Contents
Cecostomy
Cecostomy is surgery to clear a child’s bowels of feces when other treatment has not worked. Cecostomy is used for children with fecal incontinence caused by major health problems. Fecal incontinence means your child can’t control his or her bowels. Symptoms can range from having severe constipation to having a bowel movement at an unexpected or embarrassing time.
Cecostomy is different from an enema that is used to ease constipation. An enema is given directly through the rectum to help free the feces. In a cecostomy, the healthcare provider puts a tube (catheter) into the first part of the large intestines (cecum). It is in the lower right abdomen. The provider injects liquid medicine into the cecum through this tube. The medicine helps coax the feces out of the body through the rectum.
A cecostomy tube (C-tube) is a thin plastic tube that is placed through the opening on the abdomen and directly into the cecum (first part of the large intestine) to help your child empty their bowel and to decrease the incidence of fecal incontinence (soiling). A cecostomy tube is inserted by an interventional radiologist using image guidance. For the first 10 days after the cecostomy tube insertion, your child should not use the cecostomy tube and will continue with their regular bowel regime. When the doctor inserts the cecostomy tube into your child’s cecum, they will also insert a small piece of medical wire attached to a thread (retention suture). You will have an appointment to have the retention suture removed.
Cecostomy tubes can help patients who have issues such as fecal incontinence (soiling) and severe constipation to be independent in their bowel management.
Putting the cecostomy tube in place is just the first step in easing fecal incontinence. After about a week, you will give your child an enema through the cecostomy tube at home, with guidance from your child’s doctor. This process will involve putting liquid into the cecostomy tube. This liquid will pass into the cecum to encourage a bowel movement. This is called an antegrade enema. Usually an enema is given by placing liquid into the rectum to help empty the bowel. This is called a retrograde enema. However, for an antegrade enema to be successful, it will require a lot of time and patience from the patient and their family. For this reason, getting a cecostomy tube is not an option for all patients.
Your child will likely need to have the catheter removed and replaced from time to time. It will have to be done for hygiene reasons and to lower the risk for complications.
See your child’s doctor if your child has any of the following:
- A noticeable skin infection at the catheter site
- Bleeding or swelling at the site
- Pus leaking from the site
- The tube becomes dislodged or moves
- Abdominal pain
- Fever
Figure 1. Cecostomy tube
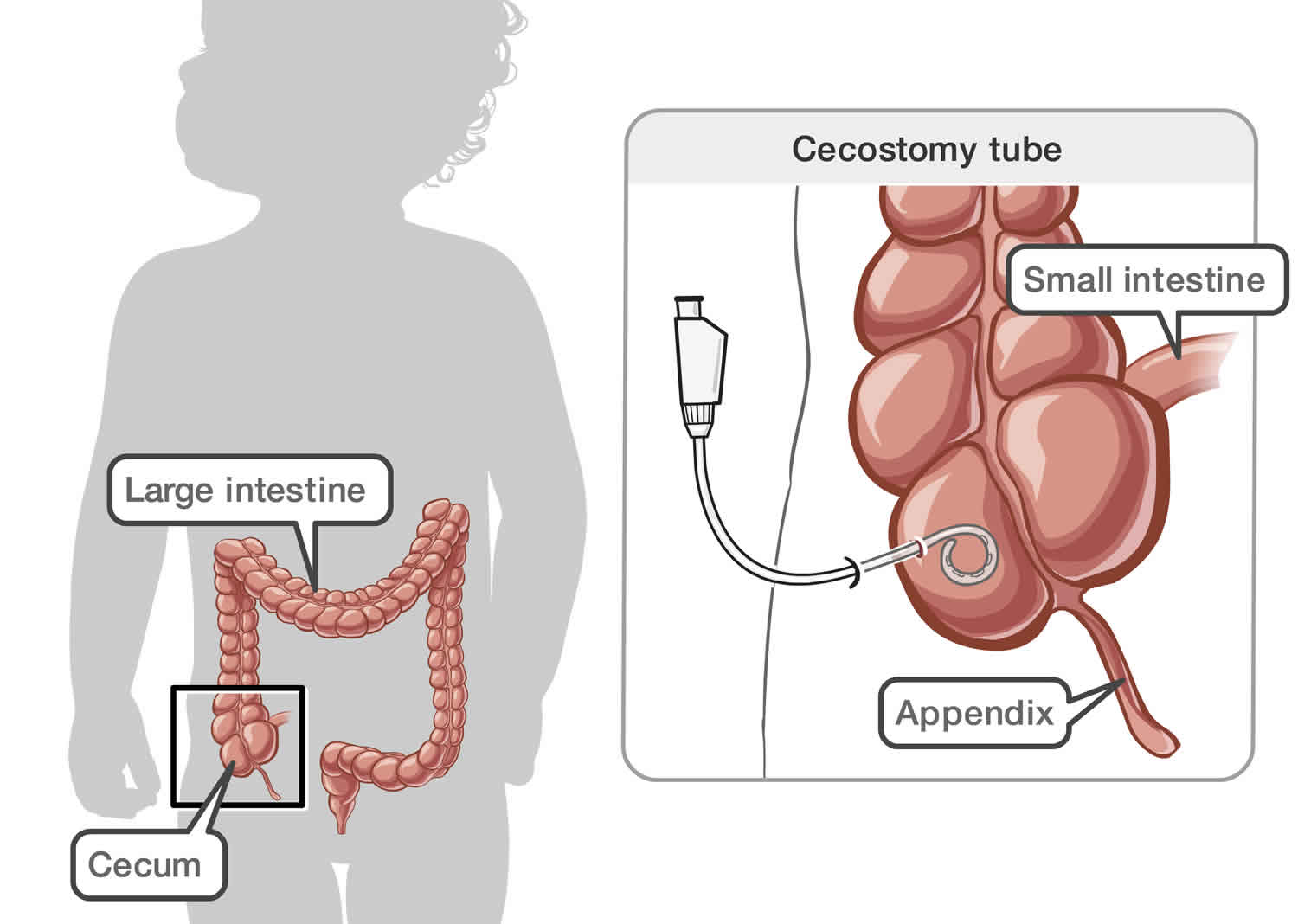
Footnote: A cecostomy tube (C-tube) is a thin plastic tube that is placed through an opening on the abdomen directly into the cecum to help your child empty their bowel. At first a temporary C-tube will be inserted. After six weeks, a long-term Chait trapdoor cecostomy tube will replace the temporary one.
