






Toilet training
The best time to begin toilet training or potty training is when your child is ready to learn. All children learn to use the potty or toilet at a different stage in their life. Using a potty is a new skill for your child to learn. Most children start to show an interest in moving on to a potty or toilet at about two years old. Trying to toilet train too early or getting impatient with the process, can cause your child to become stressed, and may lead to them avoiding going to the toilet. The key is to stay positive and calm, and wait for signs that your child is ready. It’s best to take it slowly and go at your child’s pace. Being patient with them will help them get it right, even if you sometimes feel frustrated.
Children are able to control their bladder and bowels when they’re physically ready and when they want to be dry and clean. Every child is different, so it’s best not to compare your child with others.
Most children are ready to start toilet training from around 2 or 3 years of age, although night time training often takes much longer. By that time, most children are feeling confident and comfortable enough for successful toilet training – but not all are.
Children need to go at their own pace, not that set by parents or day care centers. Your child’s behavior is often a better guide than their age.
Instead of using age, look for signs that your child may be ready to start heading for the potty. You can try to work out when your child is ready. There are a number of signs that your child is starting to develop bladder control:
- they follow simple instructions
- they know when they’ve got a wet or dirty nappy
- they get to know when they’re peeing and may tell you they’re doing it
- they keep a diaper dry for 2 hours or more
- the gap between wetting is at least an hour (if it’s less, potty training may fail, and at the very least will be extremely hard work for you)
- they show they need to pee by fidgeting or going somewhere quiet or hidden
- they know when they need to urinate and may say so in advance
- they understand and use words about using the potty
- they make the connection between the urge to pee or poop and using the potty
- they get to the potty, sit on it for enough time, and then get off the potty
- they pull down diapers, disposable training pants, or underpants
- they show an interest in using the potty or wearing underpants
Most children begin to show these signs when they’re between 18 and 24 months old, though some may not be ready until later than that. And boys often start later and take longer to learn to use the potty than girls.
Toilet training requires patience. Girls are usually trained faster than boys, but not always.
Bear in mind that most children can control their bowels before their bladder.
- by age 1, most babies have stopped doing poop at night
- by age 2, some children will be dry during the day, but this is still quite early
- by age 3, 9 out of 10 children are dry most days – even then, all children have the odd accident, especially when they’re excited, upset or absorbed in something else
- by age 4, most children are reliably dry during the day
It usually takes a little longer for children to learn to stay dry throughout the night. Although most learn this between the ages of 3 and 5, up to 1 in 5 children aged 5 sometimes wet the bed.
Even when trained, many children still don’t have full night time bladder control until about 5 years of age, or in some cases, several years later.
Often, children are 3-4 years old before they’re dry at night. One in 5 five-year-olds and 1 in 10 six-year-olds still uses nappies overnight. And bedwetting is very common in school-age children. If your child wets the bed, there are things you can do about it when you and your child are ready.
During the day, children often get caught up in what they are doing and forget to take potty breaks. Expect accidents, and don’t punish or shame your child for them. Toilet training works best when there is no pressure.
It’s worth keeping an eye out for possible health problems connected with toilet training. Signs to look for include:
- a big increase or decrease in the number of poops or urine
- poops that are very hard to pass
- unformed or very watery poops
- blood in the poop or urine (sometimes appears as cloudy urine)
- pain when your child goes to the toilet.
If you feel there might be a problem or you’re worried about how your child is adapting to toilet training, check with your doctor.
What is toilet training?
Toilet training helps children:
- recognize the need to go to the toilet
- control the need to go to the toilet
- communicate the need to go to the toilet
- complete the toilet sequence as far as they are able.
The goal of toilet training is for a child who is able to:
- pull their underwear down
- get onto the toilet
- sit on the toilet
- have a pee/poop
- wipe themselves
- get off the toilet
- pull their underwear up
- flush toilet
- wash and dry hands.
How long does toilet training take?
