






Round ligament pain
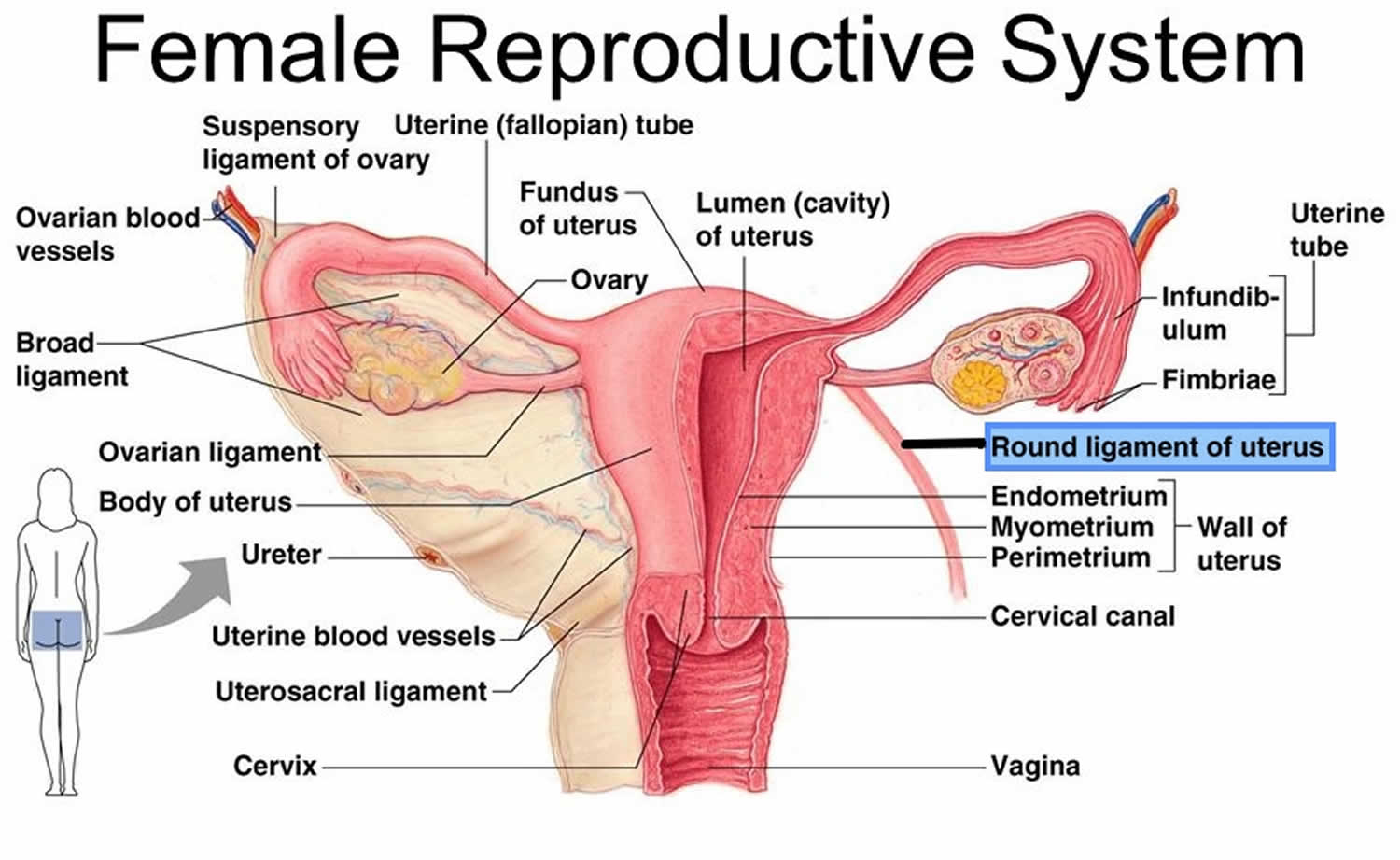
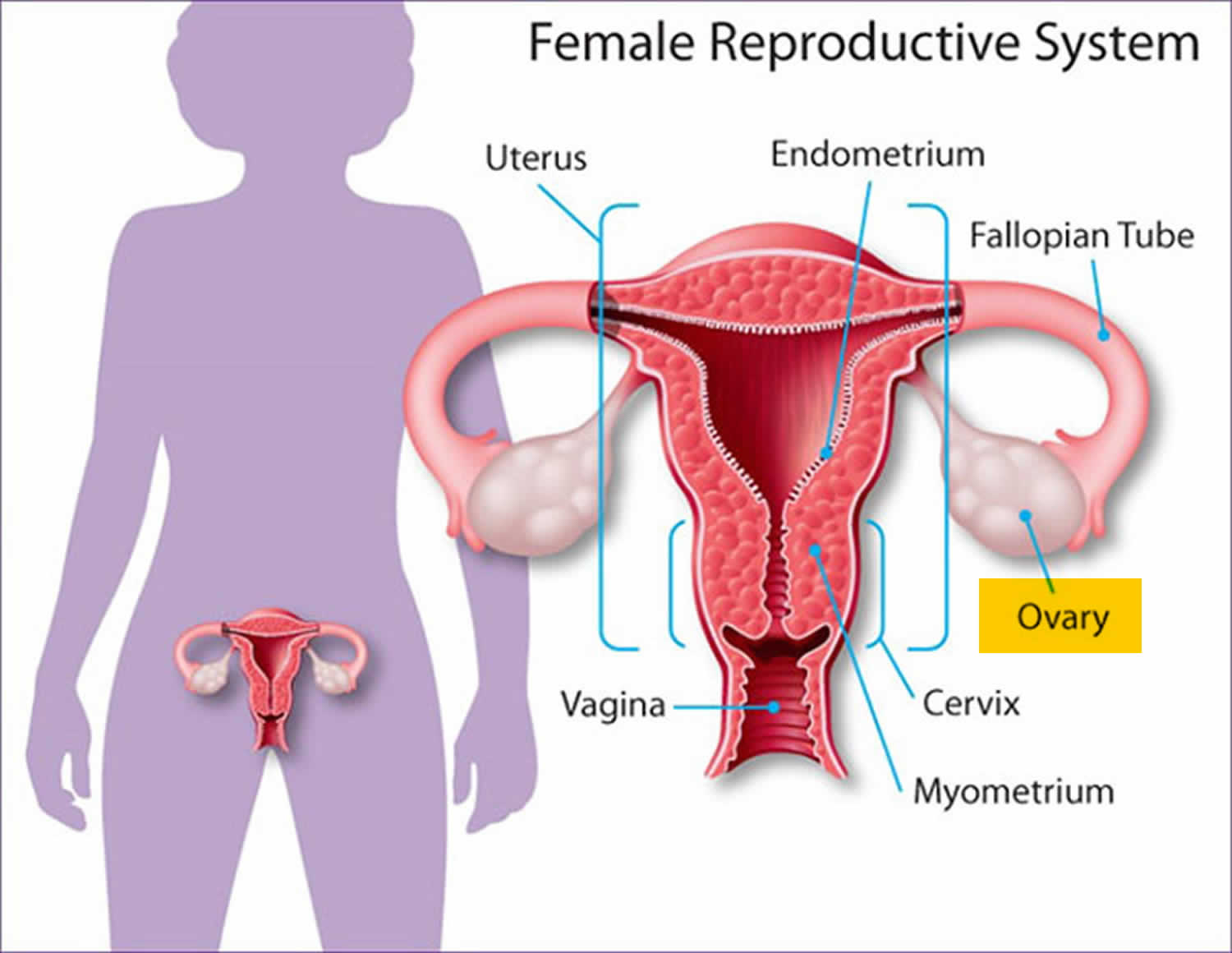
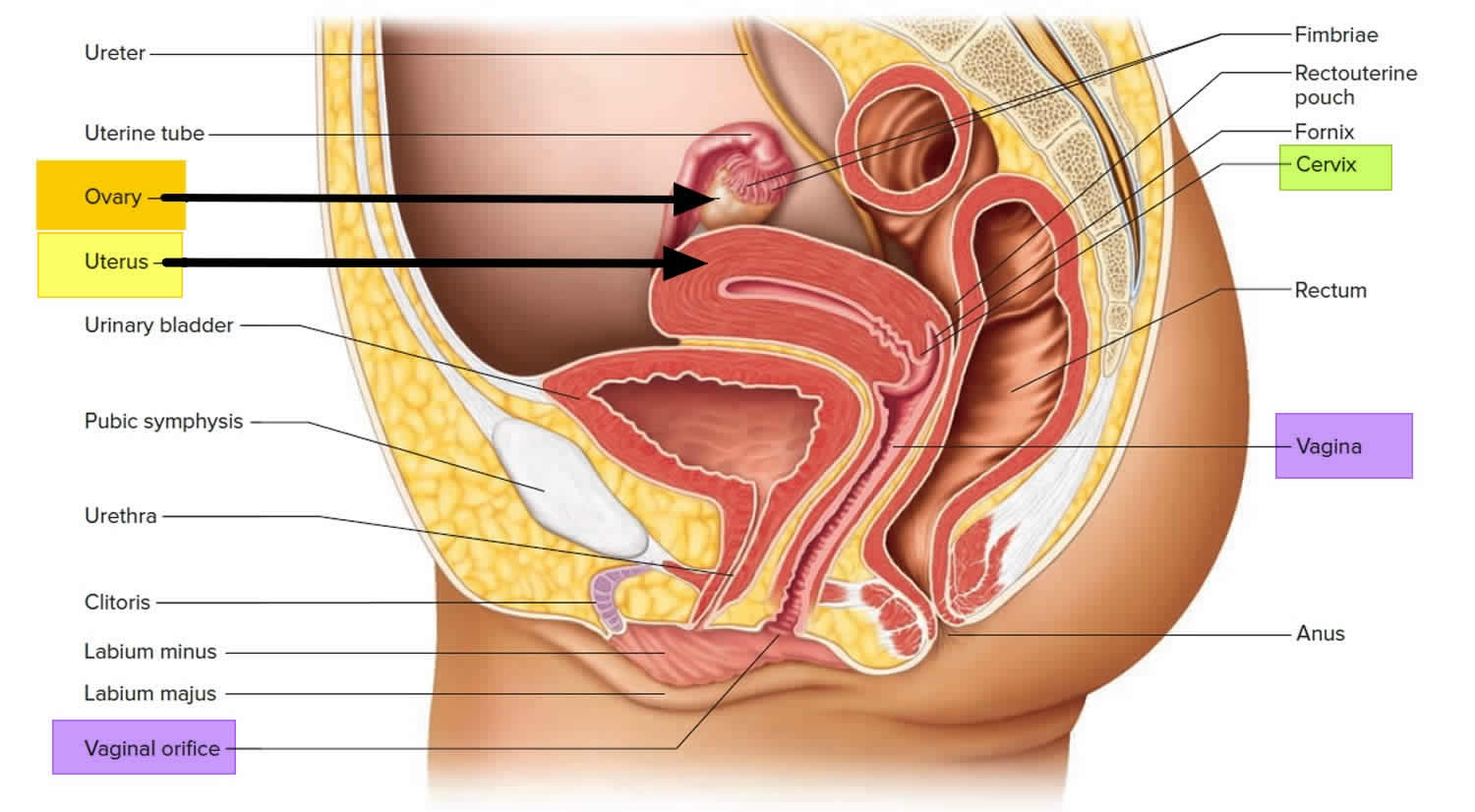
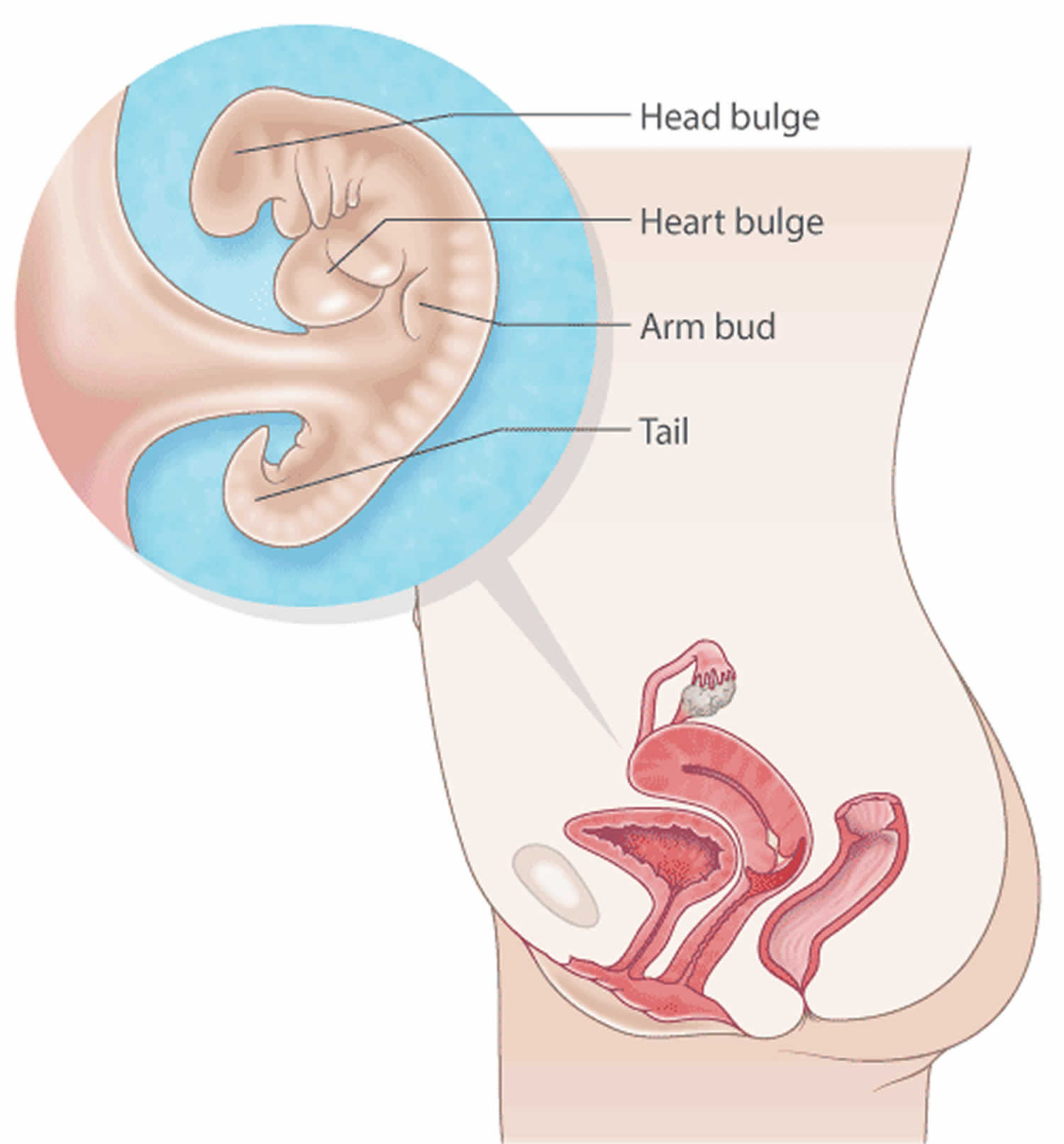
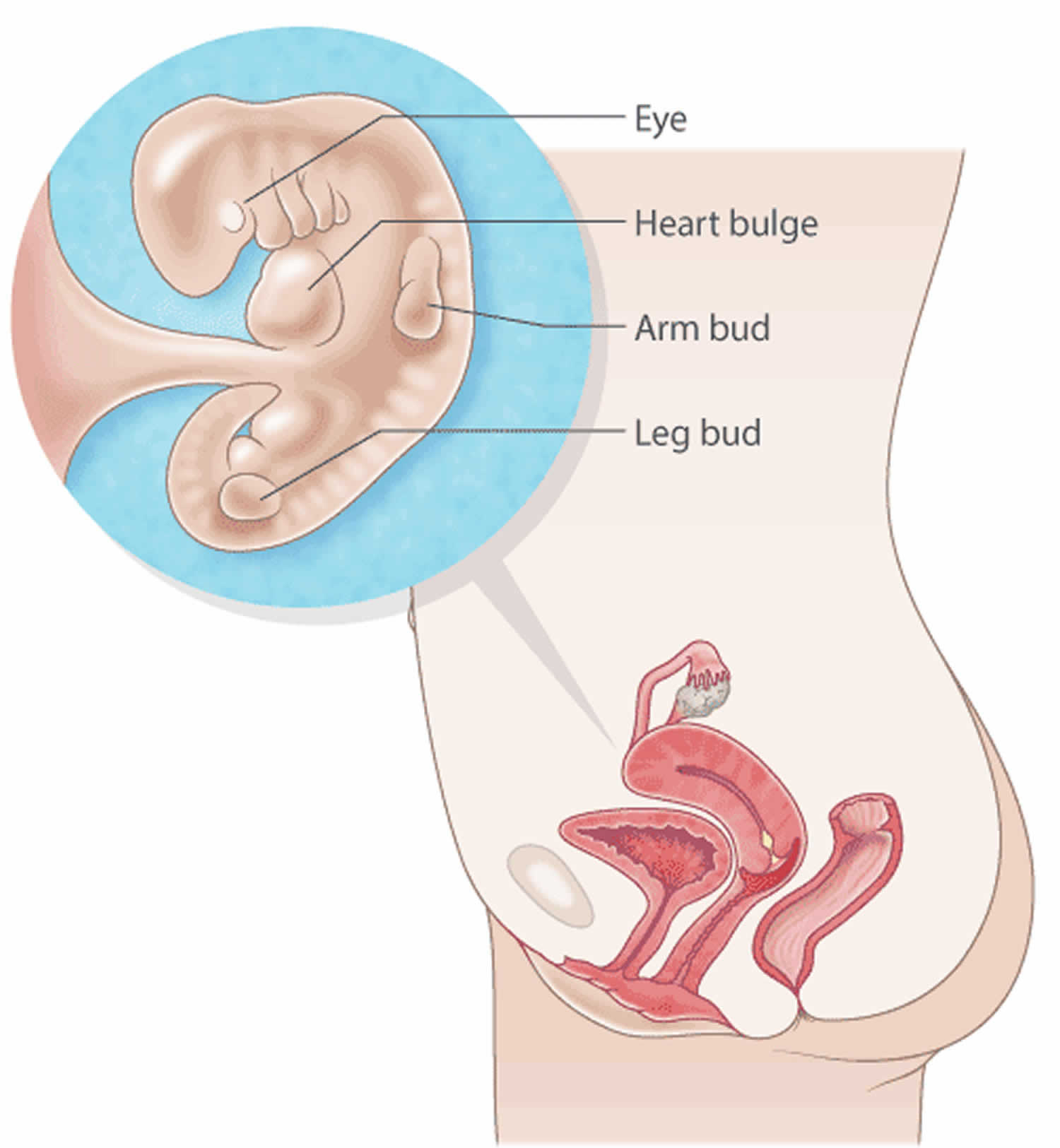
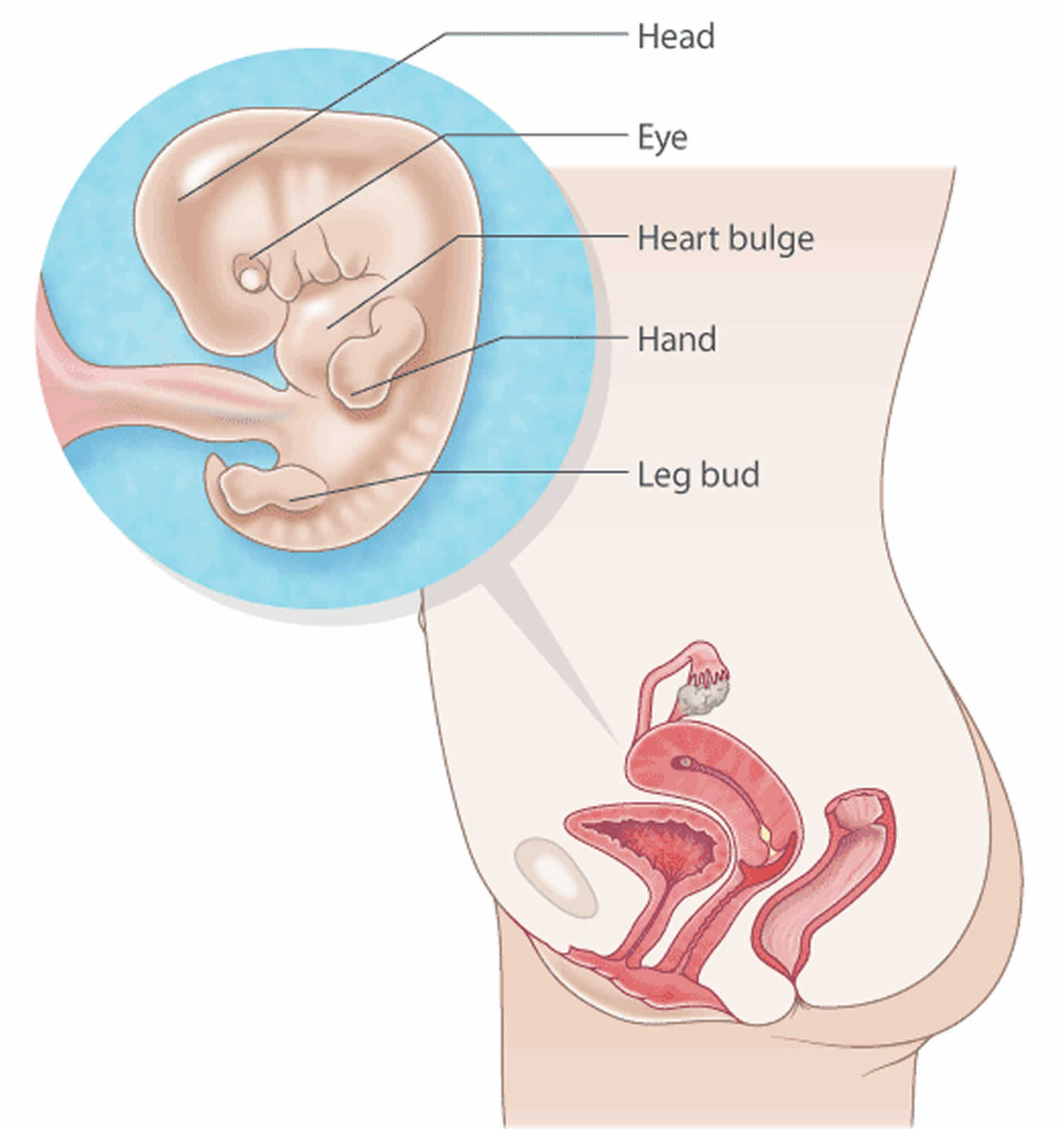
