Contents
Orchidopexy
An orchidopexy is an operation for undescended testicles (also called cryptorchidism). An undescended testicle means that the testicle has not dropped down to its normal place in the scrotum. It is necessary for your child to have surgery to relocate the testicle to the scrotum and fix it into place to keep it in the correct position. Your son may need to have this operation on unilateral orchidopexy (one testicle) or bilateral orchidopexy (both testicles).
Orchidopexy operation usually does not require an overnight stay at the hospital. Boys will have to avoid strenuous activity for a few days after the operation. Parents will have to clean and change the bandage at the incision site.
Normally before a baby boy is born, the testicles move into the scrotum (the sac that holds the testicles).
The undescended testicle can usually be palpated in the inguinal canal. In a minority of patients, the missing testicle may be located in the abdomen or be nonexistent.
Undescended testicles are associated with decreased fertility (bilateral cases), increased testicular germ cell tumors (overall risk under 1%), testicular torsion, inguinal hernias, and psychological problems 1).
Infertility
Men with undescended testes may have reduced fertility, even after orchiopexy 2).
- The infertility rate for unilateral cases is not believed to be very different from the general population.
- The fertility reduction after orchiopexy for bilateral cryptorchidism is about 38%. This is the basis for the universal recommendation for early surgery due to degeneration of spermatogenic tissue and reduced spermatogonia counts after the second year of life in patients with untreated undescended testes.
Psychological consequences
Boys with undescended testicles do not tend to be effeminate, gender-disordered, or pre-homosexual. A disturbed self-image may occur when the family dynamics are destructive toward male self-esteem. When cryptorchism is surgically corrected, a healthy masculinity generally occurs.
Testicular cancer
Overall, the risk of testicular cancer if orchiopexy is done before puberty is around 2 to 3 times that of the general population. It is 5 to 6 times higher when orchiopexy is done after puberty. The risk of cancer does not seem to be different when orchiopexy is done early in infancy compared to later in childhood 3).
- The most common type of testicular cancer in untreated undescended testes is seminoma.
- The peak age range for this tumor is 15 to 45 years.
- In contrast, after orchiopexy, seminomas represent only 30% of testicular tumors in previously undescended testes.
- It is treatable if caught early, so boys who had an orchiopexy as infants should be taught testicular self-examination.
Without surgical correction, an undescended testicle may descend during the first three months of life. To reduce risks, undescended testes may be brought into the scrotum with an orchiopexy.
Cryptorchidism, hypospadias, testicular cancer, and poor semen quality make up testicular dysgenesis syndrome. This syndrome is thought to be due to harmful environmental factors that disrupt embryonal programming and gonadal development during fetal life.
