





Spontaneous pneumothorax
A spontaneous pneumothorax is the sudden onset of a collapsed lung with the presence of air or gas in the pleural cavity (the space around the lungs) without any apparent cause, such as a traumatic injury to the chest or a known lung disease. This buildup of air puts pressure on the lung, so it cannot expand as much as it normally does when you take a breath. In most cases of spontaneous pneumothorax, a small area in the lung that is filled with air, called a bleb, ruptures, causing the air to leak into the space around the lung.
Spontaneous pneumothorax can be either small or large. A small spontaneous pneumothorax may resolve without treatment, while larger pneumothorax may need surgical intervention. Treatment for a pneumothorax usually involves inserting a flexible tube or needle between the ribs to remove the excess air.
In most cases of spontaneous pneumothorax, the cause is unknown. Tall and thin adolescent males are typically at greatest risk, but females can also have this condition. Other risk factors include connective tissue disorders, smoking, and activities such as scuba diving, high altitudes and flying.
Figure 1. Lungs pleural cavity
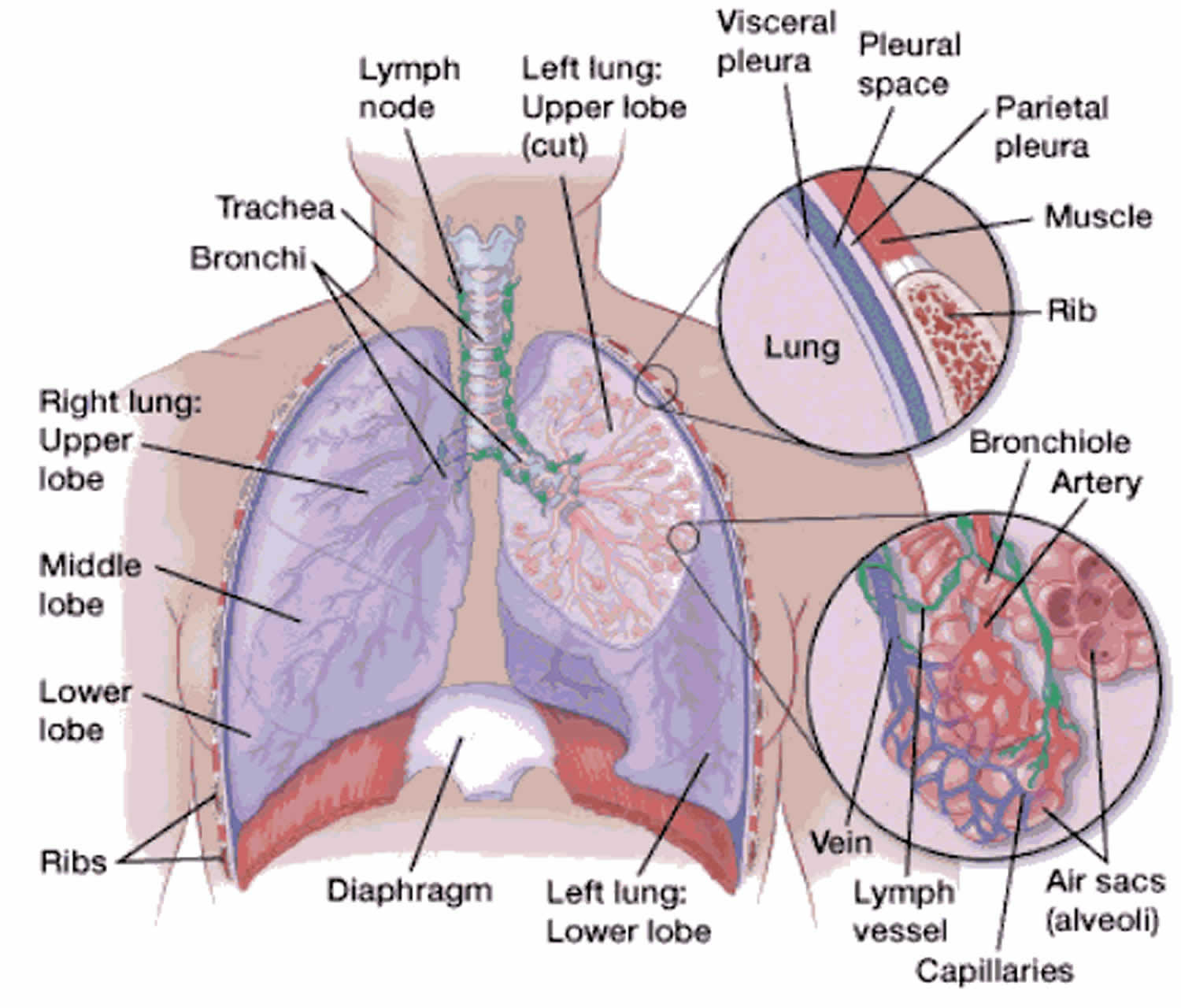
Figure 2. Collapsed and normal lung
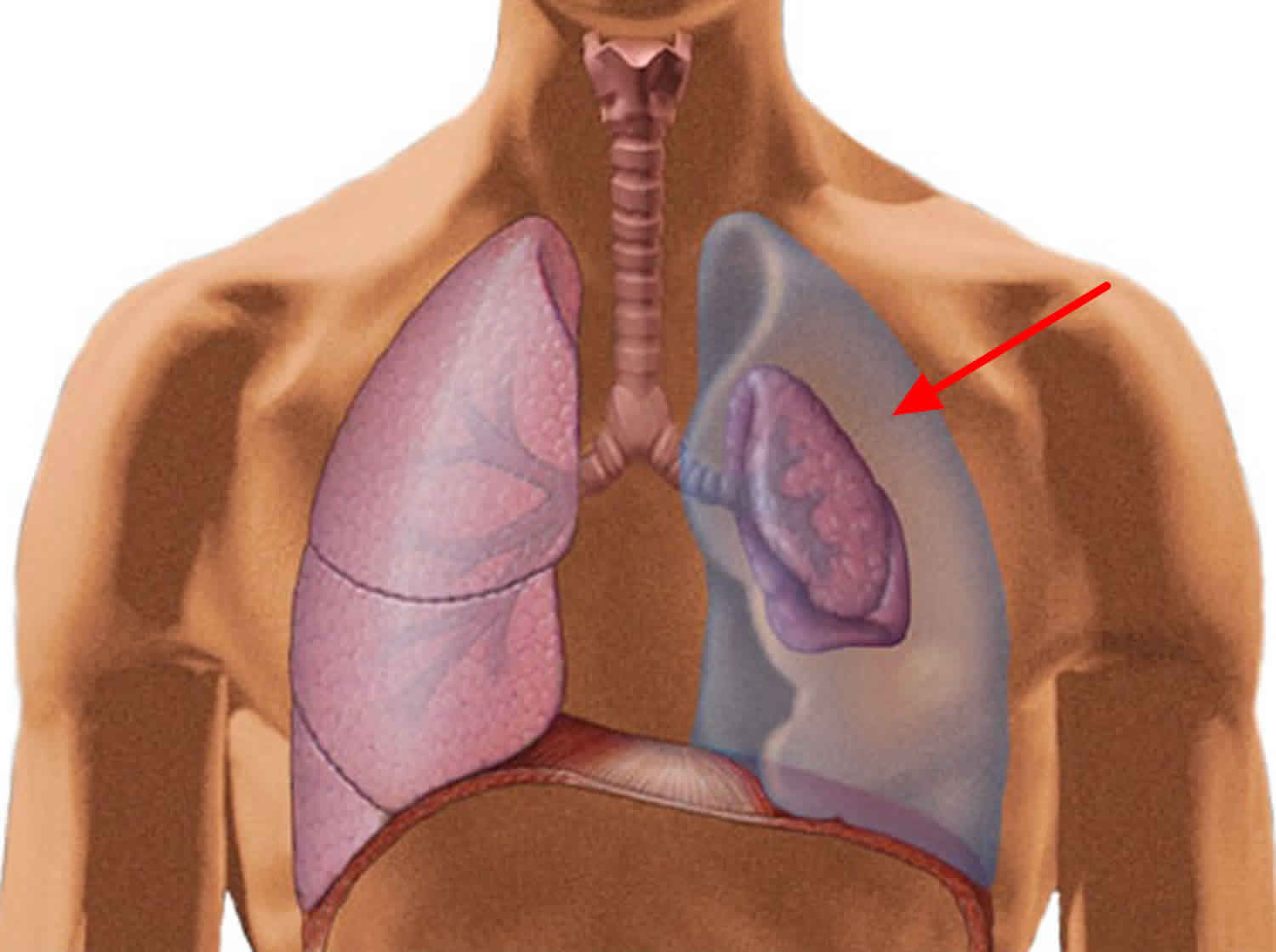
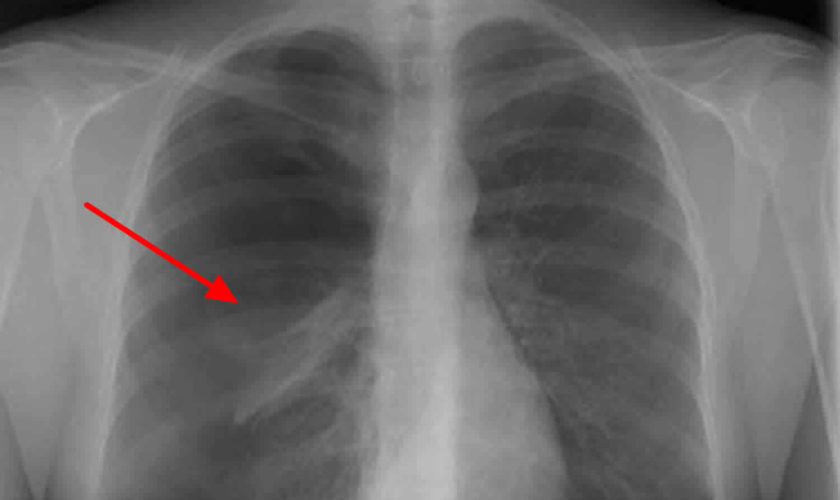
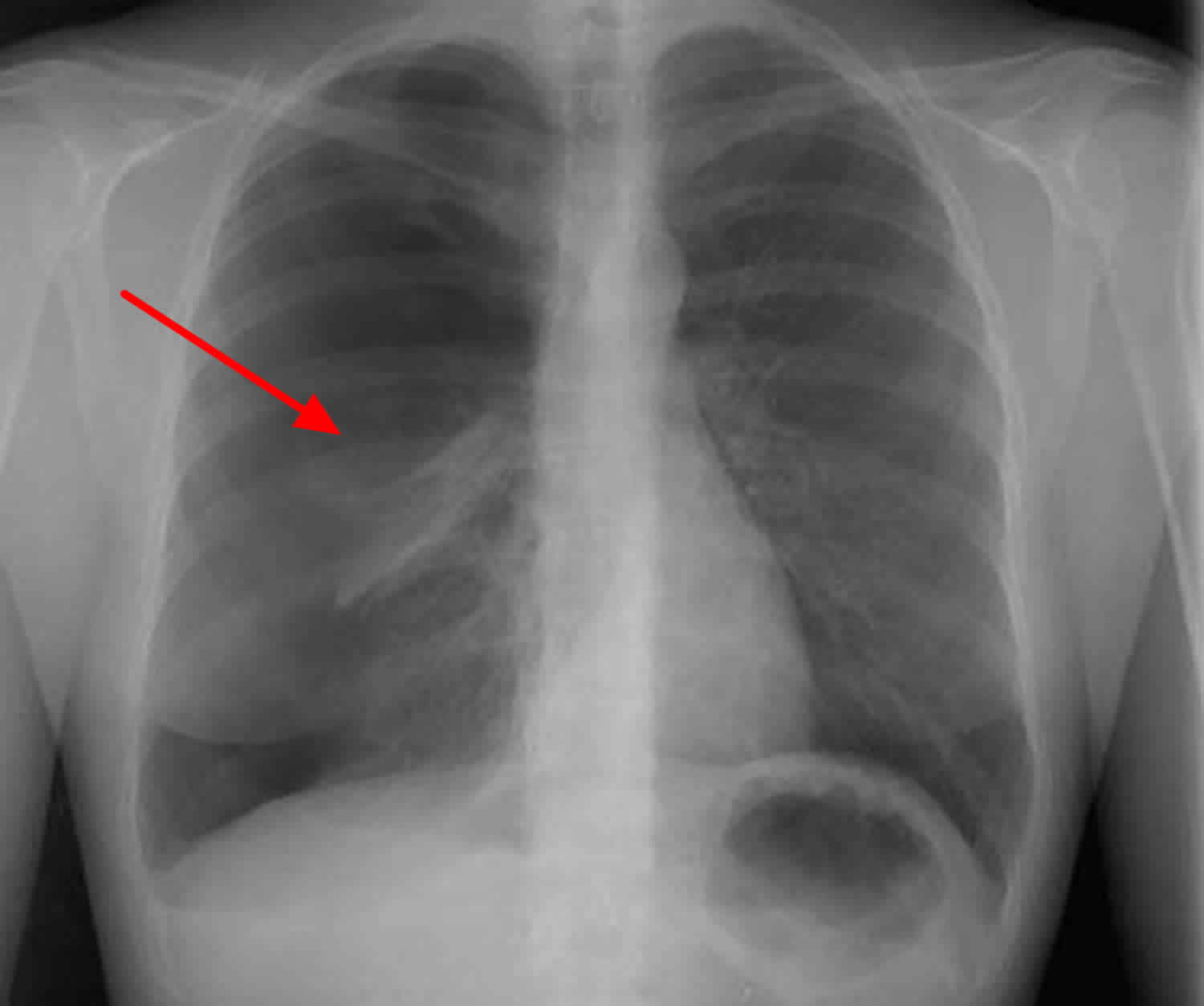
Figure 3. A large, right-sided pneumothorax has occurred from a rupture of a subpleural bleb (chest X-ray).