Cecostomy tube uses
Your child may need a cecostomy if he or she has fecal incontinence and other treatments have not worked. But most children with this health problem will have success with other treatments.
Your child may be a candidate for a cecostomy tube if they:
- experience fecal incontinence with troublesome soiling.
- have experienced long-term severe constipation.
- do not respond well to rectal enemas or other methods.
Your child may also need the cecostomy procedure if he or she has any of the following:
- The anus isn’t letting feces pass as it should (imperforate anus)
- Spinal problems, such as spina bifida
- A combination of the above 2 health problems
- Other muscular problems
Your child may NOT be a candidate for a cecostomy tube if they:
- have had previous abdominal surgery.
- have excessive soft tissue between the skin surface and the cecum.
- are unable to sit for a prolonged period of time on the toilet.
Cecostomy procedure
Your child will need to stay in the hospital for the procedure to insert the cecostomy tube. The stay often lasts 1 to 2 days. Most of the time, the procedure will go as follows:
- Your child will get medicine through an IV (intravenous) line that helps him or her relax during the procedure. Your child may be put to sleep with general anesthesia.
- A healthcare provider usually inflates the colon with air until the cecum is expanded.
- Your doctor puts surgical tools through small cuts (incisions) in the skin and into the cecum. He or she attaches the bowel to the abdominal wall with stitches, sutures, or fasteners.
- Your doctor puts a special hollow needle into the cecum.
- Your doctor threads the catheter through this needle and into the cecum.
This procedure can also be done with a laparoscope. With this technique, the healthcare provider puts a laparoscope into a small incision in the belly button.
The process outlined above is what is done to insert the cecostomy tube. The cecostomy itself will then be done occasionally to relieve the bowels based on your child’s needs.
Preparing for the cecostomy procedure
Your child will have a clinic visit in the interventional radiology department before the procedure. This visit will usually take about two hours.
During the clinic visit you should expect:
- A health and nutrition history and a physical examination will be performed by the clinic nurse and registered dietician.
- An explanation of the procedure, and a review of the consent form with the interventional radiologist.
- A review of fiber and fluid intake with the registered dietician.
- Information on how to care for and use a C- tube with the clinic nurse.
- Information on transition of care from a pediatric institution to an adult facility that would be begin at 16 years of age.
It is important that your child is healthy on the day of the procedure. If your child starts to feel unwell or has a fever within two days before the cecostomy tube insertion, let your doctor know. Your child’s procedure may need to be rebooked.