Figure 1. Male reproductive system
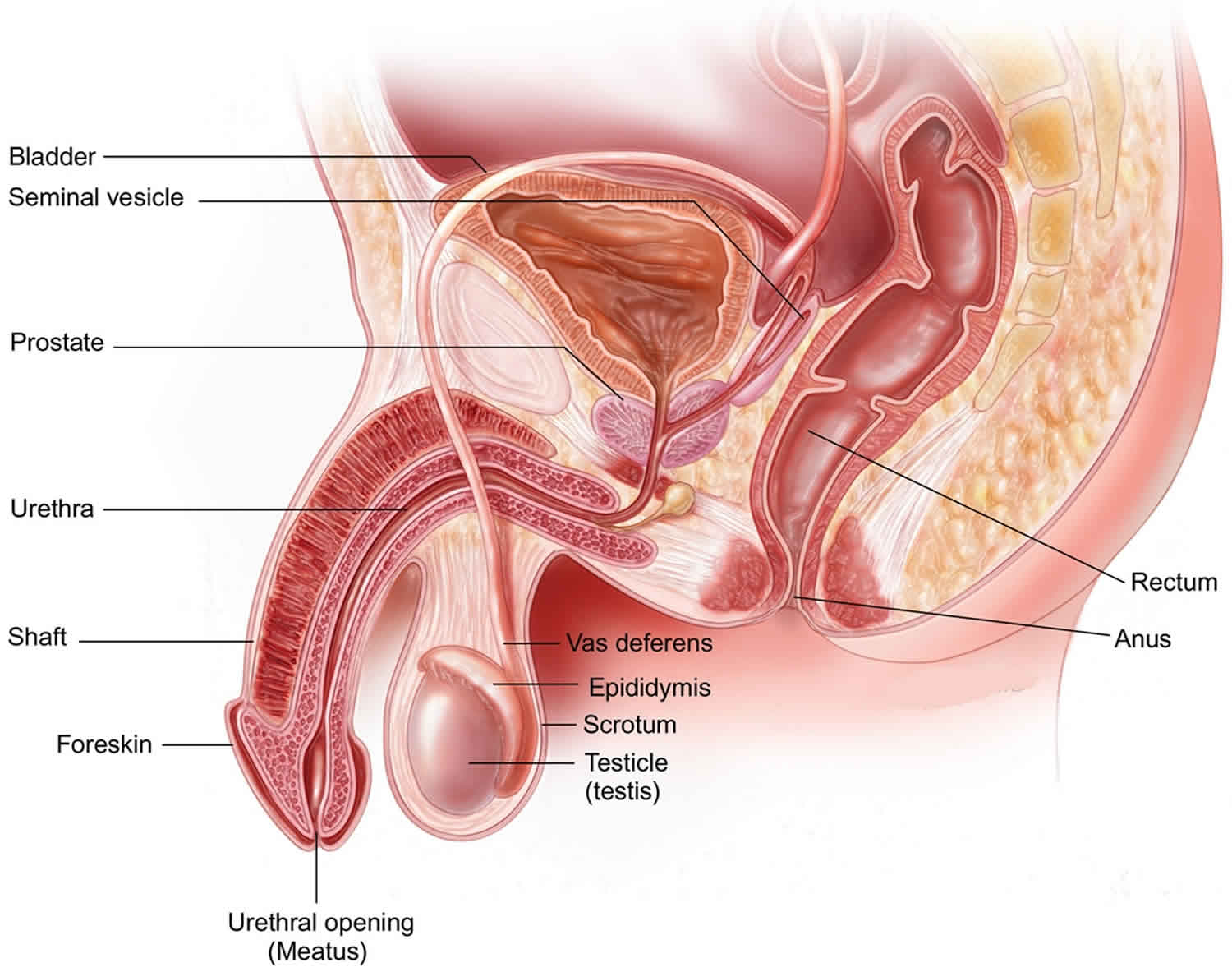
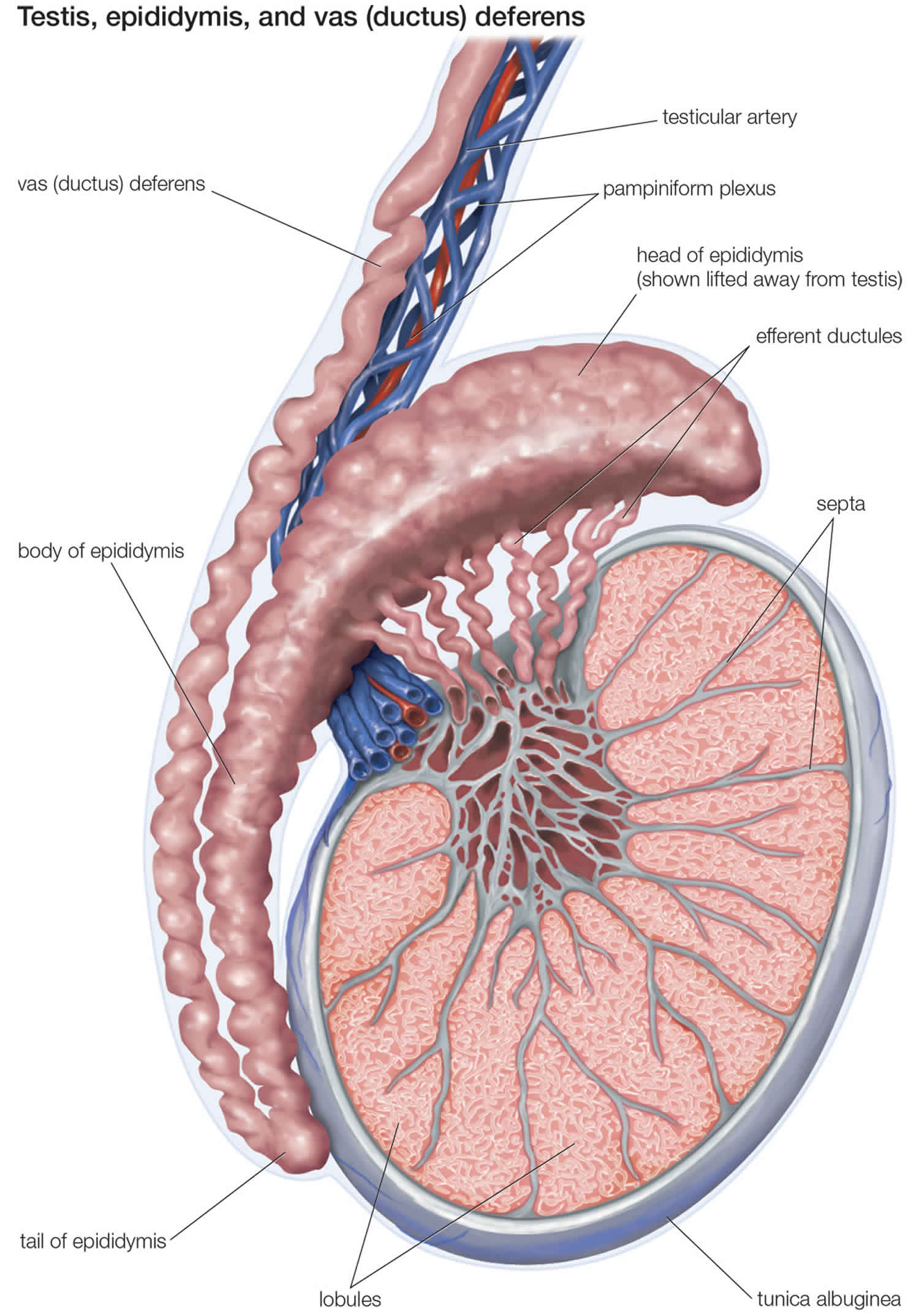
Figure 2. Testis anatomy
Most children have no problems getting better after their operations. Your child’s scrotum may be swollen and bruised after the operation. This will go away after a few days. Some children get infections in the scrotum or in their incision lines, the place where the doctor cut through the skin to operate. Your child may have an infection if he has one or more of these signs:
- increased pain at the incision line
- a red incision line
- swelling or puffiness at the incision line
- liquid leaking from the incision line
- a fever higher than 101 °F (38.3°C)
- vomiting (throwing up)
- stomach pain or stomach ache
- loss of appetite
- tiredness or no energy
If your child has one or more of these signs, see your child’s doctor.
Sometimes, a testicle will twist or rise up again after the operation. A doctor must see your child right away if he has any of these signs:
- has severe pain or swelling
- has difficulty or is unable to urinate (pee)
Take your child to the emergency room in the hospital and ask for the surgeon on call if you are worried that your child’s testicle is twisted or has risen up.
What happens during the orchidopexy operation?
Your child will be given a special “sleep medicine” called a general anesthetic. This will make sure that he sleeps during the operation.