Teaching a toddler to use the potty isn’t an overnight task. It often takes between 3 and 6 months, but can take more or less time for some children. If you start too soon, the process tends to take longer. And it can take months to even years to master staying dry at night.
Why is my child taking a long time to learn to use the toilet?
If your child takes a long time to learn to use the toilet:
- Try to get clothes that are easy to wear, change, and wash.
- Items such as large size nappies, waterproof mattress covers, and covers for duvets and pillows may be available from the continence service, when your child is three or four– ask your health care provider. If not, you can get them from larger chemists.
- If your child is older, it is often you as their parents who understand their needs, and you may be able to devise your own strategies.
- Do not despair. Try to speak with other parents for support, advice and tips.
Common toilet training problems
Many kids who’ve been using the potty have some trouble during times of stress. For example, a 2- or 3-year-old dealing with a new sibling may start having accidents.
But if your child was potty-trained and is regularly having problems, talk with your doctor.
Talk to your doctor if you have any questions about toilet training or your child is 4 years or older and is not yet potty trained.
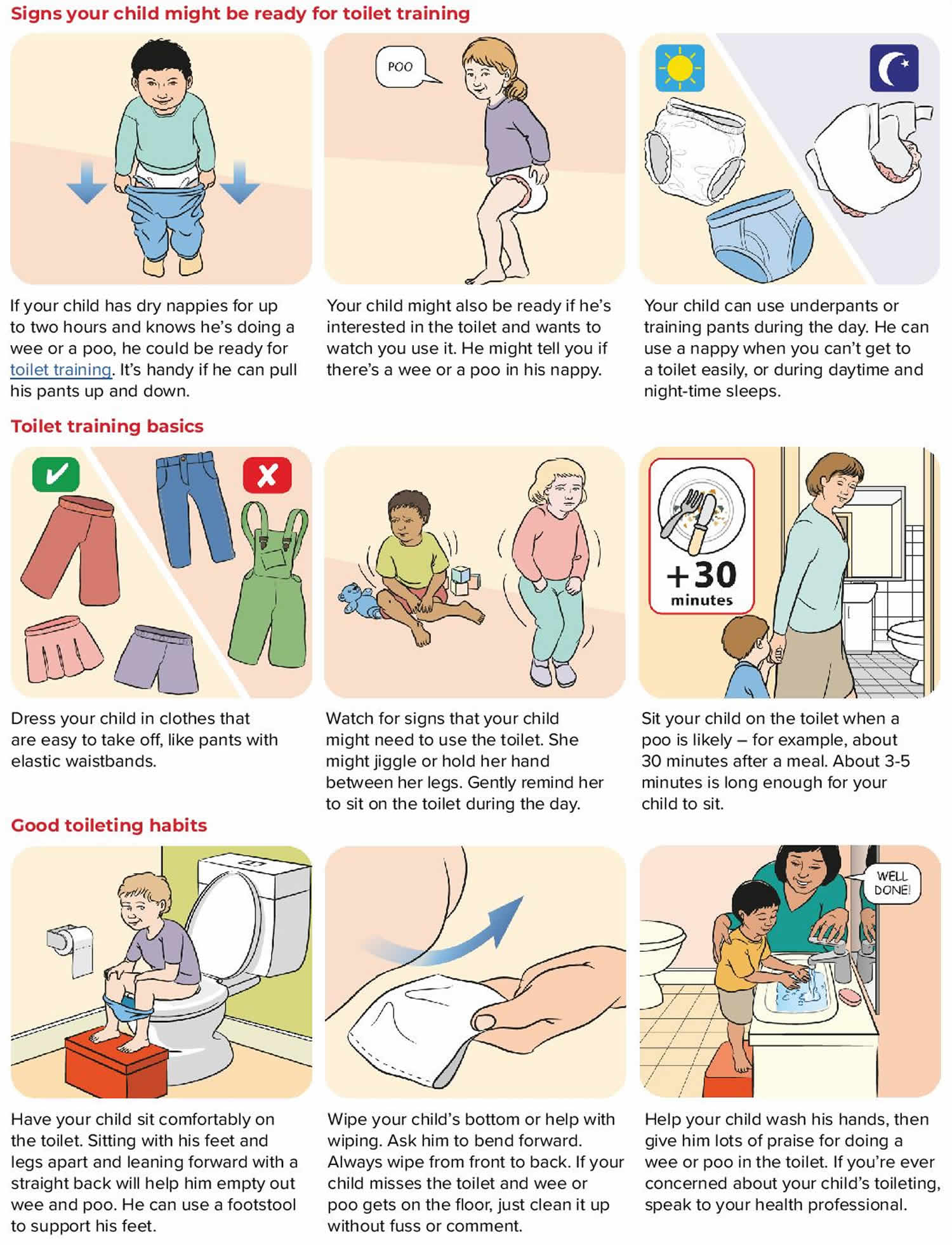
Signs that your child is ready for potty training
You might see signs that your child is ready for toilet training from about two years on. Some children show signs of being ready as early as 18 months, and some might be older than two years.