Food, drink, and medicines before the procedure
Your doctor will tell you if your child will be required to clear their bowel beginning two days prior to the cecostomy tube insertion. If required, the bowel is cleared in the following way for a cecostomy tube insertion:
- Two days before the procedure your child will start a clear fluid diet. They cannot have any solid food or milk during this time. Your child will continue a clear fluid diet until after the procedure and until the doctors tell you that it is alright to for them to eat solid food. If your child has special needs during fasting, please talk to your referring doctor in advance. Your child may need to be admitted to the hospital for a bowel washout.
- Clear fluids include:
- chicken, beef or other clear broth (without noodles)
- clear apple juice
- Kool-Aid
- Gatorade
- Pedialyte
- ginger ale
- popsicles
- water
- Clear fluids include:
- Your child will also need to take a medication called Pico-Salax to help clear their bowel before the procedure. Ask your referring doctor or the clinic nurse for instructions on how and when your child will need to take the medication.
- After your child develops nearly clear rectal outflow, they should continue drinking clear fluids. This is important to prevent dehydration. Your child can have clear fluids up to three hours prior to the booked procedure time.
- On the day of the procedure please give your child their regular morning medicines with a sip of water.
- Medicines such as acetylsalicylic acid (ASA), naproxen or ibuprofen, warfarin or enoxaparin may increase the risk of bleeding. Do not give these to your child before the procedure unless they have been cleared first by their doctor and the interventional radiologist.
During the cecostomy tube insertion procedure
Children will have a general anaesthesia for cecostomy tube insertion.
At first, a temporary cecostomy tube is inserted through your child’s abdomen, into the cecum. A small hole is made in your child’s abdomen (most of the time on the right lower abdomen). The temporary cecostomy tube is then inserted using ultrasound and X-ray to guide it into the correct position in the cecum. The entire procedure takes 60 to 90 minutes. This temporary tube is straight with a curly end, like a pig’s tail, that keeps it in place. One or two small pieces of medical wire attached to a thread, called a retention suture, are used to hold the cecum close to the abdominal wall. This retention suture stays in for two weeks while the cecostomy tube tract heals. The temporary tube will remain 3 to 4 inches outside of the body and is fastened to the skin with tape. A dressing will cover the insertion site for two weeks after the procedure. About six weeks after the temporary cecostomy tube is inserted it will be replaced with a long-term Chait trapdoor cecostomy tube.
After the cecostomy tube insertion
Once the cecostomy tube insertion is complete, your child will be moved to the recovery area. The interventional radiologist will come and talk to you about the details of the procedure. As soon as your child starts to wake up, a nurse will come and get you. Your child will be closely monitored and medication for pain will be given when needed.
Your child may also need a contrast study. This test makes sure that the catheter is placed properly. For it, the healthcare provider injects contrast dye through the tube and into the cecum. Then the provider uses an X-ray to look at the dye to make sure that it travels into the cecum.
Going home
Your child will stay in hospital for three to five days after they have had a cecostomy tube inserted. Your child can go home when the doctor feels it is safe for them to do so. Further teaching and instruction on how to use and care for the cecostomy tube will be provided prior to your child’s discharge home.
During the first two weeks after the procedure, your child should not go into the water and they should avoid taking a bath or going swimming. After two weeks, the retention suture will be cut (this is a painless procedure) and the skin around the cecostomy tube will be assessed. Further support will also be provided to you and your child.
About six weeks after the temporary cecostomy tube is inserted, you will return to the interventional radiology department to have the tube replaced with a long-term Chait trapdoor cecostomy tube. This tube is less visible than the temporary cecostomy tube and lies almost flush to the skin. It takes only 15 to 30 minutes and your child will not have to stay in hospital overnight or have a general anaesthetic. These tubes are then changed yearly in the interventional radiology department.
Skin care
The cecostomy tube that is first put in is temporary and there will be a dressing over the insertion site. The cecostomy tube will be secured to the abdomen with a device to prevent it from moving around in the tract. Your child will need to have a dressing covering the insertion site for two weeks until their follow-up appointment. The dressing will need to be changed at least once a day or whenever it gets wet, soiled or loose.
Bowel care
For the first 10 days after the cecostomy tube insertion, your child should not use the cecostomy tube and continue with their usual bowel cleansing routine as per their doctor’s recommendations.
The cecostomy tube site takes approximately 10 days to heal. Starting on day 11, your child will begin using the cecostomy tube for regular bowel irrigations. During the first few weeks, you may need to make adjustments to the time you do the bowel irrigations and how you do them.
