Contents
- Mitrofanoff
- Why is the Mitrofanoff urinary diversion done?
- Mitrofanoff urinary diversion procedure benefits
- Preparing for the Mitrofanoff urinary diversion operation
- Mitrofanoff urinary diversion operation
- After the Mitrofanoff urinary diversion operation
- Learning to use the catheter and Mitrofanoff
- Mitrofanoff procedure risks
Mitrofanoff
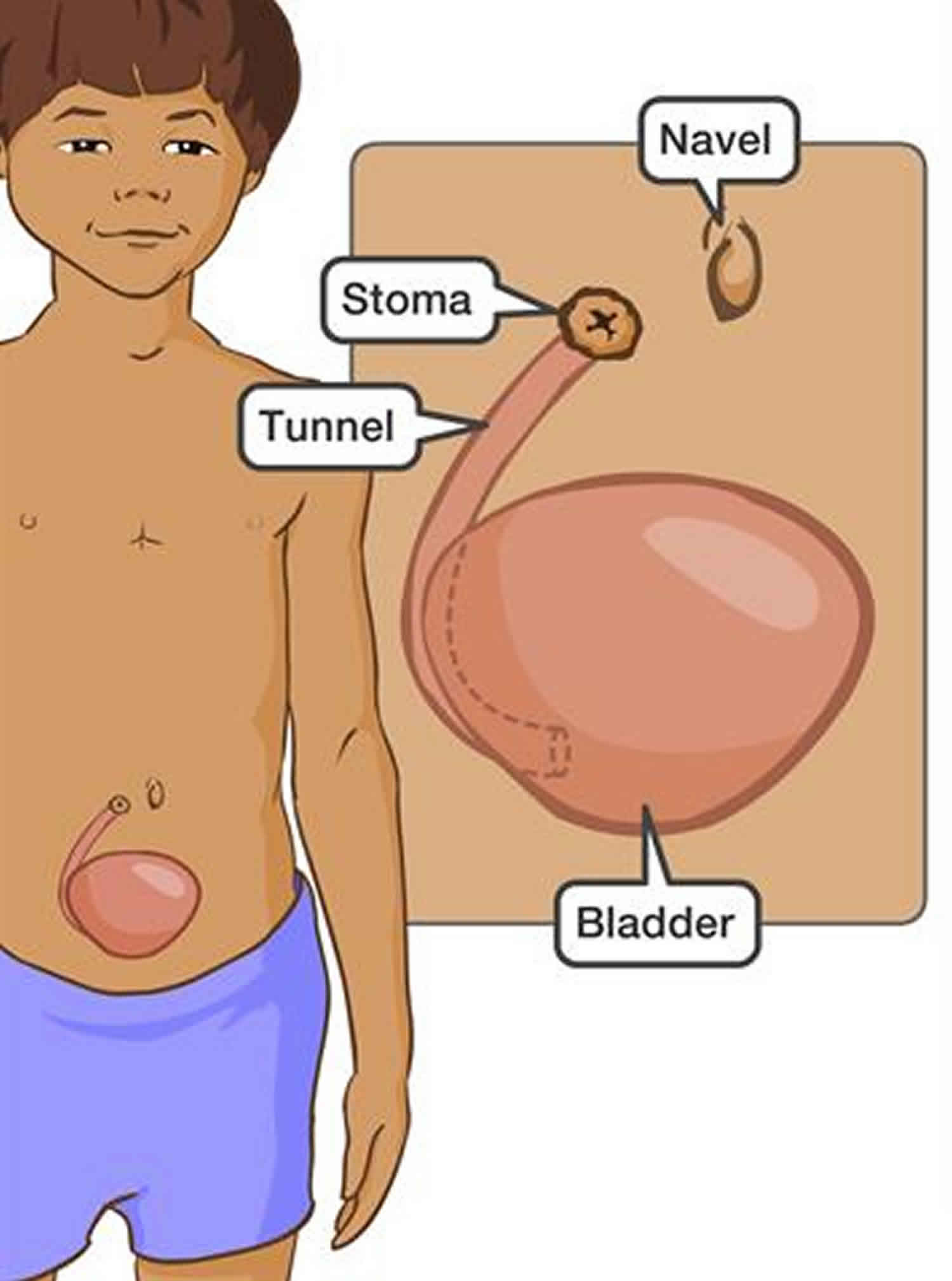
Mitrofanoff also called appendico vesicostomy, is a surgical procedure that creates a channel or tunnel from the bladder to outside the body on a child’s belly through which a child can urinate (pee) by using a catheter (putting a small tube into the new channel or tunnel) 1). The new channel or tunnel is made from the appendix. It connects the bladder to a small hole created in the belly button or in an area in the lower belly. This way, children can empty their bladders by catheterizing through the new tube instead of using the urethra (the tube that pee normally goes through when it leaves the body). Mitrofanoff procedures require a stay of 4 to 7 days at the hospital.