Your child is showing signs of being ready for potty training if they:
- are walking and can sit for short periods of time
- are becoming generally more independent when it comes to completing tasks, including saying ‘no’ more often
- are becoming interested in watching others go to the toilet – this can make you uncomfortable, but it’s a good way to introduce things
- have dry nappies for up to two hours at a time – this shows they can store urine in their bladder (which automatically empties in younger babies or newborns)
- tell you with words or gestures when they have done a poop or urinate in their nappy – if they can tell you (either with words or facial expressions) before it happens, they’re ready for toilet training
- begin to dislike wearing a nappy, perhaps trying to pull it off when it’s wet or soiled
- want their nappy changed when it is wet or dirty
- have regular, soft, well-formed bowel movements
- can pull their pants up and down
- can get to the potty on their own
- can follow simple instructions like ‘Give the ball to daddy’
- show understanding about things having their place around the home.
Not all these signs need to be present when your child is ready. A general trend will let you know it’s time to start.
What if my child does not show these signs?
If your child’s condition means that s/he is not showing any of these signs you should discuss it with one of the professionals involved with your child’s care. This could be your family doctor, community nurse, occupational therapist or pediatrician. You will need support from the professionals who deal with your child on a day to day basis and it is important to work together on ways of addressing the issue.
When to start potty training
Look for signs that your child is ready to use the potty or toilet (see above the signs that your child is ready for potty training). Remember, you cannot force your child to use a potty. If they’re not ready, you will not be able to make them use it. In time, they will want to use one – most children will not want to go to school in nappies any more than you would want them to. In the meantime, the best thing you can do is to encourage the behavior you want.
Most parents start thinking about potty training when their child is between 2 and 2 and a half, but there’s no perfect time. Some people find it easier to start in the summer, when there are fewer clothes to take off and washed clothes dry more quickly.
Try potty training when there are no great disruptions or changes to your child’s or your family’s routine. It’s important to stay consistent, so you do not confuse your child.
If you go out, take the potty with you, so your child understands that you’d like them to urinate or poop in the potty every time they need to go. Check that any other people who look after your child can help with potty training in the same way as you.
Potty training is usually fastest if your child is at the last stage before you start the training. If you start earlier, be prepared for a lot of accidents as your child learns.
They also need to be able to sit on the potty and get up from it when they’re done, and follow your instructions.
Getting ready for potty training
If you think your child is showing signs of being ready for toilet training, the first step is to decide whether you want to train using a potty or the toilet.
- There are some advantages to using a potty – it’s mobile and it’s familiar, and some children find it less scary than a toilet. Try to find out your child’s preference and go with that. Some parents encourage their child to use both the toilet and potty.
- Second, make sure you have all the right equipment. For example, if your child is using the toilet you’ll need a step for your child to stand on. You’ll also need a smaller seat that fits securely inside the existing toilet seat, because some children get uneasy about falling in.
