
Contents
What is costochondritis
Costochondritis is an inflammation of the cartilage that connects a rib to the breastbone (sternum) or chondrosternal joints of the anterior chest wall. Pain caused by costochondritis might mimic that of a heart attack or other heart conditions. Costochondritis is sometimes known as chest wall pain, costosternal syndrome or costosternal chondrodynia. Sometimes, swelling accompanies the pain (Tietze syndrome). Cartilage is tough but flexible connective tissue found throughout the body, including in the joints between bones. It acts as a shock absorber, cushioning the joints.
Costochondritis is a self-limited condition and most commonly affects the upper ribs (the second to fifth costal cartilages) on the left-hand side of your body, usually at multiple levels and lacking swelling or induration 1). Pain is often worst where the rib cartilage attaches to the breastbone (sternum) [chondrosternal joints], but it can also occur where the cartilage attaches to the rib [costochondral junctions of ribs].
Costochondritis usually has no apparent cause. Treatment focuses on easing your pain while you wait for the condition to improve on its own, which can take several weeks or longer.
Costochondritis can affect children as well as adults. A study of chest pain in an outpatient adolescent clinic found that 31 percent of adolescents had musculoskeletal causes, with costochondritis accounting for 14 percent of adolescent patients with chest pain 2). In this series, no definite cause of chest pain was found in 39 percent of cases 3). In a prospective series of children three to 15 years of age presenting to an emergency department or cardiac clinic with chest pain, chest wall pain was the most common diagnosis, with respiratory and psychogenic conditions the next most common diagnoses 4).
Costochondritis is a common diagnosis in adults with acute chest pain. It is present in 13 to 36 percent of these patients, depending on the study and the patient setting 5). In a prospective study of adult patients presenting to an emergency department with chest pain, 30 percent had costochondritis 6). A prospective study of episodes of care for chest pain in a primary care office network found musculoskeletal causes in 20 percent of episodes of care, with costochondritis responsible for 13 percent 7). These data are similar to a study of patients with noncardiac chest pain that found reproducible chest wall tenderness (although not specifically defined as costochondritis) in 16 percent of patients 8). A European study found a higher prevalence of musculoskeletal diagnoses in patients with chest pain presenting in primary care settings compared with hospital settings (20 versus 6 percent, respectively) 9).
Costochondritis usually goes away on its own, although it might last for several weeks or longer. Treatment focuses on pain relief.