During the surgery, the appendix is cut away from the intestine but not from its blood supply. The surgeon sews one end of the appendix to the back side of the bladder. The other end of the appendix is then pulled up and attached to the belly. A small hole is made on each end of the new tube (one on the belly or in the belly button, one in the bladder) so that children can put in a catheter through the opening on their belly or belly button to empty the bladder.
There are two possible ways the surgery may be done:
- Open surgery – A small cut (a couple of centimeters wide) is made in the lower belly. The skin is pulled aside so the surgeon can see and work directly on the child. This is the only surgical technique used in many hospitals. However, Nationwide Children’s Hospital reserves open surgery only for patients who are not good candidates for minimally invasive surgery.
- Robotic surgery – Several tiny cuts (several millimeters wide) are made in the belly. The surgeon uses a computer to control the robotic arms, which move small tools underneath the skin to do the operation.
The Mitrofanoff procedure is often done at the same time as other operations. Mitrofanoff operation is usually onlydone as part of another procedure, in particular:
- when enlarging your bladder with a bowel patch (enterocystoplasty);
- when a neobladder (new bladder) has been fashioned from bowel after removal of your bladder for cancer.
There are many reasons a child may need a Mitrofanoff, such as:
- Birth defects
- Injury
- Cancer
- Trouble or pain with using a catheter through the urethra. The urethra is the tube that normally carries urine (pee) out of the bladder.
- Spina bifida and myelomeningocele
- Spinal cord injuries
- Neurogenic bladder or non-neurogenic neurogenic bladder (Hinman syndrome).
You should call the doctor or seek medical attention for your child after the Mitrofanoff procedure if your child:
- Has a fever of 101°F (38.3 °C) or higher before the first follow-up visit
- Cannot pass urine through the catheter
- Passes blood through the catheter
- Accidentally pulls the catheter out
- Complains of severe pain in the belly, side or back that isn’t helped by the pain medicine they are given at discharge
- Has symptoms of a urinary tract infection (UTI) or kidney infection
- Feels pain or a blockage when catheterizing (once the surgery catheter is removed).
Why is the Mitrofanoff urinary diversion done?
The Mitrofanoff procedure is done for children who can not urinate on their own. Many of these children use traditional catheters before surgery. These catheters are inserted through the urethra, the normal place pee exits the body. However, catheters through the urethra can cause pain in boys and may be difficult for girls to put in because of their anatomy. Girls who use wheelchairs are often not able to put in a catheter unless they sit on a toilet, which can make them less independent.
In some cases, children for whom it is difficult to catheterize through the urethra may stay in diapers. In others, the sphincter muscles do not work well and the child continues to leak into a diaper. Diapers can become socially uncomfortable for children as they age. The smell of urine and its impact on the skin and any wounds in the diaper area can lead to low quality of life.
After a Mitrofanoff procedure, children can empty their bladders without diapers, without needing to transfer to a toilet, and without catheterizing through the urethra. This makes it easier and more comfortable for many children to empty their bladders. They can stay dry between catheterizations. In the case of many wheelchair users, it allows more independence, since children can catheterize themselves through the opening on their belly or in their belly button.
Mitrofanoff procedures are often done for children with:
- Spina bifida and myelomeningocele
- Spinal cord injuries
- Neurogenic bladder or non-neurogenic neurogenic bladder (Hinman syndrome)
- Birth defects
- Injury
- Cancer
- Trouble or pain with using a catheter through the urethra. The urethra is the tube that normally carries urine (pee) out of the bladder.
What are the alternatives to Mitrofanoff urinary diversion?
- Intermittent self-catheterization in men-or in women
- Urostomy– diverting your urine straight on to the surface of your abdomen (tummy) so that it drains into a bag
Mitrofanoff urinary diversion procedure benefits
Mitrofanoff procedures allow intermittent urinary catheterization – once every few hours. This offers a lower risk of infection than a permanent (indwelling) catheter and allows one to not leak urine continually like an ileovesicostomies, which drain from a hole (stoma) in the belly into a bag.