- Third, it’s best to plan toilet training for a time when you don’t have any big changes coming up in your family life. Changes might include going on holiday, starting day care, having a new baby or moving house. It can be a good idea to plan toilet training for well before or after these changes.
Also, toilet training might go better if you and your child have a regular daily routine. This way, the new activity of using the toilet or potty can be slotted into your normal routine.
Here are some tips for getting ready:
- Teach your child some words for going to the toilet – for example, ‘pee’, ‘poop’ and ‘I need to go’.
- When you change your child’s nappy, put wet and dirty nappies in the potty – this can help your child understand what the potty is for.
- Let your child try sitting on the potty or the small toilet seat to get familiar with the new equipment.
- Let your child watch you or other trusted family members using the toilet, and talk about what you’re doing.
- Once or twice a day you might want to start putting trainer pants on your child. This helps your child understand the feeling of wetness.
- Make sure your child is eating plenty of fiber and drinking lots of water so your child doesn’t get constipated. Constipation can make toilet training harder.
Using a potty will be new to your child, so get them used to the idea gradually. Talk about your child’s nappy changes as you do them, so they understand urine and poop and what a wet nappy means. If you always change their nappy in the bathroom when you’re at home, they will learn that’s the place where people go to the toilet. Helping you flush the toilet and wash their hands is also a good idea.
Leave a potty where your child can see it and explain what it’s for. Children learn by watching and copying. If you’ve got an older child, your younger child may see them using it, which will be a great help. It helps to let your child see you using the toilet and explain what you’re doing. Using your child’s toys to show what the potty is for can also help.
You could see if your child is happy to sit on the potty for a moment, just to get used to it, when you’re changing their nappy, especially when you’re getting them dressed for the day or ready for bed at night.
Once you start, toilet training might take days, weeks or months. The key is to not push your child, and let your child learn at their own pace. Your child will get the hang of it in time. And if your child doesn’t cooperate or seem interested in toilet training right now, just wait until they want to try again.
Potty types
The two basic potty options are:
- a standalone, toddler-size potty chair with a bowl that can be emptied into the toilet
- a toddler-size seat that can be placed on top of a toilet seat that will let your child feel more secure and not fear falling in. If you choose this, get a stepping stool so your child can reach the seat comfortably and feel supported while having a bowel movement.
It’s usually best for boys to first learn to use the toilet sitting down before learning to pee standing up. For boys who feel awkward — or scared — about standing on a stool to pee in the toilet, a potty chair may be a better option.
You may want to get a training potty or seat for every bathroom in your house. You may even want to keep a potty in the trunk of your car for emergencies. When traveling long distances, be sure to take a potty seat with you and stop every 1 to 2 hours. Otherwise, it can take too long to find a restroom.
Training pants
Disposable training pants are a helpful step between diapers and underwear. Because kids’ nighttime bladder and bowel control often lags behind their daytime control, some parents like using training pants at night. Others prefer that their child use training pants when they’re out and about. Once the training pants remain dry for a few days, kids can make the switch to wearing underwear.
But some people think that disposable training pants might make kids think it’s OK to use them like diapers, thus slowing the toilet-teaching process.
Ask your doctor if your child would benefit from using disposable training pants as a transitional step.
Before starting
Choose a time when you can spend a lot of time with your child, when your child seems happy and there are no major distractions or stressful events like starting nursery, moving house, moving from a cot to a bed. Make sure the time you choose fits in with you as well – perhaps at a time when there is someone else to help you if this is possible.
It may take some time for your child to learn, so make sure that toilet training can be carried out in the other places your child visits such as the playgroup, nursery, or school.