Costochondritis may be confused with a separate condition called Tietze’s syndrome. Both conditions involve inflammation of the costochondral joint and can cause very similar symptoms. However, Tietze’s syndrome is much less common and often causes chest swelling, which may last after any pain and tenderness has gone. Tietze syndrome usually occurs in a single rib 70 percent of the time, usually within costal cartilages of ribs two through three, predominantly in rib two 10).
Costochondritis also tends to affect adults aged 40 or over, whereas Tietze’s syndrome usually affects young adults under 40.
Figure 1. Costochondritis
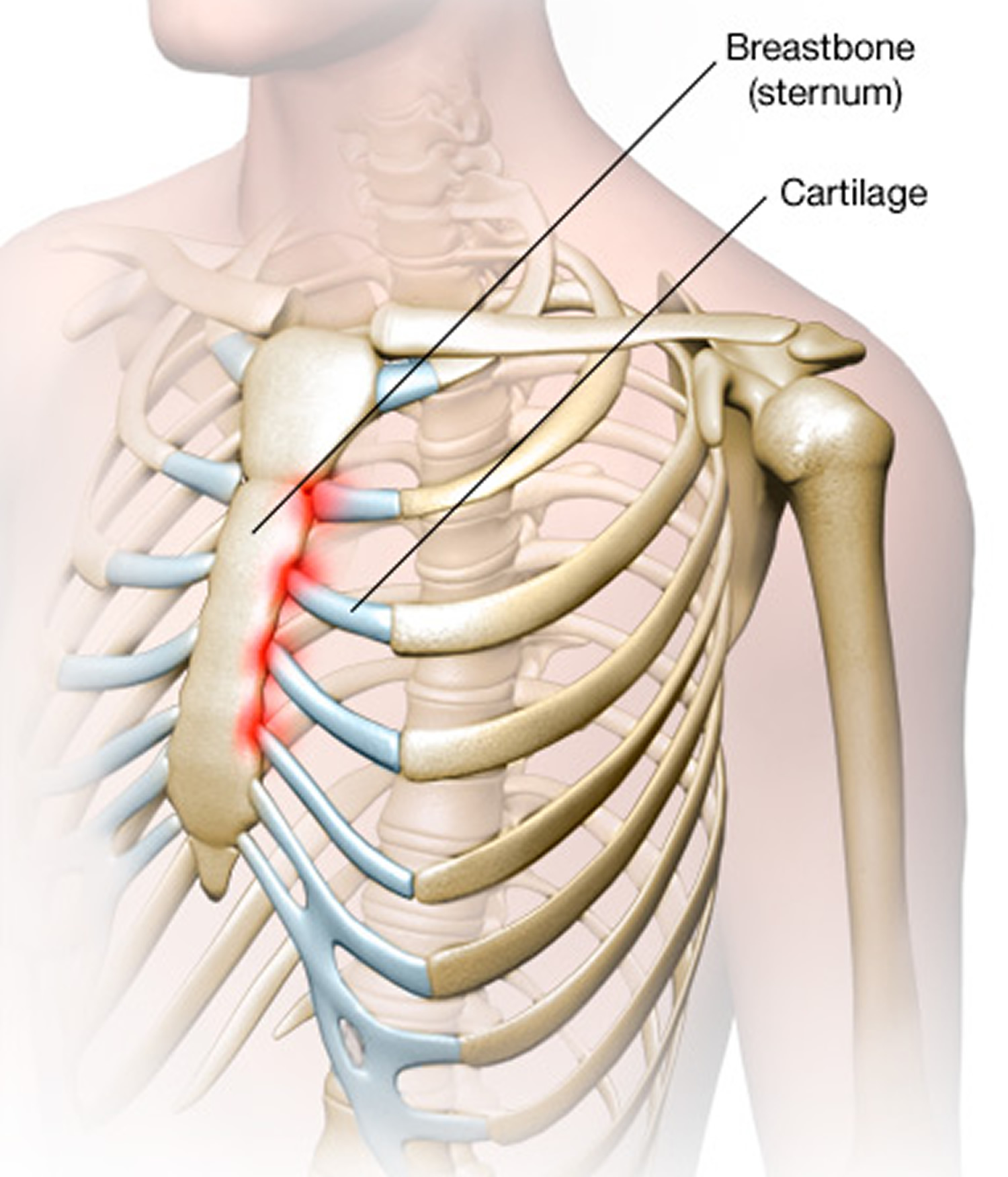
Figure 2. Sternum and chest wall anatomy
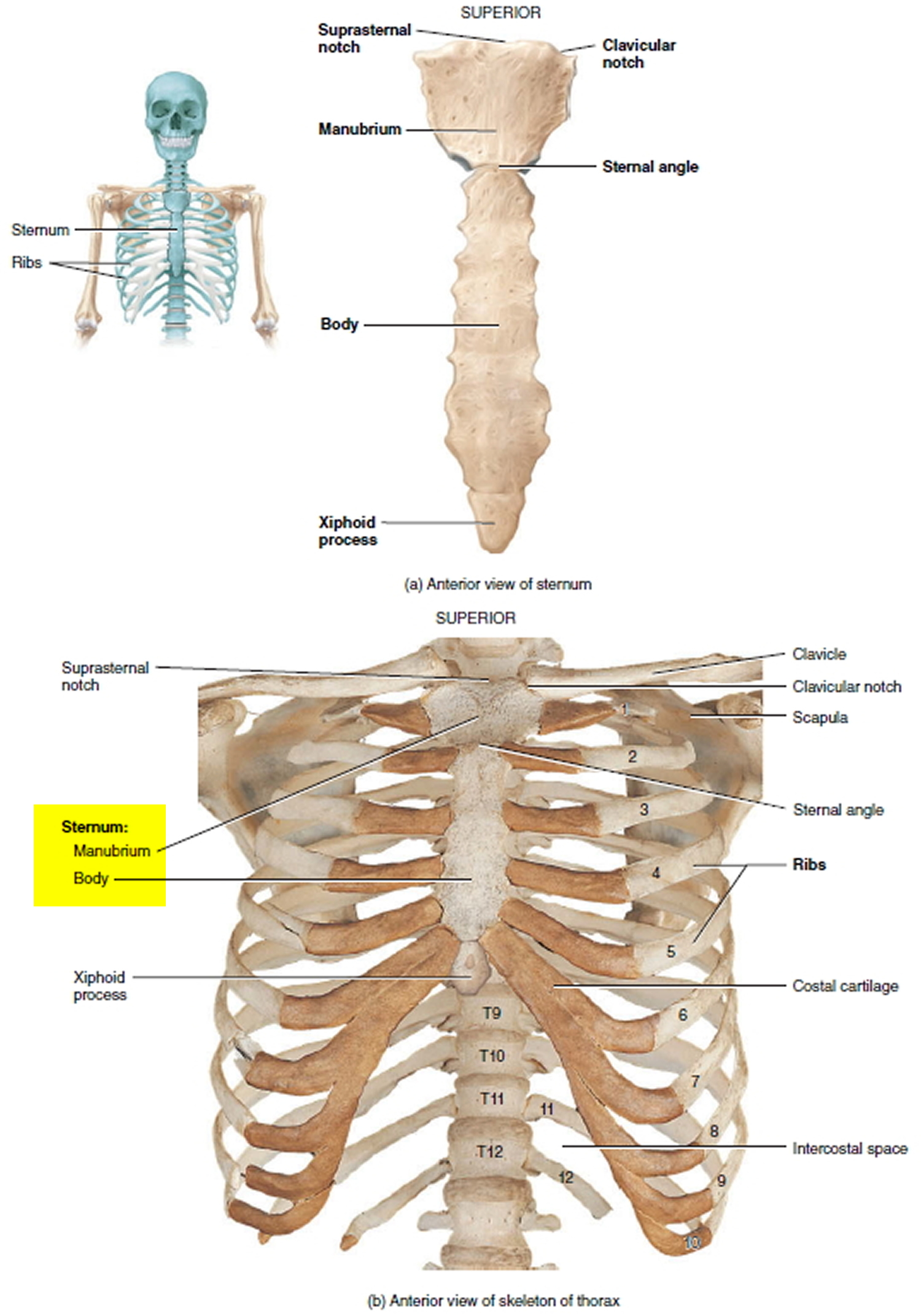
Figure 3. Important organs behind the sternum
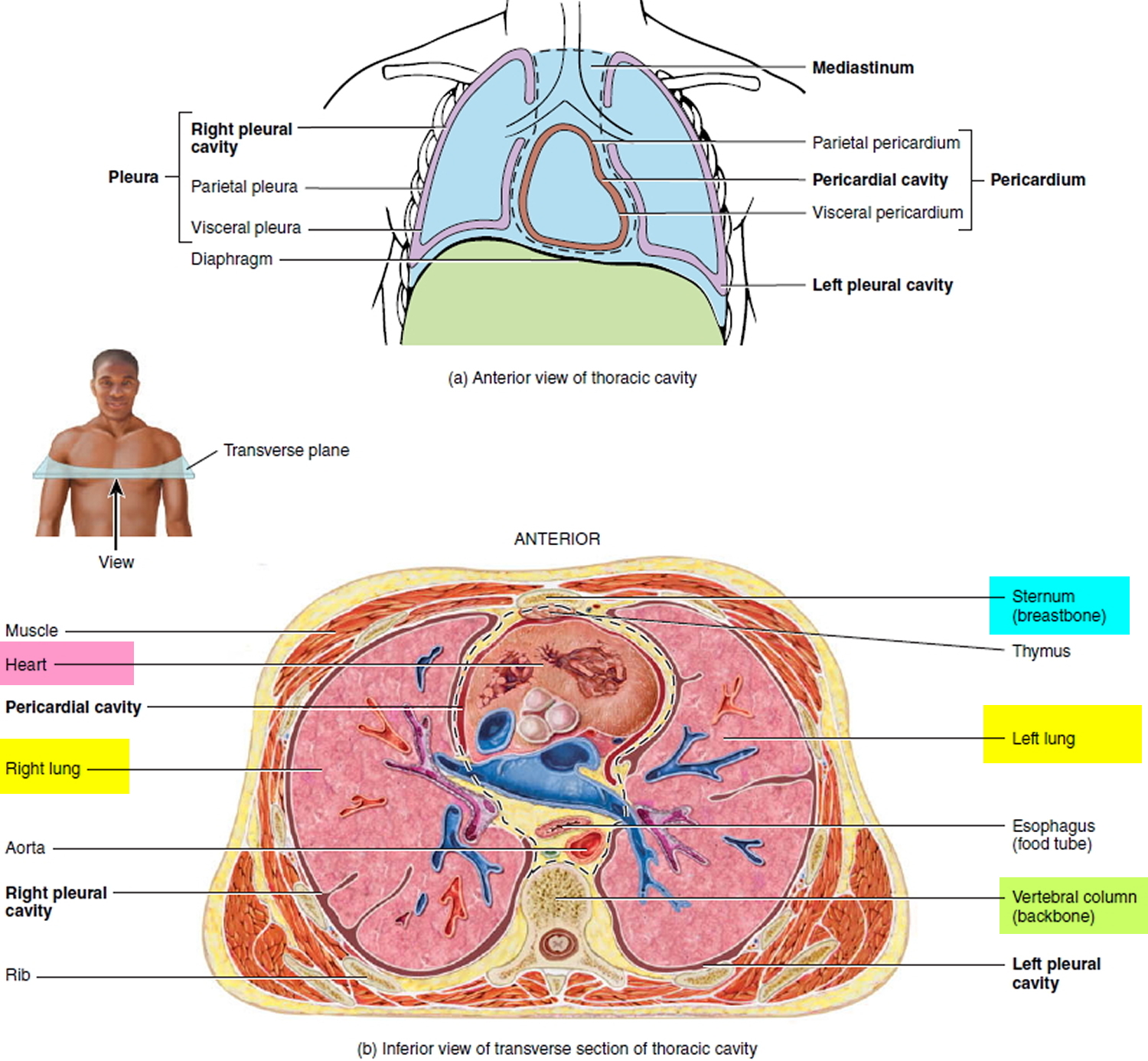
Table 1. Costochondritis vs Tietze Syndrome
| Feature | Tietze syndrome | Costochondritis |
|---|---|---|
|
Prevalence |
Rare |
More common |
|
Age |
Younger than 40 years |
Older than 40 years |
|
Number of sites affected |
One (in 70 percent of patients) |
More than one (in 90 percent of patients) |
|
Costochondral junctions most commonly affected |
Second and third |
Second to fifth |
|
Local swelling |
Present |
Absent |
How long does costochondritis last?
Costochondritis may improve on its own after a few weeks, although it can last for several months or more. The condition doesn’t lead to any permanent problems, but may sometimes relapse.
If you have chest pain, you should seek emergency medical attention to rule out life-threatening causes such as a heart attack.
Call your local emergency number for an ambulance.
Costochondritis causes
What causes costochondritis
Costochondritis usually has no clear cause. Occasionally, however, costochondritis may be caused by:
- Injury. A blow to the chest is one example.
- Physical strain. Heavy lifting, strenuous exercise and severe coughing have been linked to costochondritis.
- Arthritis. Costochondritis might be linked to specific problems, such as osteoarthritis, rheumatoid arthritis or ankylosing spondylitis.
- Joint infection. Viruses, bacteria and fungi — such as tuberculosis, syphilis and aspergillosis — can infect the rib joint. Respiratory tract infections can also cause costochondritis.
- Infections after surgery or from IV drug use
- Tumors. Noncancerous and cancerous tumors can cause costochondritis. Primary cancers of the rib, lung, pleura, and muscle or cancer might travel to the joint from another part of the body, such as the breast, thyroid or lung 12).
Risk factors for costochondritis
Costochondritis occurs most often in women and in people older than 40.
Tietze syndrome usually occurs in teenagers and young adults, and with equal frequency in men and women.
Costochondritis symptoms
The symptoms may develop gradually or start suddenly.
