






Pilomatricoma
Pilomatricoma also called pilomatrixoma and sometimes known as calcifying epithelioma of Malherbe, is an uncommon, harmless, hair follicle tumor derived from hair matrix cells (from the cells at the base of hair follicles) 1). Pilomatricomas are typically found in the head and neck region, but also occur in the upper extremities and are rarely reported in other sites 2). The largest case series in the literature includes 346 pilomatrixomas of which 15.3 percent were observed in the upper extremities 3).
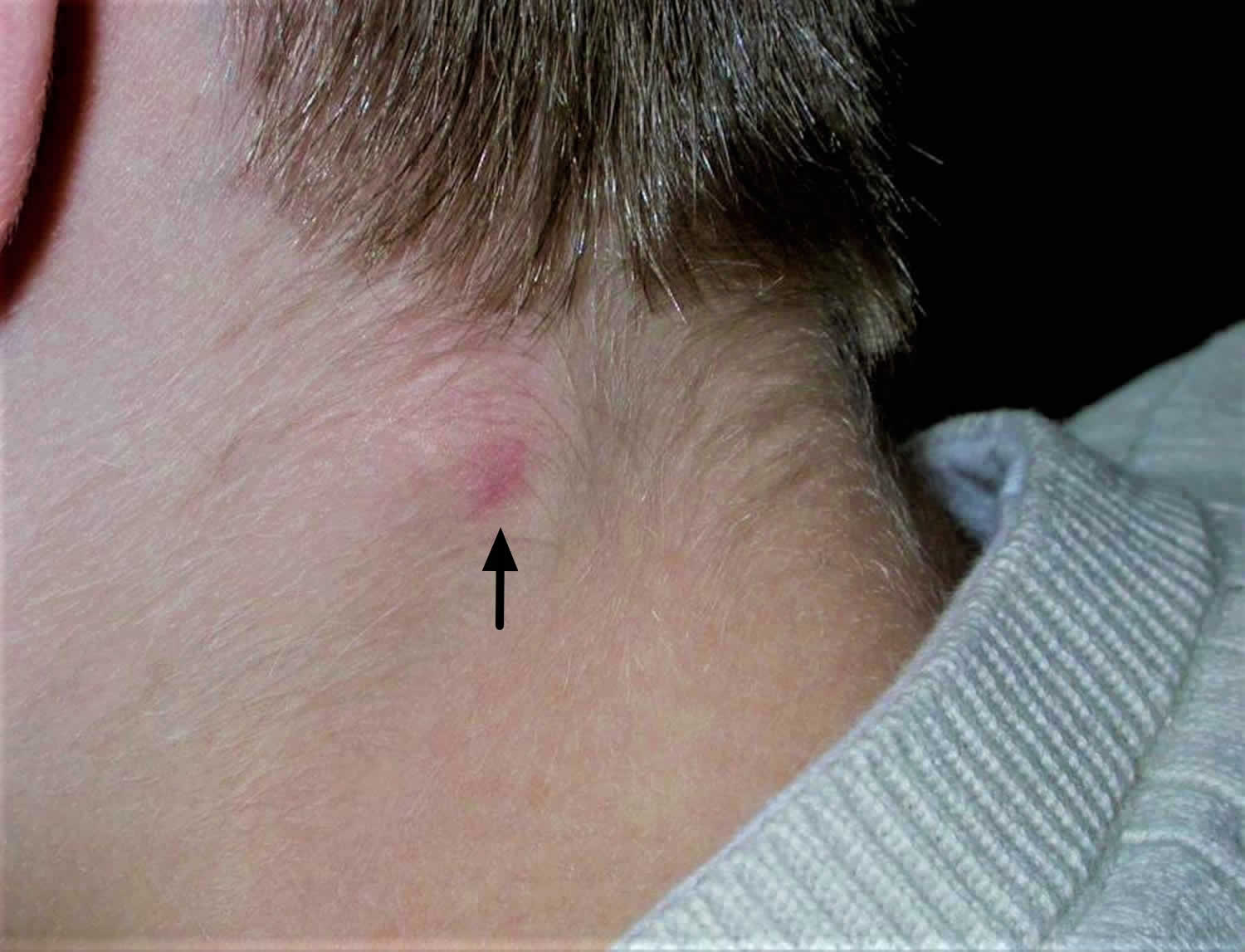
A pilomatricoma normally appears as a single pink or purplish lump containing white areas. The white areas are due to calcium (chalky) deposits and makes the lump feel hard as a bone.