Types of pneumothorax
There are different types of pneumothorax:
Primary spontaneous pneumothorax
Primary spontaneous pneumothorax is the most common type of pneumothorax, is described as primary because it has no known cause and develops in otherwise healthy people. Primary spontaneous pneumothorax is thought to be caused by a tiny tear of an outer part of the lung. Primary spontaneous pneumothorax is more common in tall people and mainly affects healthy young adults without lung disease.
Secondary spontaneous pneumothorax
Secondary spontaneous pneumothorax develops as a complication of existing lung disease, such as chronic obstructive pulmonary disease (COPD), pneumonia, tuberculosis, sarcoidosis or cystic fibrosis. The lung disease weakens the edge of the lung in some way, making the lung more likely to tear and cause air to escape.
Traumatic pneumothorax
Traumatic pneumothorax is a type of pneumothorax is caused by an incident such as a car accident, broken ribs or a stab wound.
Iatrogenic pneumothorax
Iatrogenic pneumothorax is a pneumothorax that occurs as a result of mechanical ventilation, which causes an imbalance in the air pressure around the lungs.
Tension pneumothorax
Tension pneumothorax is a pneumothorax (of any type) that leads to the heart and lungs not working properly. It is a medical emergency.
Spontaneous pneumothorax causes
Spontaneous means the pneumothorax was not caused by an injury such as a rib fracture. Primary spontaneous pneumothorax is likely due to the formation of small sacs of air (blebs) in lung tissue that rupture, causing air to leak into the pleural space. Air in the pleural space creates pressure on the lung and can lead to its collapse. A person with this condition may feel chest pain on the side of the collapsed lung and shortness of breath.
Blebs may be present on an individual’s lung (or lungs) for a long time before they rupture. Many things can cause a bleb to rupture, such as changes in air pressure or a very sudden deep breath. Often, people who experience a primary spontaneous pneumothorax have no prior sign of illness; the blebs themselves typically do not cause any symptoms and are visible only on medical imaging. Affected individuals may have one bleb to more than thirty blebs. Once a bleb ruptures and causes a pneumothorax, there is an estimated 13 to 60 percent chance that the condition will recur.
Spontaneous pneumothorax signs and symptoms
Spontaneous pneumothorax most commonly presents without severe symptoms.
Patients with a collapsed lung may experience a sudden onset of the following symptoms:
- Sharp chest pain, made worse by a deep breath or a cough
- Shortness of breath
A larger pneumothorax will cause more severe symptoms, including:
- Chest tightness
- Easy fatigue
- Rapid heart rate
- Bluish color of the skin caused by lack of oxygen
- Nasal flaring
- Chest wall retractions.
Until a bleb ruptures and causes pneumothorax, no clinical signs or symptoms are present in primary spontaneous pneumothorax. Young and otherwise healthy patients can tolerate the main physiologic consequences of a decrease in vital capacity and partial pressure of oxygen fairly well, with minimal changes in vital signs and symptoms, but those with underlying lung disease may have respiratory distress.
In one series, acute onset of chest pain and shortness of breath were present in all patients in one series; typically, both symptoms are present in 64-85% of patients. The chest pain is described as severe and/or stabbing, radiates to the ipsilateral (same side) shoulder and increases with inspiration (pleuritic).
In primary spontaneous pneumothorax, chest often improves over the first 24 hours, even without resolution of the underlying air accumulation. Well-tolerated primary spontaneous pneumothorax can take 12 weeks to resolve. In secondary spontaneous pneumothorax, the chest pain is more likely to persist with more significant clinical symptoms.