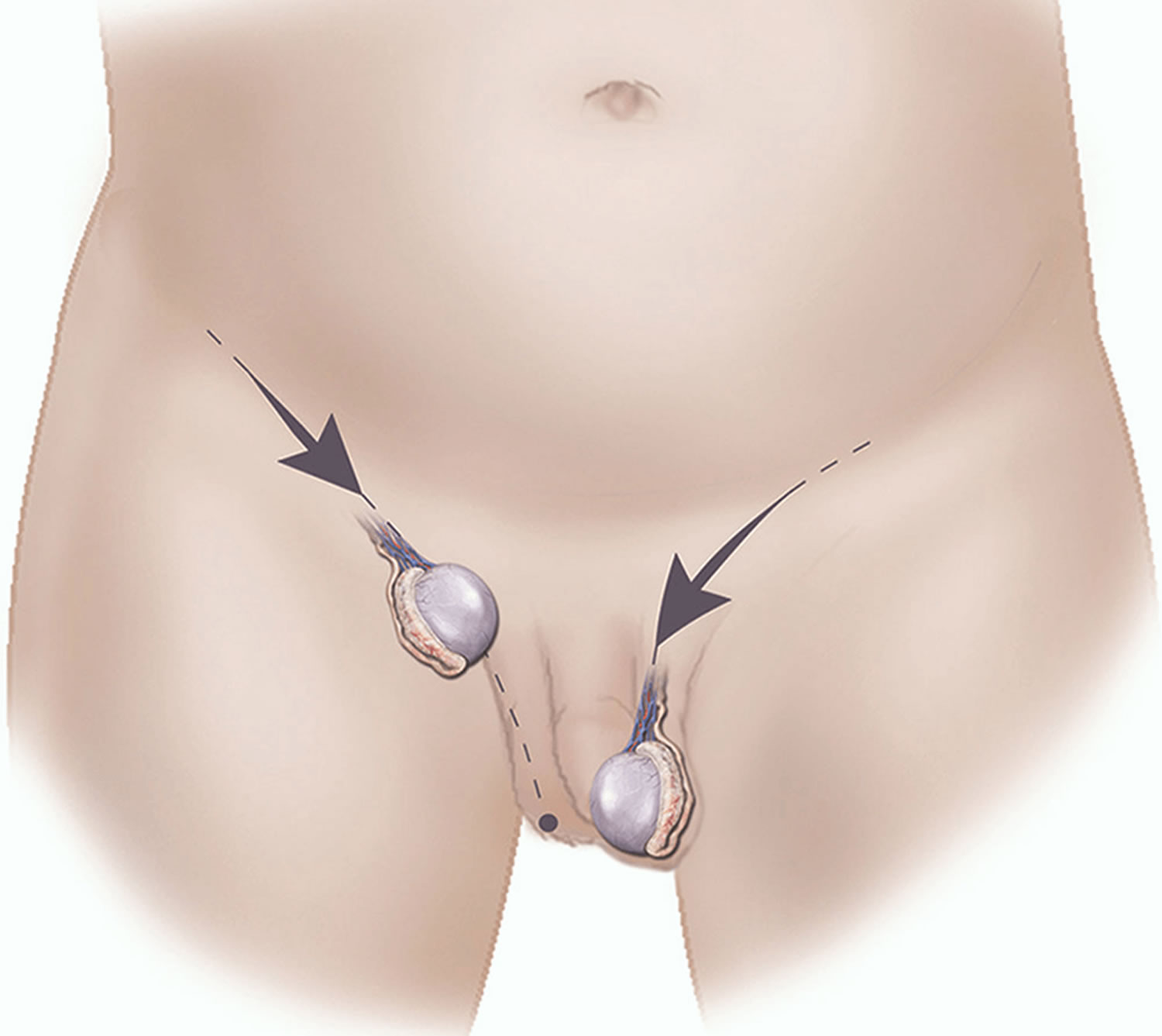
The doctors will make a small incision (cut) in the area at the top of your child’s leg, called the groin. They will gently move your son’s testicle into the scrotum. If both testicles need descending, there will be two incisions, one on each side of the groin.
The orchidopexy operation usually takes about one hour per testicle.
Usually an orchidopexy is an out-patient operation. This means the operation is done on the day that your child comes to the hospital. Your son will have to spend a few hours waking up from the surgery. Your son can probably go home after the operation. He will not stay in the hospital overnight.
Orchiopexy technique
For palpable undescended testes, an inguinal or scrotal orchiopexy is recommended 4).
- An incision is made in the high scrotum, median scrotal raphe, high edge of the scrotum, or groin. Many different type of retractors can be used depending of the size of the incision. Inguinal incisions can be as small as 1 cm. Scrotal incisions can be larger as they tend to heal concealed specially when in the median raphe.
- The testis can be approached first or the cord first; for scrotal cases, the testis is found first. For an inguinal approach, the testis can be approached first or the external oblique fascia opened proximal to the external ring and the cord approached first.
- When approaching the testis first, all the cremasteric muscles are divided as well as everything not going into the external ring.
- The more difficult part of the case is separating the hernia sac from the vas and testicular vessels. This can be approached anteriorly or posteriorly. The posterior approach is much easier to teach and learn.