Pilomatricomas are usually less than 3 cm in diameter, although rarely can be larger. They are most common on the head and neck or the upper body in children and teenagers, but can develop anywhere on the body at any age.
Pilomatricoma is most often diagnosed in young children but may also affect adults. Pilomatricoma appears to be slightly more common in females than males.
Your doctor may suspect the diagnosis on examining the skin and may refer you for an ultrasound scan. The diagnosis is confirmed by specialist examination of a small tissue sample (a biopsy – when a tiny piece of skin is removed under local anesthetic).
Figure 1. Pilomatricoma

Can a pilomatricoma be cured?
Yes, if a pilomatricoma is completely removed surgically (cut out or excised), it is considered to be cured. It is very unlikely that they will grow back after being removed. They do not tend to go away by themselves and will either stay the same size or slowly grow over the years.
Pilomatricoma causes
The cause of pilomatricoma is now known to be due to a localized mutation in a hair matrix cell. An overactive proto-oncogene called BCL-2 suggests the normal process of cell death is suppressed, and mutations in CTNNB1 in most cases suggest loss of regulation of a protein complex called beta-catenin or LEF-1.
Are pilomatricomas hereditary?
Most pilomatricomas do not run in families, but very rarely (less than 1 in 100,000) there may be a link to rare (less than 1 in 10,000) genetic disorders.
Pilomatricoma signs and symptoms
A pilomatricoma does not normally cause any symptoms unless it becomes inflamed or infected; when it becomes red and sore. Occasionally the growth may burst and release white and yellow chalky fluid. Pilomatricomas can sometimes be uncomfortable.
Pilomatricoma presents as a single skin-colored or purplish lesion:
- They are usually found on the head and neck, but they may occur on any site.
- They don’t usually cause any symptoms, but they may be tender.
- They may be skin coloured, white or red.
- They may be regular or irregular in shape.
- Most pilomatricomas are 5–10 mm in diameter.
- They may remain stable for years or slowly grow in size up to several centimeters in diameter.
Pilomatricoma is characterized by calcification within the lesion, which makes it feel hard and bony, and often results in an angulated shape (the ‘tent’ sign).
Pilomatricoma complications
Complications of pilomatricoma are rare. However, occasionally they grow to giant size several centimeters in diameter and pilomatrix carcinoma (cancer) has been very rarely reported. Pilomatrix carcinoma is locally aggressive and can recur and approximately 90 cases have been reported in the literature. In several cases, it has demonstrated metastases. Many key features are similar between these benign and malignant counterparts; the primary differentiating characteristics include a high mitotic rate with atypical mitoses, central necrosis, infiltration of the skin and soft tissue, and invasion of blood and lymphatic vessels 4).
A few cases have been reported of multiple pilomatricomas in association with the rare neurological condition myotonic dystrophy. Individual cases have also been reported of pilomatricomas arising in patients with a variety of other genetic disorders. The vast majority are not associated with any other abnormality.
Pilomatricoma diagnosis
If pilomatricoma is suspected, dermoscopy may be helpful, showing a central whitish or grayish-blue structureless area. Erythema and telangiectasia are sometimes observed.
If the nature of the skin lesions is uncertain, ultrasound scan may be recommended. The scan of pilomatricoma is described as a doughnut within the dermis (mid layer of the skin) with a tail (the tail denotes calcification). Alternatively, the calcification may be detected by X-ray.
A biopsy will help to establish the cause of the lesion. Alternatively the whole lesion can be removed, providing both diagnosis and treatment. The histology of pilomatricoma is striking. It may show a sharply demarcated tumor surrounded by a fibrous capsule or a poorly demarcated tumor without capsule. There are darkly stained ‘basophilic’ cells and ‘shadow’ cells with missing nuclei. Calcium deposits are found in most lesions.
Pilomatricoma treatment
Pilomatricomas are usually surgically excised. They do not disappear by themselves, and if incompletely removed, they may recur. The recurrence rate is low, ranging from 0 to 3 percent 5). If a lesion recurs after excision or rapidly enlarges, it should be excised due to malignant potential or possible misdiagnosis.
References [ + ]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}