After mitrofanoff, children do not have to wear diapers and can stay dry between catheterizations. They can often empty their bladders independently and without transfer to a toilet. The opening in the belly is very small; most are hard to see even when looking at the belly. All of these characteristics of the Mitrofanoff procedure may help it improve children’s quality of life.
Preparing for the Mitrofanoff urinary diversion operation
The Mitrofanoff procedure is not an emergency surgery. Your surgeon will schedule the operation in advance. Before any operation, patients often have to do specific things to prepare. Staff at the hospital will tell you what you need to do before the operation. They will give you a brochure or pamphlet to read. If you do not get this information, ask. If you have more questions after reading the pamphlet, ask.
Because the surgeon will cut out your child’s appendix, it is important to make sure that your child’s bowel is as clean as it can be before the operation. Getting the bowel as clean as possible means restricting what your child eats and having enemas.
Eating and drinking
For two to three days before the operation, your child should only have clear fluids to drink. Clear fluids are liquids you can see through, like water, apple juice, ginger ale, Sprite, Jello and freezies. Your child cannot have anything else to eat or drink.
- Write the date of your child’s operation.
- Write the date your child must start having only clear fluids.
Enemas
Your child will need to have several enemas. An enema means that a small tube is put into your child’s anus and water is flushed inside. Then, your child will go to the bathroom and expel the water and feces (poop) from the bowel. Usually, enemas are a bit uncomfortable but they do not hurt.
Mitrofanoff urinary diversion operation
The day of the operation, your child will be pre-admitted at the Urology Unit. Your child can have only clear liquids to drink.
Your child will be given another enema.
Your child will be given a special “sleep medicine” called a general anesthetic during the operation. This means that your child will sleep and will feel no pain during the procedure.
Mitrofanoff surgery usually takes about two to six hours. Your surgeon will speak to you about this before the surgery.
After the Mitrofanoff urinary diversion operation
When your child goes back to the Urology Unit from the operating room, they will have an intravenous line (IV). An IV is a tiny plastic tube that is placed in a vein in the hand or arm. For the first few days after the operation, your child will get the liquids and medicines they need through the IV.
Your child will may also have some of the following.
- Nasogastric tube. Your child will have a nasogastric tube. The tube usually stays in place for about one week. Your child’s stomach must stay empty and have a chance to rest after the operation.
- Suprapubic catheter. Your child will have a suprapubic catheter after the operation. This catheter is a small tube that goes through the skin of the belly into the bladder. All the urine that would normally be stored in the bladder drains out through this tube and into a bag called a urine collection bag. This catheter will be taken out at the urology clinic, usually about one week after the Mitrofanoff operation. Your child will not need an operation to take out the catheter.
- Stents. Your child may have ureteral stents. These are small plastic tubes that sit in the ureters. The ureters are the tubes between the kidneys and the bladder. The ureteral stents let all the urine drain from the kidneys and give your child time to heal. Your child will need an operation to take out the stents, usually six to eight weeks after the Mitrofanoff operation.
- Urinary catheter. Your child will have a urinary catheter inside the Mitrofanoff. It may or may not be attached to a urine collection bag.
Incision, stitches and gauze
Your child’s incision will be closed with stitches. The incision is the place where the surgeon cuts through the skin to operate. The stitches will dissolve about 10 days after the operation.
The incision and the stitches will be covered with white gauze. The nurse will change the gauze every day.
Penrose drain
A drain called a Penrose drain may be placed in your child’s belly, close to the incision. It takes away the extra liquids that may collect during the operation. This drain looks a lot like a thick elastic band. It will be stitched in place and covered with a piece of gauze.
Your surgical team will take out this drain before your child goes home.
Managing your child’s pain
There are several ways to control pain that work well. Which way we use will depend on your child’s age and needs.
- Your child may get medicine for pain through the IV.
- Your child may have an epidural catheter. An epidural catheter is a small plastic tube that an anesthesiologist puts into a space in the spine. (The anesthesiologist is the doctor who gives sleep medicine to take away the pain.) The catheter is put in in the operating room. This catheter lets your child have medicine for pain all the time. The epidural catheter works well because it numbs the body below the incision.
- Once your child feels better, they can swallow their pain medicine.
Bladder spasms treatments
Catheters and stents may bother the bladder and cause cramps, called bladder spasms. Sometimes bladder spasms can hurt a lot. If your child has painful bladder spasms, they will be given a medicine called a B&O suppository. This medicine relaxes the bladder and reduces the pain.