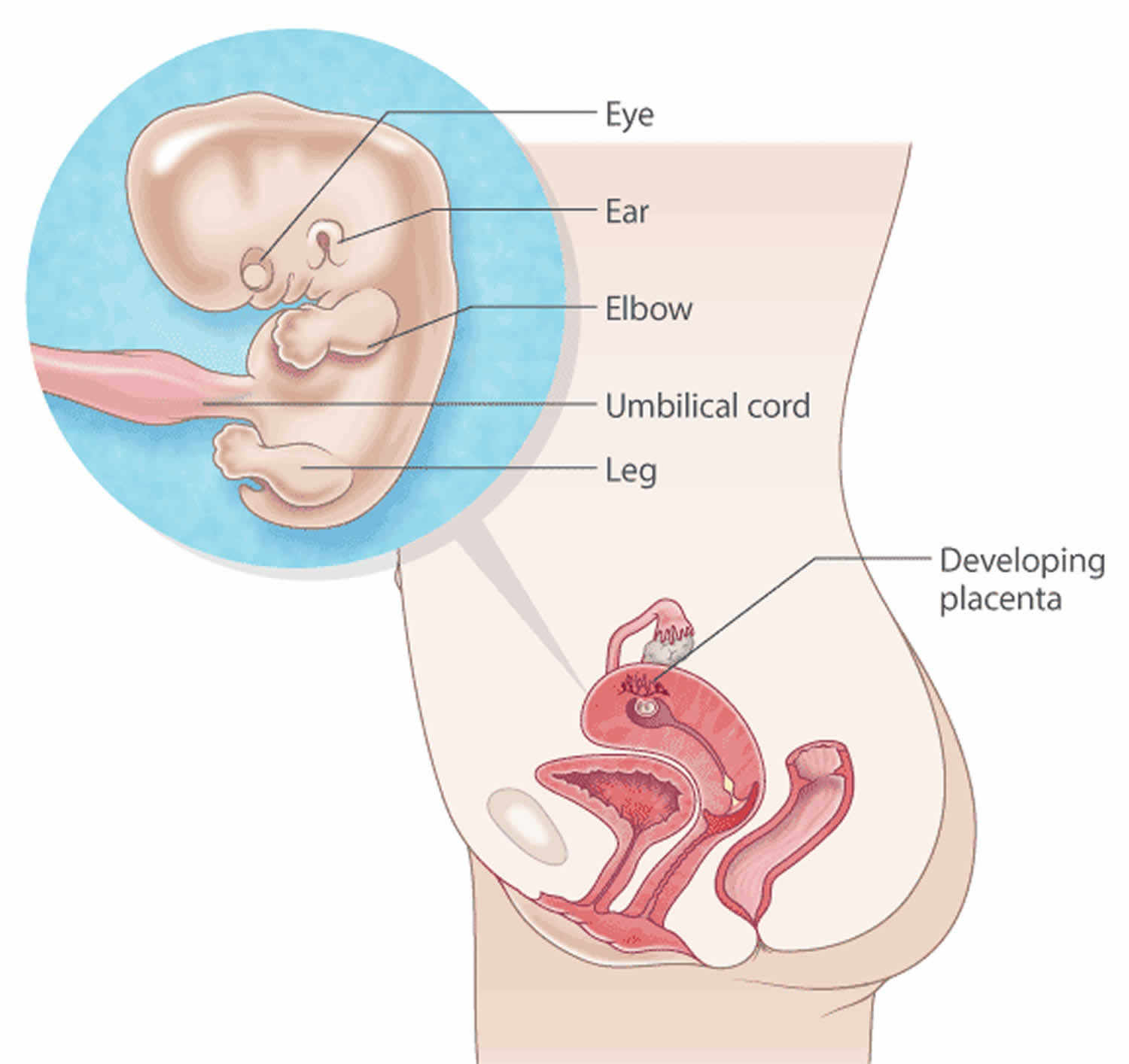
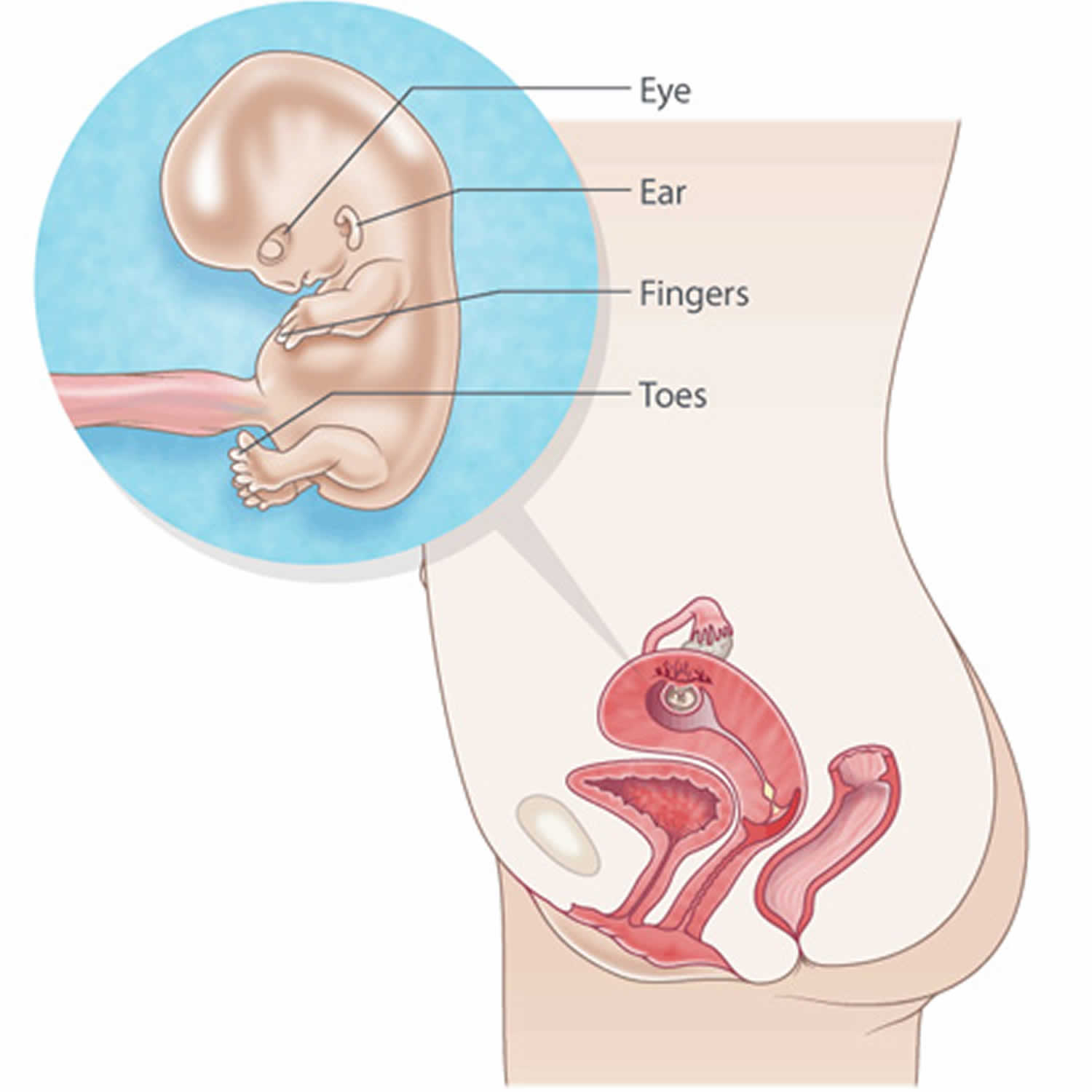
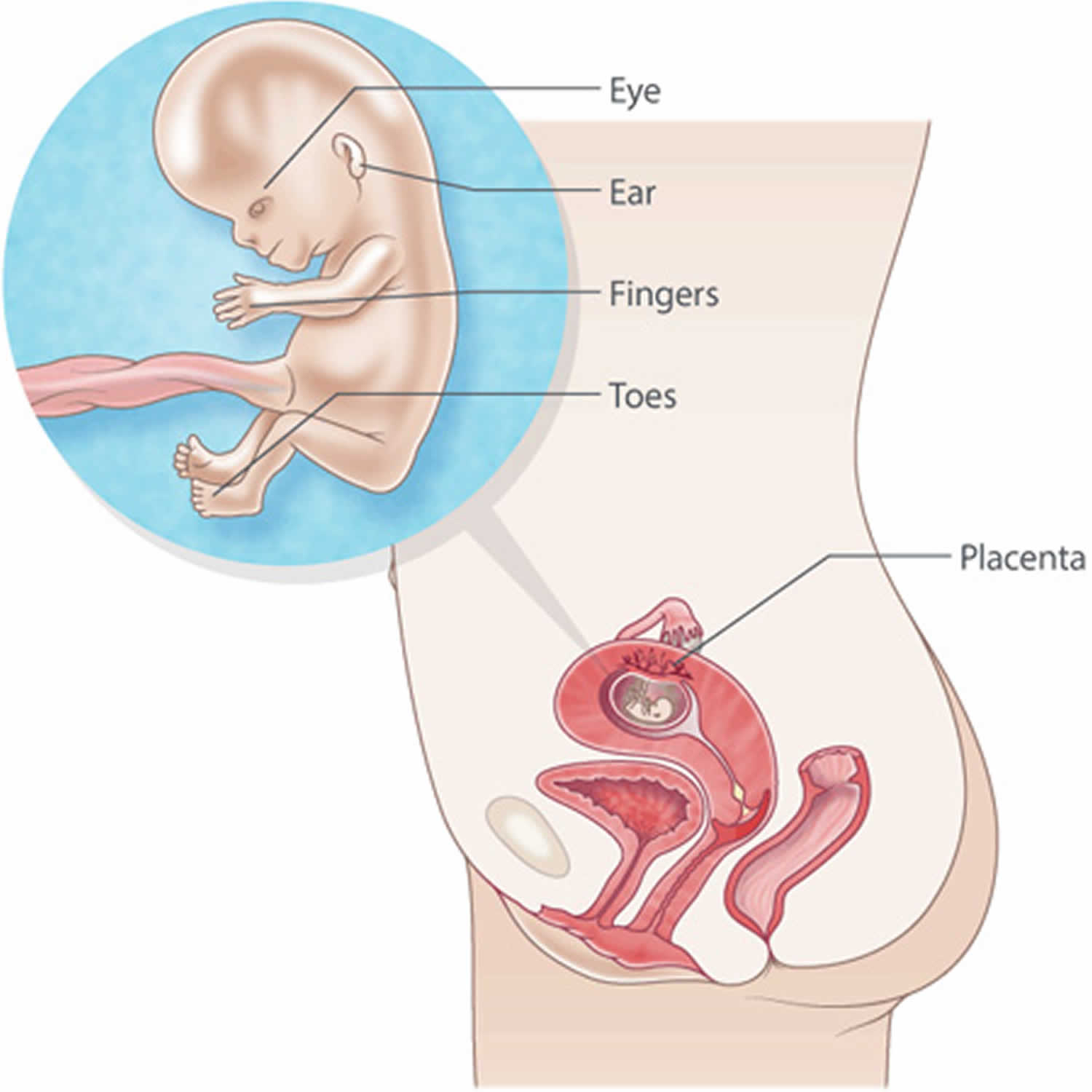
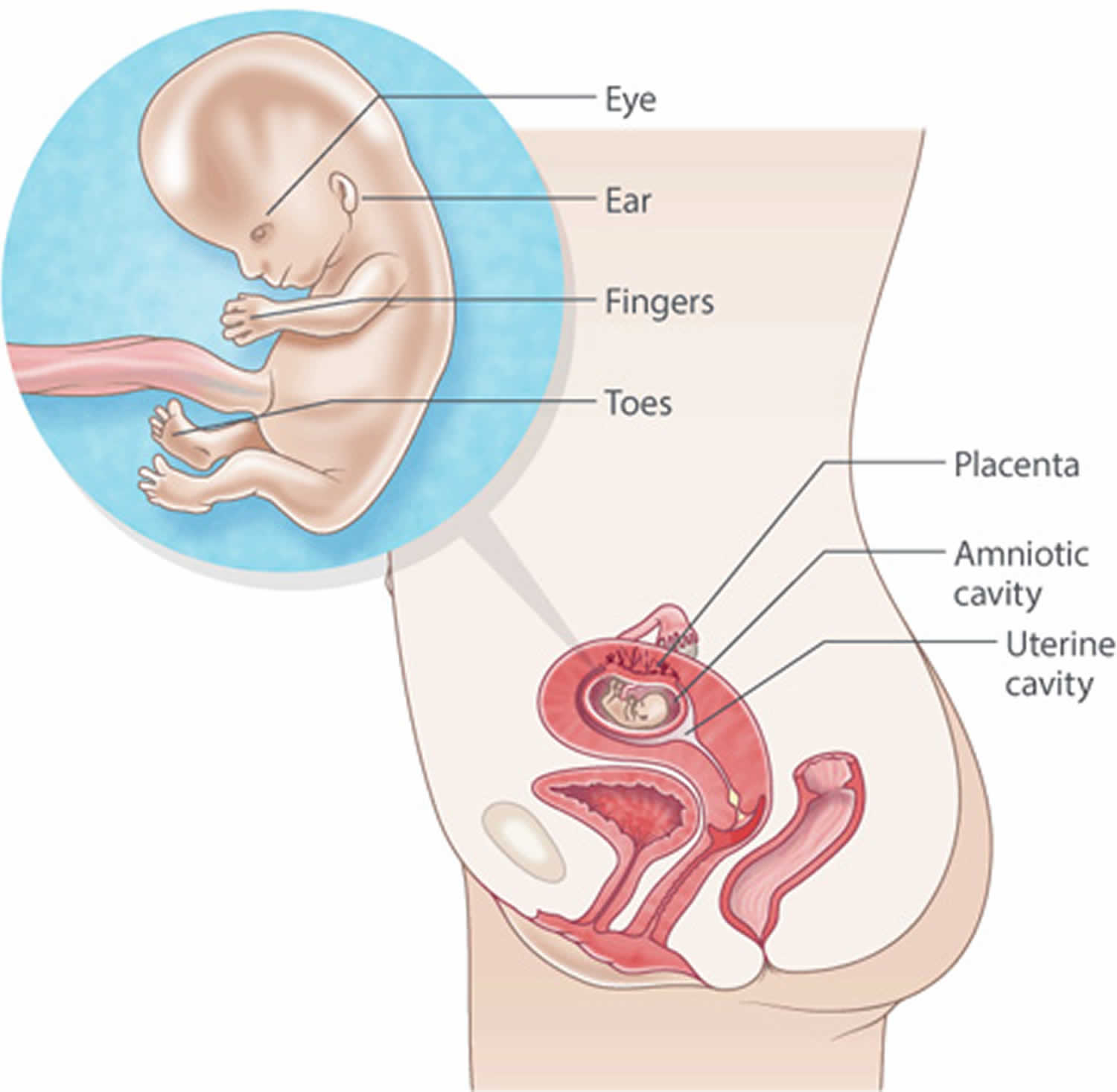
The round ligaments are a pair of cordlike structures in the pelvis that help support the uterus by connecting the front of the uterus to the groin region (Figure 1). During pregnancy, pain in the location of the round ligaments is common. Round ligament pain is most common during the second trimester. Round ligament pain is considered a normal part of pregnancy as your body goes through many different changes. As pregnancy your progresses, the round ligaments become softer and might stretch. It’s believed that pain associated with the round ligaments might be caused by the tightening or spasm of the ligaments or irritation of nearby nerve fibers.
Round ligament pain typically is experienced on the right side of the abdomen or pelvis, but discomfort can also occur on the left or both sides. Round ligament pain often occurs upon waking and rolling over in bed or during rapid movement or vigorous activity.
To relieve round ligament pain, try gentle stretching and changing your position. Avoid rapid or repetitive movement. Flexing your hips before you cough or sneeze might also provide relief. No medication is necessary. Taking acetaminophen (Tylenol, others) might help, however.
Note that pain in your lower abdomen can have other causes, some can be serious. If you have pain accompanied by fever or chills, nausea, vomiting, pain with urination, pain with bleeding, changes in vaginal discharge or moderate or severe pain, see your health care provider.