Tips before starting:
- Look at the times your child is most likely to use the toilet, for example after meals, when she/he wakes up from a sleep. It is worth making a chart for a few weeks to establish any patterns. The chart can be very simple where you note the times when the child urinate or poops
- Plan a routine you can stick to, until it becomes established
- Make sure the potty or toilet is comfortable for your child and your child can sit on it without any fear of falling off. Your child should be able to place his/her feet flat on the floor or foot step
- There are various toilet seats and steps available from retail outlets. It is worth looking at the range and deciding what would be good for your child
- If your child has difficulty in sitting, an occupational therapist should be able to help with equipment and check whether the toilet needs to be adapted so it is more comfortable for your child
- Make sure you change your child in the toilet so that they get used to the toilet as a place where urination and poop happens
- Try and make the bathroom as welcoming as possible. You could put stickers on the walls to make it an exciting place to be.
How to start potty training
It’s a good idea to start toilet training on a day when you have no plans to leave the house. Keep the potty in the bathroom. If that’s upstairs, keep another potty downstairs so your child can reach the potty easily wherever they are. The idea is to make sitting on the potty part of everyday life for your child.
Encourage your child to sit on the potty after meals, because digesting food often leads to an urge to do a poop. Having a book to look at or toys to play with can help your child sit still on the potty.
If your child regularly does a poop at the same time each day, leave their nappy off and suggest that they go in the potty. If your child is even the slightest bit upset by the idea, just put the nappy back on and leave it a few more weeks before trying again.
Encouraging them to use the potty to pee will help build their confidence for when they are ready to use it to poop.
As soon as you see that your child knows when they’re going to pee, encourage them to use their potty. If your child slips up, just mop it up and wait for next time. It takes a while for them to get the hang of it.
If you do not make a fuss when they have an accident, they will not feel anxious and worried, and are more likely to be successful the next time. Put them in clothes that are easy to change and avoid tights and clothes with zips or lots of buttons.
Your child will be delighted when they succeed. A little praise from you will help a lot. It can be quite tricky to get the balance right between giving praise and making a big deal out of it. Do not give sweets as a reward, but you could try using a sticker chart.
TIPS: Try to stay calm if toilet training seems to take longer than you expect. Stay positive about your child’s achievements, because your child will get there eventually. Too much tension or stress can lead to negative feelings and might result in your child avoiding going to the toilet.
Timing
- Sit your child on the potty at times when pooping often happen, like 30 minutes after eating or after having a bath. This doesn’t work for all children – true toilet training begins when your child is aware of doing a pee or poop and is interested in learning the process.
- Look out for signs that your child needs to go to the toilet. Cues include changes in posture, passing wind, going quiet or moving to a different room by themselves.
- If your child doesn’t do a pee or poop after 3-5 minutes of sitting on the potty or toilet, take your child off. It’s best not to make your child sit on the toilet for long periods of time, because this will feel like punishment.
There are some times when you may want to put off starting toilet training, such as:
- when traveling
- around the birth of a sibling
- changing from the crib to the bed
- moving to a new house
- when your child is sick (especially if diarrhea is a factor)
Encouraging and reminding your child
- Praise your child for trying (even if progress is slow), especially when they’re successful. You could say, ‘Well done for sitting on the potty’. This lets your child know they’re doing a good job. Gradually reduce the amount of praise as your child masters each part of the process.
- At different stages throughout the day (but not too often), ask your child if they need to go to the toilet. Gentle reminders are enough – it’s best if your child doesn’t feel pressured.
- If your child misses the toilet, try not to get frustrated. Children don’t usually have accidents on purpose, so just clean up without any comments or fuss.
Pants and clothing
- Stop using nappies (except at night and during daytime sleeps). Start using underpants or training pants all the time. You can even let your child choose some underpants, which can be an exciting step.
- Dress your child in clothes that are easy to take off – for example, trousers with elastic waistbands, rather than full body suits. In warmer weather, you might like to leave your child in underpants when you’re at home.
Hygiene
- Wipe your child’s bottom until your child learns how. Remember to wipe from the front to the back, particularly with girls.
- Teach your son to shake his penis after a pee to get rid of any drops. Early in toilet training it sometimes helps to float a ping pong ball in the toilet for your son to aim at. Or he might prefer to sit to do a pee, which can be less messy.
