange to have a burial at home, although you’ll need to consult your local authority before doing so.
Cremation is an alternative to burial and can be performed at either the hospital or a local crematorium. However, not all crematoriums provide this service and there won’t be any ashes for you to scatter afterwards.
Unlike a stillbirth, you don’t need to formally register a miscarriage. However, some hospitals can provide a certificate to mark what has happened if you want one.
Emotional impact
Sometimes the emotional impact is felt immediately after the miscarriage, whereas in other cases it can take several weeks. Many people affected by a miscarriage go through a bereavement period.
Certain things, like hearing names you were thinking of for your baby or seeing other babies, can be painful reminders of your loss. You may need help learning how to deal with these situations and the feelings they create. Tell your provider if you need help to deal with your grief. And visit Share Your Story, the March of Dimes online community 6) where you can talk with other parents who have had a miscarriage. We also offer the free booklet From hurt to healing that has information and resources for grieving parents.
It’s common to feel tired, lose your appetite and have difficulty sleeping after a miscarriage. You may also feel a sense of guilt, shock, sadness and anger – sometimes at a partner, or at friends or family members who have had successful pregnancies.
Different people grieve in different ways. Some people find it comforting to talk about their feelings, while others find the subject too painful to discuss.
Some women come to terms with their grief after a few weeks of having a miscarriage and start planning for their next pregnancy. For other women, the thought of planning another pregnancy is too traumatic, at least in the short term.
The father of the baby may also be affected by the loss. Men sometimes find it harder to express their feelings, particularly if they feel their main role is to support the mother and not the other way round. It may help to make sure you openly discuss how both of you are feeling.
Miscarriage can also cause feelings of anxiety or depression, and can lead to relationship problems.
Getting support
If you’re worried that you or your partner are having problems coping with grief, you may need further treatment and counseling. There are support groups that can provide or arrange counseling for people who have been affected by miscarriage.
Future pregnancies
It’s possible to become pregnant during the menstrual cycle immediately after a miscarriage. But if you and your partner decide to attempt another pregnancy, make sure you’re physically and emotionally ready. Ask your health care provider for guidance about when you might try to conceive.
Keep in mind that miscarriage is usually a one-time occurrence. Most women who miscarry go on to have a healthy pregnancy after miscarriage. Less than 5 percent of women have two consecutive miscarriages, and only 1 percent have three or more consecutive miscarriages.
The predicted risk of miscarriage in a future pregnancy remains about 14 percent after one miscarriage. After two miscarriages the risk of another miscarriage increases to about 26 percent, and after three miscarriages the risk of another miscarriage is about 28 percent.
If you experience multiple miscarriages, generally two or three in a row, consider testing to identify any underlying causes — such as uterine abnormalities, coagulation problems or chromosomal abnormalities. If the cause of your miscarriages can’t be identified, don’t lose hope. About 60 to 80 percent of women with unexplained repeated miscarriages go on to have healthy pregnancies.
Are special tests recommended before attempting pregnancy after miscarriage?
If you experience two or more consecutive miscarriages, talk with your health care provider about whether further testing is needed to identify any underlying causes before attempting to get pregnant again. For example:
- Blood tests. A sample of your blood is evaluated to help detect problems with hormones or your immune system.
- Chromosomal tests. You and your partner might both have your blood tested to determine if your chromosomes are a factor. Tissue from the miscarriage — if it’s available — also might be tested.
Procedures can be done to detect uterine problems. For example:
- Ultrasound. This imaging method uses high-frequency sound waves to produce precise images of structures within the body. Your health care provider places the ultrasound device (transducer) over your abdomen or places it inside your vagina to obtain images of your uterus. An ultrasound might identify uterine problems such as fibroids within the uterine cavity.
- Hysteroscopy. Your health care provider inserts a thin, lighted instrument called a hysteroscope through your cervix into your uterus to diagnose and treat identified intrauterine problems.
- Hysterosalpingography. Your health care provider inserts a catheter inside your cervix, which releases a liquid contrast material into your uterus. The dye traces the shape of your uterine cavity and fallopian tubes and makes them visible on X-ray images. This procedure provides information about the internal contours of the uterus and any obstructions in the fallopian tubes.
- Sonohysterogram. This ultrasound scan is done after fluid is injected into your uterus though your vagina and cervix. This procedure provides information about the internal contours of the uterus, the outer surface of the uterus and any obstructions in the fallopian tubes.
If the cause of your miscarriages can’t be identified, don’t lose hope. Most women who experience repeated miscarriages are likely to eventually have healthy pregnancies.
References [ + ]





{kind=link}