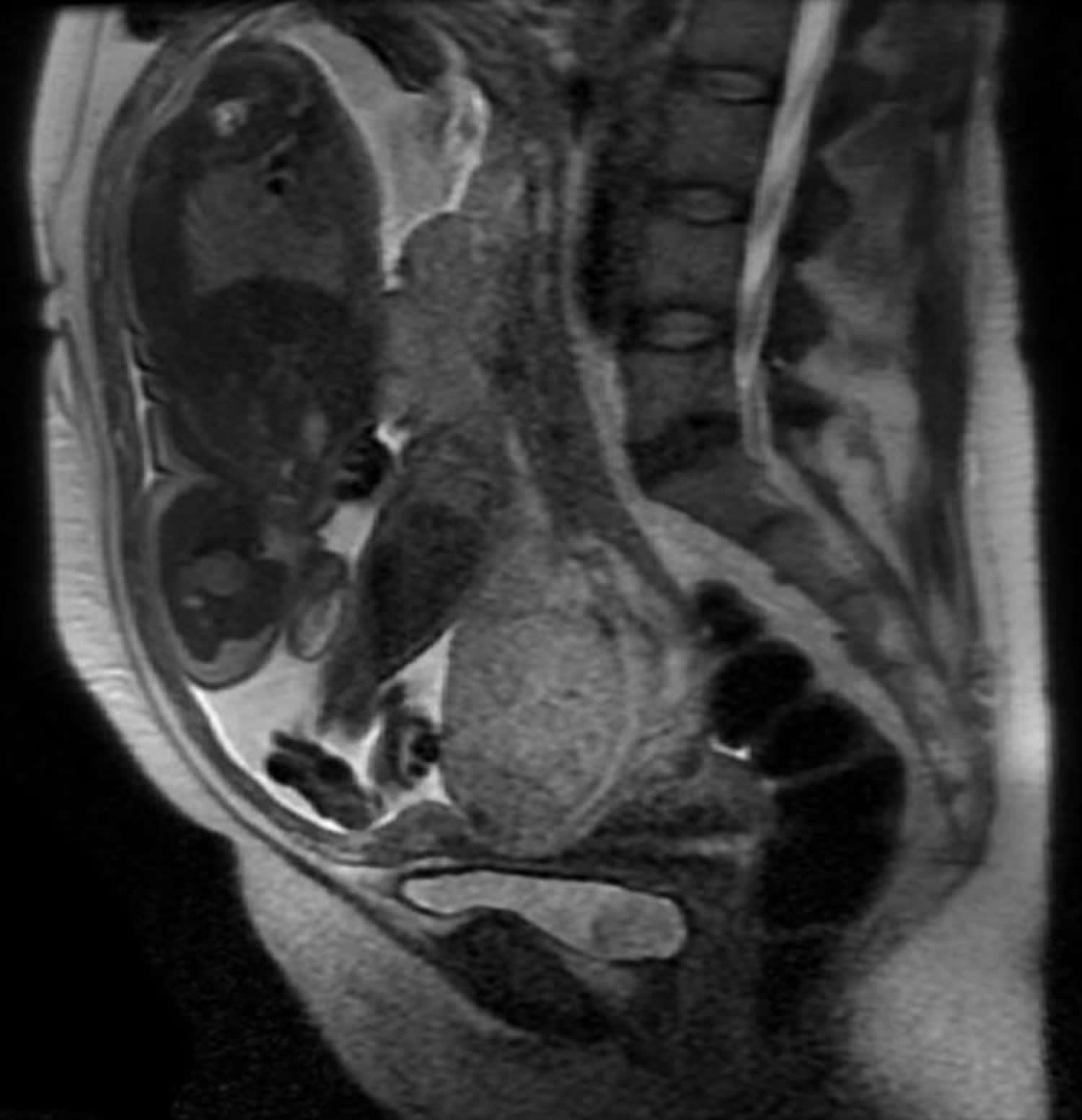
Figure 1. Round ligament anatomy
When you should see your doctor:
- If the pain lasts longer than a few seconds. If the pain lasts for more than a few minutes, you should contact your healthcare provider immediately.
- If your pain persists after resting or it is accompanied by severe pain, you would want to notify your healthcare provider.
- Severe pain or cramping, or more than four contractions in an hour (even if they don’t hurt)
- Low back pain, especially if you didn’t previously have back pain, or an increase in pressure in the pelvic area (a feeling that your baby is pushing down)
- Bleeding, spotting, or a change in the type or amount of vaginal discharge
- Fever, chills, faintness, or nausea and vomiting
- Pain or burning when you urinate
Round ligament pain causes
The round ligament supports the uterus and stretches during pregnancy. It connects the front portion of the uterus to the groin. These ligaments contract and relax muscles, but much more slowly.
Any movement (including going from a sitting to standing position quickly, laughing, or coughing) that stretches these ligaments by making them contract quickly, can cause a woman to experience pain. Round ligament pain should only last for a few seconds.
Round ligament pain symptoms
Round ligament pain is a brief, sharp, stabbing pain or a longer-lasting dull ache that pregnant women commonly feel in the lower abdomen or groin, starting in the second trimester. Women with round ligament pain may have a sharp pain in their abdomen or hip area that is either on one side or both. Some women even report pain that extends into the groin area.
You may feel round ligament pain as a short jabbing sensation if you suddenly change position, such as when you’re getting out of bed or out of a chair or when you cough, roll over in bed, or get out of the bathtub. You may feel it as a dull ache after a particularly active day – when you’ve been walking a lot or doing some other physical activity.
The round ligaments surround your uterus in your pelvis. As your uterus grows during pregnancy, the ligaments stretch and thicken to accommodate and support it. These changes can occasionally cause pain on one or both sides of your abdomen.
You may feel the pain starting from deep inside your groin, moving upward and downward on either side to the top of your hips. The pain is internal, but if you were to trace it on your skin, it would follow the bikini line in a very high-cut bathing suit.
Round ligament pain treatment
Resting comfortably is one of the best ways to help with round ligament pain. Changing positions slowly allows the round ligaments to stretch more gradually and can help alleviate any pain. You can also try flexing your knees towards your abdomen or lying on your side with a pillow under your belly for support and another between your legs. A warm bath and OTC acetaminophen may help, too.
If you know that you are going to sneeze, cough, or laugh you can bend and flex your hips, which can reduce the pull on the ligaments.
If you are having consistent round ligament pain, your health care provider may recommend daily stretching exercises. The most common exercise is done by placing your hands and knees on the floor, lowering your head to the floor, and keeping your bottom in the air.
If you find that you’re more prone to round ligament pain when you’re particularly active, cut back to see if that helps. Then, if you feel fine, you can gradually increase your activity until you find the level of exertion that’s comfortable for you.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}