The pain associated with costochondritis usually:
- Occurs on the left side of your breastbone
- Is sharp, aching or pressure-like
- Affects more than one rib
- Worsens when you take a deep breath, sneeze or cough
- Gets worse if you move
- If you put pressure on your chest by using a tight seatbelt or hugging someone.
Costochondritis is sometimes confused with a rare condition called Tietze syndrome, which has similar symptoms but also causes chest swelling.
- Costochondritis might feel like you’re having a heart attack. If you are in doubt, see your doctor as soon as possible. If you have chest pain and have trouble breathing, feel sick or are sweaty, dial your local emergency number for an ambulance.
Pain that is reproduced by palpation of the typically affected areas suggests costochondritis, but depends on the exclusion of underlying causes (Table 1) 21,2,7,8,12,16-20). Although pain reproduced by chest wall palpation is considered atypical for a cardiac cause, it does not exclude it. In a study of costochondritis in an emergency department, 6 percent of patients with pain reproduced by chest wall palpation were also diagnosed with myocardial infarction, compared with 27 percent of the control group who had chest pain without pain to palpation.1 In another study of noncardiac chest pain in an emergency department, almost 3 percent of patients had adverse coronary events at 30 days follow-up.21
Table 1. Differential Diagnosis and Treatment of Chest Wall Conditions
| Condition | Diagnostic considerations | Treatment principles |
|---|---|---|
|
Arthritis of sternoclavicular, sternomanubrial, or shoulder joints |
Tenderness to palpation of specific joints of the sternum; evidence of joint sclerosis can be seen on radiography |
Analgesics, intra-articular corticosteroid injections, physiotherapy 13) |
|
Costochondritis |
Tenderness to palpation of costochondral junctions; reproduces patient’s pain; usually multiple sites on same side of chest 14) |
Simple analgesics; heat or ice; rarely, local anesthetic injections or steroid injections 15) |
|
Destruction of costal cartilage by infections or neoplasm |
Bacterial or fungal infections or metastatic neoplasms to costal cartilages; infections seen postsurgery or in intravenous drug users; chest computed tomography imaging useful to show alteration or destruction of cartilage and extension of masses to chest wall; gallium scanning may be helpful in patients with infection |
Antibiotics or antifungal drugs; surgical resection of affected costal cartilage; treatment of neoplasm based on tissue type 16) |
|
Fibromyalgia |
Symmetric tender points at second costochondral junctions, along with characteristic tender points in the neck, back hip, and extremities, and widespread pain 17) |
Graded exercise is beneficial; cyclobenzaprine (Flexeril), antidepressants, and pregabalin (Lyrica) may be beneficial |
|
Herpes zoster of thorax |
Clusters of vesicles on red bases that follow one or two dermatomes and do not cross the midline; usually preceded by a prodrome of pain; postherpetic neuralgia is common |
Oral antiviral agents (e.g., acyclovir [Zovirax], famciclovir [Famvir], valacyclovir [Valtrex]); analgesics as needed for pain; may require narcotics or topical lidocaine patches (Lidoderm) to control pain |
|
Painful xiphoid syndrome |
Tenderness at sternoxiphoid joint or over xiphoid process with palpation 18) |
Usually self-limited unless associated with congenital deformity of xiphoid; analgesics; rarely, corticosteroid injections 19) |
|
Slipping rib syndrome |
Tenderness and hypermobility of anterior ends of lower costal cartilages causing pain at lower anterior chest wall or upper abdomen; diagnosis by “hooking maneuver”: curving fingers under costal margin and gently pulling anteriorly—a “click” and movement is felt that reproduces patient’s pain 20) |
Rest, physiotherapy, intercostal nerve blocks; or, if chronic and severe: surgical removal of hypermobile cartilage segment 21) |
|
Tietze syndrome |
A single tender and swollen, but nonsupportive costochondral junction; usually in costochondral junction of ribs two or three 22) |
Simple analgesics; usually self-limiting; rarely, corticosteroid injections 23) |
|
Traumatic muscle pain and overuse myalgia |
History of trauma to chest or recent new onset of strenuous exercise to upper body (e.g., rowing); may be bilateral and affecting multiple costochondral areas; muscle groups may also be tender to palpation 24) |
Simple analgesics; refrain from doing or reduce intensity of strenuous activities that provoke pain 25) |
[Source 26)]
Costochondritis diagnosis
During the physical exam, your doctor will feel along your breastbone for areas of tenderness or swelling. The doctor may also move your rib cage or your arms in certain ways to try to trigger your symptoms.