Shortness of breath/dyspnea in primary spontaneous pneumothorax is generally of sudden onset and tends to be more severe with secondary spontaneous pneumothorax because of decreased lung reserve. Anxiety, cough, and vague presenting symptoms (e.g, general malaise, fatigue) are less commonly observed. The most common underlying abnormality in secondary spontaneous pneumothorax is chronic obstructive pulmonary disease (COPD), and cystic fibrosis carries one of the highest associations, with more than 20% reporting spontaneous pneumothorax.
Despite descriptions of Valsalva maneuvers and increased intrathoracic pressures as inciting factors, spontaneous pneumothorax usually develops at rest. By definition, spontaneous pneumothorax is not associated with trauma or stress. Symptoms of iatrogenic pneumothorax are similar to those of a spontaneous pneumothorax and depend on the age of the patient, the presence of underlying lung disease, and the extent of the pneumothorax.
A history of previous pneumothorax is important, as recurrence is common, with rates reported between 15% and 40%. Up to 15% of recurrences can be on the contralateral (opposite) side. Secondary pneumothoraces are often more likely to recur, with cystic fibrosis carrying the highest recurrence rates at 68-90%. No study has shown that the number or size of blebs and bullae found in the lung can be used to predict recurrence.
Spontaneous pneumothorax diagnosis
If your child has a sudden onset of shortness of breath or sharp chest pain that is worsened by breathing, go to the Emergency Department to be evaluated or call 911. In order to make an accurate diagnosis, the medical team will evaluate your child’s symptoms and perform a physical exam, including the following:
- History: Your physician will obtain your child’s full medical history, in addition to assessing the symptoms she is currently experiencing. You may be asked questions about when the symptoms started, the severity of the pain or shortness of breath, and length of time you waited prior to arriving to the Emergency Department.
- Physical exam: Using a stethoscope, your child’s physician will listen for decreased or no breath sounds on the affected side.
- Chest X-ray: This radiologic test will show a pneumothorax if it is present.
Physical Examination
The presentation of a patient with pneumothorax may range from completely asymptomatic to life-threatening respiratory distress. Symptoms may include diaphoresis, splinting chest wall to relieve pleuritic pain, and cyanosis (in the case of tension pneumothorax). Findings on lung auscultation also vary depending on the extent of the pneumothorax. Affected patients may also reveal altered mental status changes, including decreased alertness and/or consciousness (a rare finding).
Respiratory findings may include the following:
- Respiratory distress (considered a universal finding) or respiratory arrest
- Tachypnea (or bradypnea as a preterminal event)
- Asymmetric lung expansion – A mediastinal and tracheal shift to the contralateral side can occur with a large tension pneumothorax
- Distant or absent breath sounds – Unilaterally decreased or absent lung sounds is a common finding, but decreased air entry may be absent even in an advanced state of the disease
- Lung sounds transmitted from the unaffected hemithorax are minimal with auscultation at the midaxillary line
- Hyperresonance on percussion – This is a rare finding and may be absent even in an advanced state of the disease
- Decreased tactile fremitus
- Adventitious lung sounds (crackles, wheeze; an ipsilateral finding)
Cardiovascular findings may include the following:
- Tachycardia – This is the most common finding. If the heart rate is faster than 135 beats/min, tension pneumothorax is likely
- Pulsus paradoxus
- Hypotension – This should be considered as an inconsistently present finding; although hypotension is typically considered a key sign of a tension pneumothorax, studies suggest that hypotension can be delayed until its appearance immediately precedes cardiovascular collapse
- Jugular venous distention – This is generally seen in tension pneumothorax, although it may be absent if hypotension is severe
- Cardiac apical displacement – This is a rare finding.
Tension pneumothorax
Although tension pneumothorax may be a difficult diagnosis to make and may present with considerable variability in signs, respiratory distress and chest pain are generally accepted as being universally present, and tachycardia and ipsilateral air entry on auscultation are also common findings. Sometimes, reliance on history alone may be warranted.
Findings may be affected by the volume status of the patient. In hypovolemic trauma patients with ongoing hemorrhage, the physical findings may lag behind the presentation of shock and cardiopulmonary collapse. Increased pulmonary artery pressures and decreased cardiac output or cardiac index are evidence of tension pneumothorax in patients with Swan-Ganz catheters.
When examining a patient for suspected tension pneumothorax, any clue may be helpful, as subtle thoracic size and thoracic mobility differences may be elicited by performing careful visual inspection along the line of the thorax. In a supine patient, the examiner should lower themselves to be on a level with the patient.
Tracheal deviation is an inconsistent finding. Although historic emphasis has been placed on tracheal deviation in the setting of tension pneumothorax, tracheal deviation is a relatively late finding caused by midline shift.