- How the testis is positioned and secured in the scrotum varies. Most would agree that a sub-dartos pouch is desirable. Some surgeons do not suture the testis in place, others use absorbable sutures, others non-absorbable, and others just close the passage into the groin.
For nonpalpable testes under anesthesia, exploratory laparoscopy is recommended. If a testis is found during exploratory laparoscopy, the options are 5):
- Laparoscopic orchiopexy preserving the vessels: the testis is dissected off a triangular pedicle containing the gonadal vessels and the vas deferens.
- Laparoscopic one stage Fowler Stevens orchiopexy: gonadal vessels are divided and the testis is dissected off a pedicle of the vas and brought down in one stage.
- Laparoscopic two stage Fowler Stevens orchiopexy: vessels are divided with clips but dissection of the testis is postponed for 6 months to allow for optimal development of collaterals.
If no testis is found during exploratory laparoscopy, one has to determine the presence of either blind ending vessels or a testicular nubbin to completely rule out a missing testis. The vas can be dissociated from the testis and thus is not always a good guide to find the gonad 6).
If the internal ring is closed but vessels are going into it, a scrotal exploration usually will find a testicular nubbin. Look for a small structure with a brown spot.
If vessels are going into an open inguinal ring, one can usually push the testis into the abdomen but if not, an inguinal or scrotal exploration would be warranted.
Caring for your child at home after the orchidopexy operation
Pain relief
Your son will probably feel soreness in his groin for the first few days after the operation. Your child’s doctor may prescribe codeine for the pain. You can also give your child acetaminophen or ibuprofen for pain. Give him this medicine exactly as your doctor tells you.
Signs your child is in pain
Older children can usually tell you if they have pain. In younger children, look for these signs of pain:
- a lot of fussiness
- increased sweating
- pale skin color
- refusing to walk or trouble walking
- unusually quiet behavior
Taking care of the stitches
Your son will have a bandage over the incision site or sites. These bandages cover the stitches. You may see a small amount of blood on the bandage. This is normal. The bleeding will gradually stop. Keep the incision area dry and clean. Shower or shallow tub bathing are OK. Do not put the incision or dressing under the water for 2 weeks.
After a few days, you can soak the bandage off in the bathtub.
Once the bandage has been removed, clean the incision site twice a day. The nurse will give you instructions on how to do this.
- Using a clean wet cloth, gently pat the incision site clean.
- Put an antibiotic ointment such as Polysporin lightly over the stitches for one week. An antibiotic ointment is a special cream that kills germs. You can buy antibiotic creams at the pharmacy without a prescription.
- The stitches will dissolve and do not need to be removed.
If your child is still in diapers, you should change them when they are wet. Leave the diaper off for about 30 minutes every day. If your child is older, he can eat his regular food. Your child should have a bowel movement (poop) every day.
Food and Drink
For Children:
- Continue with water, clear fruit juices or popsicles. If the child has no trouble with these, you can slowly begin to give solid foods.
For Infants:
- Infants may have clear liquids such as water, Pedialyte® or watered-down apple juice (mix half water and half juice) or breast milk. If your infant has no trouble with these, he may have regular formula or continue with breast milk. Infants may need to be burped more often than usual the first day after surgery.
Your child’s activities
Your child should avoid certain activities that might harm the incision until after his check-up in the clinic. These activities include:
- strenuous activities
- contact sports such as football or hockey
- riding a bicycle
After a few weeks, your child will be able to resume all his normal physical activities.
Follow-up care
Your child will need a check-up at the clinic. Staff at the hospital will make an appointment for your son to come in for a check-up to make sure he is getting well. If you are not given an appointment, ask.
When you suspect a problem
Talk to a doctor if you have any concerns. Call your child’s surgeon, the doctor who did your child’s operation.
Orchidopexy operation risks
Risks for any anesthesia are:
- Reactions to medicines
- Problems breathing
Risks for any surgery are:
- Bleeding
- Infection
Risks for orchidopexy surgery include:
- Shrinkage of the testicle or failure of the testicle to grow to normal size.
- Inability to bring the testicle into the scrotum, resulting in the removal of the testicle.
References [ + ]





{kind=link}