Cecostomy tube flush
For the first 10 days, you will need to flush the temporary cecostomy tube with 10 mL of normal saline twice a day to ensure the tube does not become blocked.
To make saline you will need:
- a large container
- table or kosher salt
- tap water (unboiled) room temperature or warm
Recipe: 2 cups (500 mL) water + 1 teaspoon of salt
You can make larger volumes of this recipe to help save you time. The saline solution can be kept on your counter top for four hours, or stored in the fridge for four days.
Cecostomy tube placement risks
Cecostomy tube insertion is a low-risk procedure. The risk may increase depending on your child’s condition, age and health.
The risks of a cecostomy tube insertion include:
- pain and discomfort
- bleeding and irritation at the tube site
- infection of the skin around the site where the tube was inserted, in the abdomen (peritonitis) caused by misplacing the catheter or a generalized infection in the body. If your child has a VP shunt, there is a risk of shunt or brain infection
- granulation tissue (growth of tissue at the tube site)
- bowel damage requiring surgery
- the cecostomy tube (catheter) gets displaced
- mechanical failure of the cecostomy tube.
Cecostomy tube common problems
Cecostomy tube moves
If the cecostomy tube looks longer or shorter, it may have moved. This can happen because the cecostomy tube comes in three sizes (small, medium, long), and often children are in between sizes. If the tube is sitting high off the skin, you can push it back in. If there is resistance when you try to push it back in, there may be a coil in the tract. This is not an emergency, but your child should be assessed in the interventional radiology department.
Cecostomy tube gets blocked
To unblock your child’s temporary cecostomy tube, you will need:
- a 10 mL syringe
- warm water
- Fill a 10 mL syringe with warm water.
- Connect the syringe to the end of the cecostomy tube.
- Push and pull on the plunger of the syringe to move the liquid in and out of the cecostomy tube. That will help clear out any fecal material that might be in the way. You may have to try this a few times before the cecostomy tube is no longer blocked.
- When the cecostomy tube is no longer blocked, fill the syringe with 10 mL of water and push it into the tube.
- Take the syringe off the cecostomy tube and close it up.
If you are not able to unblock the temporary cecostomy tube, or your child’s trapdoor is blocked you will need to have the tube replaced in the interventional radiology department on the next working day. Call the clinic to arrange this.
Making saline solution for bowel irrigation
You can easily make saline to use for your child’s irrigation. To make saline you will need:
- a large container
- table or kosher salt
- tap water (unboiled) room temperature or warm
Recipe: 2 cups (500 mL) water + 1 teaspoon of salt
You can make larger volumes of this recipe to help save you time. The saline solution can be kept on your counter top for four hours, or stored in the fridge for four days.
How much saline and glycerin should I use for my child?
All children should cleanse their bowel with a saline solution either every day or every other day. Each child is different and will need different amounts of fluids for irrigation. For children that have hard stools, glycerin can be added to the saline solution. Talk to your doctor if you think your child needs this. The amount of saline and glycerin that your child will need depends on two things; how constipated they are and their weight. If you do not know how much saline or glycerin to use, please call your clinic during working hours and ask to speak to a nurse.
- The recommended amount of saline for your child is: 10–20 mL/kg per flush.
- The recommended amount of glycerin for your child is: 0.5–1.0 mL/kg/dose (max dose 60 mL/day.
It is important to remember that as your child grows and gains weight, they will need more saline and glycerin to cleanse their bowel.
What to do if nothing comes out in the toilet after you flush the bowel?
Often irrigating the bowel can take a long time. For most children, it takes 45 to 60 minutes to flush out their bowels.
If you irrigate your child’s bowel and nothing comes out after an extended period of time, your child may have a blockage in their bowel. There are several things you can try to unblock your child’s bowel.
- Massage your child’s abdomen clockwise to help the fluid move through.
- Have your child move around to help encourage the fluid to pass.
If your child is having a lot of cramping or discomfort and is having difficultly passing fluid, they should be seen by their doctor or go to the nearest Emergency Department. Your child may need a physical assessment and possibly an abdominal X-ray to see if they have a blockage of stool.
What do I do if my child is having accidents in between flushes?
Accidents can be caused by a number of things. Your child might:
- be constipated
- need a change to their diet and fluid intake
- have an infection
- need a change to their irrigation regime
- need a stool softener or bulking agent
If your child is having accidents in between flushes, call your doctor, the service who referred you or your clinic nurse during working hours to help sort out the cause of accidents. Your child may need to have some tests done if changes to their diet, regime and bulking agents do not help solve the problem.