Abdominal distention may occur from increased pressure in the thoracic cavity producing caudal deviation of the diaphragm and from secondary pneumoperitoneum produced as air dissects across the diaphragm through the pores of Kohn.
If patients who are mechanically ventilated are difficult to ventilate during resuscitation, high peak airway pressures are clues to pneumothorax. A tension pneumothorax causes progressive difficulty with ventilation as the normal lung is compressed. On volume-control ventilation, this is indicated by marked increase in both peak and plateau pressures, with relatively preserved peak and plateau pressure difference. On pressure control ventilation, tension pneumothorax causes sudden drop in tidal volume. However, these observations are neither sensitive nor specific for making the diagnosis of pneumothorax or ruling out the possibility of pneumothorax.
The development of tension pneumothorax in patients who are ventilated will generally be of faster onset with immediate, progressive arterial and mixed venous oxyhemoglobin saturation decline and immediate decline in cardiac output. Cardiac arrest associated with asystole or pulseless electrical activity (PEA) may ultimately result. Occasionally, the tension pneumothorax may be tolerated and its diagnosis delayed for hours to days after the initial insult. The diagnosis may become evident only if the patient is receiving positive-pressure ventilation. Tension pneumothorax has been reported during surgery with both single- and double-lumen tubes.
Spontaneous pneumothorax treatment
Treatment of spontaneous pneumothorax depends on the duration, severity of symptoms and size of pneumothorax.
Patients who seek treatment for minimal or resolving symptoms after more than 24 hours will receive a chest X-ray to determine treatment. If the imaging reveals only a small pneumothorax, the patient may only require oxygen supplementation and observation in the hospital for a brief period of time.
Patients with large pneumothorax who seek treatment within a short time of the onset and present more severe symptoms may require placement of a chest tube (inserted between the ribs) to release the tension. In most cases, the placement of the chest tube allows the lung to re-expand fully and quickly.
The chest tube can be left in place for several days. During that time, your child must stay in the hospital for continued evaluation. She will undergo a series of chest X-rays to monitor the pneumothorax and determine if it is improving or worsening.
Some patients with a pneumothorax may also receive supplemental oxygen, which may improve symptoms and can help the air around the lung be reabsorbed more quickly.
Patients with a persistent air leak from the chest tube for more than five days or those with recurrent or bilateral spontaneous pneumothorax may be candidates for surgery.
A tension pneumothorax should be treated with immediate decompression with a needle in the 2nd intercostal space (between the second and third rib at the front). This is then followed by a formal intercostal tube insertion as above.
Surgery for spontaneous pneumothorax
Patients with a persistent air leak from the chest tube for more than five days or those with recurrent or bilateral spontaneous pneumothorax may be candidates for surgery.
Goals of surgery:
- Identify bullae (blebs) responsible for the air leak and remove them if they are present.
- Obliterate the pleural space and minimize the chances for future lung collapse.
The operation is usually performed using a video-assisted thoracic surgery (VATS), with two to four small incisions.
After surgery
After your child has surgery to treat spontaneous pneumothorax, she will spend an hour or so recovering in the post-acute care unit before returning to a room in the hospital. She will likely have a chest tube after the operation, which may need to remain in place for a number of days.
Your child will experience some pain and will receive pain medications throughout the stay. Some patients will initially require IV pain medications and then transition to oral pain medications. The pain management team will work with the surgical team and your child to provide adequate pain control.
Your child may have chest incisions with a clear adhesive glue dressing or gauze covering the site. The clear adhesive will dissolve and peel off naturally; the gauze dressings will be removed 48-72 hours after surgery.
Follow-up care
If your child has an operation or receives inpatient treatment with a chest tube or oxygen therapy to treat spontaneous pneumothorax, you will need to make an appointment to see the surgeon for follow-up three to four weeks after discharge. After your child has been treated for spontaneous pneumothorax, it is important that you carefully monitor her health.
After your child has been treated for spontaneous pneumothorax, it is important that you carefully monitor her health. See your doctor if your child experiences any of the following symptoms:
- Fever greater than 101 °F (> 38.3 °C)
- Signs of infection of incision sites, including: redness, yellow or green discharge, tenderness, warmth or foul odor
- Any other concerns
If your child suffers any of the following signs or symptoms, she must be brought to the Emergency Department as quickly as possible to receive proper treatment:
- Sudden onset of chest pain
- Shortness of breath or difficulty breathing








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}