The pain of costochondritis can be very similar to the pain associated with heart disease, lung disease, gastrointestinal problems and osteoarthritis. While there is no laboratory or imaging test to confirm a diagnosis of costochondritis, your doctor might order certain tests — such as an electrocardiograph (ECG), X-ray, CT or MRI — to rule out other conditions.
Costochondritis treatment
Costochondritis often gets better after a few weeks, but self-help measures and medication can manage the symptoms.
Treatment for costochondritis focuses on pain relief.
Medications
Your doctor might recommend:
- Nonsteroidal anti-inflammatory drugs (NSAIDs). Although certain medications, such as ibuprofen (Motrin IB) or naproxen sodium (Aleve) are available over the counter, your doctor might prescribe stronger varieties of these nonsteroidal anti-inflammatory medications. Side effects might include damage to your stomach lining and kidneys.
- Narcotics. If your pain is severe, your doctor might prescribe medications containing codeine, such as hydrocodone/acetaminophen (Vicodin, Norco) or oxycodone/acetaminophen (Tylox, Roxicet, Percocet). Narcotics can be habit-forming.
- Antidepressants. Tricyclic antidepressants, such as amitriptyline, are often used to control chronic pain — especially if it’s keeping you awake at night.
- Anti-seizure drugs. The epilepsy medication gabapentin (Neurontin) also has proved successful in controlling chronic pain.
Physical therapy
Physical therapy treatments might include:
- Stretching exercises. Gentle stretching exercises for the chest muscles may be helpful.
- Nerve stimulation. In a procedure called transcutaneous electrical nerve stimulation (TENS), a device sends a weak electrical current via adhesive patches on the skin near the area of pain. The current might interrupt or mask pain signals, preventing them from reaching your brain.
Transcutaneous electrical nerve stimulation (TENS) is a method of pain relief where a mild electric current is delivered to the affected area using a small, battery-operated device. The electrical impulses can reduce the pain signals going to the spinal cord and brain, which may help relieve pain and relax muscles. They may also stimulate the production of endorphins, which are the body’s natural painkillers. Although TENS may be used to help relieve pain in a wide range of conditions, it doesn’t work for everyone. There isn’t enough good-quality scientific evidence to say for sure whether TENS is a reliable method of pain relief. Speak to your doctor if you’re considering TENS.
Surgical and other procedures
If conservative measures don’t work, your doctor might suggest injecting numbing medication and a corticosteroid directly into the painful joint.
Corticosteroids are powerful medicines that can help reduce pain and swelling. They can be injected into and around your costochondral joint to help relieve the symptoms of costochondritis.
Corticosteroid injections may be recommended if your pain is severe, or if NSAIDs are unsuitable or ineffective.
They may be given by your doctor, or you may need to be referred to a specialist called a rheumatologist.
Having too many corticosteroid injections can damage your costochondral joint, so you may only be able to have this type of treatment once every few months if you continue to experience pain.
Home remedies
It can be frustrating to know that there’s little your doctor can do to treat your costochondritis.
Costochondritis can be aggravated by any activity that places stress on your chest area, such as strenuous exercise or even simple movements like reaching up to a high cupboard.
Any activity that makes the pain in your chest area worse should be avoided until the inflammation in your ribs and cartilage has improved.
You may also find it soothing to regularly apply heat to the painful area – for example, using a cloth or flannel that’s been warmed with hot water.
Self-care measures might make you feel more comfortable. They include:
- Over-the-counter nonsteroidal anti-inflammatory drugs pain relievers. Ask your doctor about using ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve, others).
- Heat or ice. Try placing hot compresses or a heating pad on the painful area several times a day. Keep the heat on a low setting. Ice also might be helpful.
- Rest. Avoid activities that make your pain worse.
References [ + ]





{kind=link}