Cecostomy tube falls out or gets pulled out
If your child’s cecostomy tube falls out, try to insert a Foley catheter to keep the hole to your child’s intestine open until a new cecostomy tube can be put in. The first six weeks after your child first gets their cecostomy tube is the most important time for healing. If your child’s cecostomy tube falls out within two weeks of when it was put in, you can try to insert a Foley catheter to stop the hole from closing. This is not an emergency, but the tube needs to be reinserted as soon as possible.
Putting the Foley catheter in when your child’s cecostomy tube comes out
In your supplies, you should have a soft tube called a Foley catheter. It will be one size smaller than your child’s cecostomy tube. Try to put the Foley catheter into the hole (opening) following the directions below. The sooner you try to put the Foley catheter into the hole the easier it will be. The longer the tube is out, the smaller the hole will become. If you cannot put the Foley catheter in, call the interventional radiology department during working hours. Go to the emergency department on holidays, weekends or at night.
You will need:
- lubricating jelly
- 8 French Foley catheter
- tape
- catheter plug with a protector cap
- Wash your hands and the skin around your child’s cecostomy gently but thoroughly with soap and water.
- Wet the tip of the catheter with a lubricating jelly such as K-Y Jelly or Muko. DO NOT use petroleum jelly (Vaseline).
- Put the tip of the Foley catheter about 2 or 3 inches (4 to 6 centimeters) into the hole in your child’s abdomen where the cecostomy tube was. Measure the tube against your index finger.
- Tape the Foley catheter to your child’s stomach. Plug it or bend it so stool will not leak out.
- You can use the Foley catheter to give your child their bowel clean-out.
- Call the interventional radiology department on the next working day to make an appointment for a cecostomy tube reinsertion. This is done as an outpatient. Your child will not need to stay overnight in the hospital.
Go to the emergency department if your child has any of the following problems after the Foley catheter is inserted:
- severe pain in the tummy
- sudden high fever
- diarrhea
- severe abdominal distention
Cecostomy tube causing skin problems
After the first 24 hours post-insertion, the cecostomy tube dressing must be changed daily and the skin around the cecostomy tube must be washed with soap and water.
Your child needs a dressing covering the cecostomy site for two weeks.
Red skin
Your child’s skin may get sore and red because of:
- acidic juices from the intestine leaking out around the cecostomy tube
- the cecostomy tube moving around too much in its hole
- an incorrect tube size that may be causing pressure on the skin
- infection
Infection
Your child may have an infection if:
- the skin around the cecostomy tube is redder than usual and redness is spreading
- there is a change in the color and thickness of the liquid leaking around the cecostomy tube
- there is swelling, or you feel warmth around your child’s C- tube or your child is in pain
- your child has a fever
- there is pus draining from the stoma
If your child has any of these signs, call your doctor.
Granulation tissue
Extra tissue that grows around the cecostomy tube is called granulation tissue. Granulation tissue is not harmful. It looks red, moist and may bleed easily when rubbed. The tissue may have yellow sticky drainage. Pressure and friction from the cecostomy tube and moisture around the site may contribute to the growth of granulation tissue. Granulation tissue can be treated at home with saline soaks. Call your family doctor or referring service to request an appointment for treatment. Do not apply any creams directly to the hole.
Protecting your child’s skin
If there is liquid leaking out from around your child’s cecostomy tube that makes the skin burn and feel itchy, then protect the skin with a zinc based barrier cream. Zincofax and Ihles Paste are barrier creams that you can buy in your local drugstore.
How to treat problems with your child’s skin?
If your child has problems with their skin, you can use a warm salt water soak to dry out and soothe the area around the cecostomy tube. Soak the skin with salt water three to four times a day when your child has a skin problem.
To make a salt water soak:
- Measure 1 cup of warm water and 2 teaspoons of table salt in a clean cup or bowl.
- Stir the salt into the warm water until the salt dissolves and disappears.
- Wet a piece of gauze or a strip of a clean cotton face cloth in the warm salt water.
- Place the wet gauze or cloth around the cecostomy tube on the skin of your child’s abdomen. Leave for 30 minutes. Your child needs a salt water soak three to four times a day when they have a problem with their skin. Reduce how often you give your child a salt water soak as their skin heals.
If you have trouble taking the tape off your child’s skin, put a wet face cloth over the tape for a few minutes before you take it off.
It is also very important to make sure that your child’s skin is dried well around and under the cecostomy tube after salt soaks and bathing.





{kind=link}