- Teach your child how to wash hands after using the toilet. This can be a fun activity that your child enjoys as part of the routine.
Potty training pants and pull-ups
Your child is more likely to understand toilet use if they’re no longer wearing a nappy. Disposable or washable potty training pants also called pull-ups can be handy when you start potty training and can give children confidence when it’s time to swap nappies for “grown-up” pants. They do not soak up urine as well as disposable nappies, so your child will find it easier to tell when they are wet.
Pull-ups are very popular and are marketed as helpful for toilet training. It isn’t clear that they actually help. But you can try them to help your child get used to wearing underwear.
Training pants are absorbent underwear worn during toilet training. They’re less absorbent than nappies but are useful for holding in bigger messes like accidental poop. Training pants should be a step towards normal pants, rather than a replacement for nappies. Encourage your child to keep their training pants dry by using the potty. Once your child is wearing training pants, dress your child in clothes that are easy to take off quickly.
Generally, cloth training pants are less absorbent than pull-ups and can feel a little less like a nappy. Pull-ups might be handier when you’re going out.
Wearing training pants is a big move for your child. If you celebrate it, the transition will be easier. Talk about how grown-up your child is and how proud you are.
If your child is not ready to stop wearing nappies and it’s hard for them to know when they’ve done a pee, you can put a piece of folded kitchen paper inside their nappy. It will stay wet and should help your child learn that urinating makes you feel wet.
Out and about while toilet training
It’s easier to stay home for a few days when you start toilet training, but you’ll probably have to go out at some stage.
Wherever you’re going, it’s a good idea to check where the nearest toilet is. If you’re going to a local shopping center, ask your child if they need to go when you get there. This can help get your child familiar with the new area.
It’s best to take a spare change of underpants and clothes for your child when you’re out, until your child is very confident about using the toilet. It’s also a good idea to carry plastic bags for wet or soiled clothes.
If your child goes to a child care service or to friends’ or relatives’ houses without you, let people know that your child is toilet training. This way they can help your child use the toilet or potty in the way that you do at home.
Night-time potty training
Focus on getting your child potty trained during the day before you start leaving their nappy off at night. If your child’s nappy is dry or only slightly damp when your child wakes for a few mornings in a row, they may be ready for night-time potty training.
Ask your child to use the potty last thing before they go to bed and make sure it’s close by, so they can use it if they need to pee in the night. There are bound to be a few accidents, so a waterproof sheet to protect your child’s mattress is a good idea.
Just like daytime potty training, it’s important to praise your child for success. If things are not going well, stick with nappies at night for a while longer and try again in a few weeks’ time.
Using the toilet instead of the potty
Some children start using the toilet instead of the potty earlier than others. A child’s trainer seat that clips onto the toilet can help make your child feel safer and more confident on the toilet. A step for your child to rest their feet on gets your child in a good position for doing a poop.
If you have a boy, encourage them to sit down to urinate. If they also need a poop, sitting down will encourage them to go.
Once you start toilet training
Be patient don’t expect instant results.
- Do not restrict fluid intake – plenty of drinks should be given so that the need to go to the toilet becomes familiar.
- Ensure your child has a healthy diet with plenty of fiber for example brown bread, fruit, wholegrain – to help their bowel movements to be soft and easy to pass.
- Take your child to the toilet at the times you expect they may need to go – refer to the chart you have made.
- Avoid taking your child toilet frequently. If they have just used the toilet, they will not need to visit for at least one hour.
- Keep to the planned routine as much as you can.
- Do not show any signs of concern – it will make your child feel anxious.
Remember there are several steps in the whole process and each one needs to be reached – they may not all happen at once.
- If your child is reluctant to sit still, you could sing some songs or read a book with them just for a few minutes to get your child used to sitting on the potty or toilet. Never keep your child on the potty or toilet for more than five minutes.
- If your child is older and too big for a potty and still not showing interest in using the toilet then make sure they visit the toilet area regularly. You may need to put a favorite book, picture or toy next to the toilet or play a favorite piece of music to encourage them to come into the room.
- Make sure all toileting needs occur in the toilet or bathroom so that your child associates the changing of nappies/pants with the toilet area.
- Praise your child first for showing an interest in the potty or toilet, then for using the potty – every small step should be rewarded with praise or stickers.
- Make sure your child sees you washing your hands after wiping them so it becomes part of the process of using the toilet.
- Let your child get used to the routine of washing his/her hands after being on the potty or toilet.
Setbacks and accidents while toilet training
Learning to do pees and poops in the toilet takes time. You can expect accidents and setbacks – these are all just part of the process.
If your child gets upset because of an accident, reassure your child that it doesn’t matter and there’s no need to worry.
Here are ideas to help avoid accidents:
- Pay attention if your child says they need the toilet straight away. They might be right!
- If you’re sure your child hasn’t done a poo or pee in a while, remind your child that they might need to go. Your child might be so caught up in what they’re doing that they don’t realise they need to go until it’s too late.
- Check if your child wants to go to the toilet during a long playtime or before an outing. If they don’t want to go, that’s fine.
- Try to make sure the potty or toilet is always easy to get to and use.
- Ask your child to pee just before going to bed.
How to toilet train your child
Dress your child in clothes that are easy to get off and on.
Start by putting a potty chair in your child’s play area. Put your child on the potty seat when they give a signal that they need to go to the toilet. If you are using the toilet, buy a toddler toilet seat with a smaller hole that fits inside the big toilet seat. Put a step there so they can climb up by themselves and rest their feet while they are sitting. Boys can pee standing up or sitting.
Notice when your child is about to urinate or poop. Guide them to the potty or toilet. Stay calm and relaxed. Sit with your child and read to them while they sit on the potty (5 minutes is long enough). Praise and hug your child for sitting quietly and trying to use the potty or toilet, even when they are not successful.
When they have finished, wipe your child’s bottom. Teach girls to wipe from front to back.
When they have used the potty or toilet on their own a few times, you can allow your child to pick out their ‘big boy’ or ‘big girl’ underwear. Make sure you take your child’s potty chair with you when traveling, for consistency.
Potty training with a child with disability
Some children with a long-term illness or disability find it more difficult to learn to use a potty or toilet. This can be challenging for them and for you, but it’s important not to avoid potty training for too long. It is important to speak to a doctor to check for physical problems if your child is having difficulty in learning to use the toilet.
Most children start to show an interest in moving on to a potty or toilet at about two years old. If your child has a physical or learning disability they may not be ready to start until they are older. They may need longer to learn to use the potty or toilet.
Some children, particularly those with profound and multiple difficulties may not be able to use the toilet on their own, but will need to have a toileting program which will ensure their needs are treated with respect. Ask your doctor or community nurse for advice.
All children are different and the way they learn to use the toilet may be linked with the specific condition they have. It is a good idea to get in touch with the relevant support groups to get advice from people who have more experience.
Smearing
Some children with learning disabilities smear their feces after going to the toilet. There can be various reasons for this. It could be a child has simply not understood the process of wiping with toilet paper properly. Others enjoy the feel of the texture of the feces and providing them with an alternative activity such as play dough can resolve the situation. Some will use it as a way of getting attention, or because they have learnt they are rewarded for such behavior by being given a nice warm bath. Children can also behave in this way because they are extremely upset and agitated.
If your child smears:
- try to stay calm
- avoid giving them lots of attention as a result of their behavior
- reinforce good behavior by giving them lots of praise when they carry out other activities well
- try to see if there is a pattern to their behavior, as it might help you understand why they are doing it
- seek advice from a professional such as a nurse, doctor, occupational therapist or psychologist on dealing with it
- set a period of time to try any strategies and if nothing happens, wait for a while before starting again.















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}