Symptoms of bladder spasms
Signs that your child is having bladder spasms may include:
- pain that comes on quickly and then stops
- an itchy bottom
- the need to urinate or have a bowel movement (poo) often
- your child holding or rubbing their genitals (private parts) more than usual
- urine leaking around the catheter
- drawing the knees up to the chest, especially in babies and toddlers
The nurse will check your child’s pain control regularly. But you know your child best. The nurse will want to know if you think your child’s pain is being controlled well. If you feel your child is in pain, tell the nurse.
Getting active again
Right after the operation, your child will have to stay in bed all day and all night. Your child may not be allowed to sit up for one or two days. While your child is lying in bed, they should try to do these things:
- take deep breaths and cough
- exercise their legs
- roll from side to side
The nurse will help.
The doctor will decide when your child is ready to get out of bed. Your child will have to become active slowly. Your child can start by sitting in a chair. Then they can slowly start to walk when they are ready.
Eating and drinking after the operation
Your child’s bowel needs to rest after the operation. So your child will not be able to eat or drink for a while. When they begin to feel grumbling in the stomach and passes gas, the doctor will take out the nasogastric tube.
Your child will be allowed only clear liquids at first. They can eat normal food after a few days.
Your child must drink as much liquid as possible. This will help the catheters drain well.
What can I expect when my child get home?
- you must leave the catheter through your Mitrofanoff channel in place, even if it is not draining urine
- you will usually be discharged with one or two catheters in your bladder
- your surgical team may instruct you to flush the catheters to keep them draining well
- you should check daily that your catheters are draining normally
- if they block with mucus plugs, they must be flushed out and unblocked as soon as possible
- your doctor will arrange for your stitches or clips to be removed seven to 10 days after the procedure
- a follow-up appointment will be made for you to have your catheter(s) removed after two to three weeks; your doctor often do a cystogram (a dye X-ray of your bladder) before removing your catheter(s) to make sure everything has healed
- you may see blood in your urine for up to a month after the procedure
- women may see some vaginal discharge over the same period of time
- you will need at least six weeks off work, longer if your job is physically strenuous
- you should not have sexual intercourse for four weeks
- you should avoid straining or heavy lifting for six weeks
- you will be given a copy of your discharge summary and a copy will also be sent to your family doctor
- any antibiotics or other tablets you may need will be arranged and dispensed from the hospital pharmacy
Once everything has healed completely, your doctor will remove the catheter in your Mitrofanoff channel and teach you how to pass a similar catheter in and out to empty your bladder/neobladder. If you have any difficulty with this at home, you should contact your surgical team.
Follow-up care after a Mitrofanoff urinary diversion procedure
Your child’s catheters must stay in place for 3 to 4 weeks after the surgery. This allows the swelling to go down and the cuts and new tube to heal. You will have to return to the hospital for a nurse to remove the catheters. You and your child will also receive training from a nurse to learn how and when to catheterize using the new tube through the belly button. The nurse will provide some initial supplies and connect you with resources for home shipping for supplies in the future.
About 1 month after the surgical catheters come out, your child will need a follow-up ultrasound to check for swelling in the kidneys. This will let the doctor know if the surgery worked to effectively drain your child’s urine. Your child will also need an ultrasound at least every year to keep checking kidney health.
You should also expect the following after the Mitrofanoff procedure:
- The cut skin is usually closed with internal, absorbable stitches and skin glue (except for the new hole on the belly where the but connects, which stays open). The stitches disappear on their own and do not require any special removal or care.
- Your child can wash by sponge bath for the 2 days following the surgery. After that, showers are acceptable. Once the catheters are removed, baths are also okay.
- The cuts and catheters may be sore for a few days or weeks.
- Gym class, strenuous activity and heavy lifting should be avoided until the catheter is removed.
- Wheelchair transfers can begin again about 2 weeks after the operation.
- Your child must rinse (irrigate) the bladder once a day. This will be part of your child’s new routine. The rinse helps clear out mucus made by the appendix tube. If your child does not rinse the bladder, he or she may get kidney stones or infections.
Learning to use the catheter and Mitrofanoff
When your doctor feels that everything has healed, they may decide to send your child home for a short time. Your child will have these two catheters:
- a catheter in the Mitrofanoff
- a suprapubic catheter
The nurse will teach you how to look after your child’s catheters at home before you leave the hospital.
Before you go home, we will arrange for a home care nurse to visit you at home. This nurse will help you and your child look after the catheters in your home.
The doctor will decide when you should learn how to put a catheter into the Mitrofanoff to drain the urine. This is called catheterization. When you learn to catheterize the Mitrofanoff, your child will return to the hospital for a couple of hours. The nurse will teach you and your child how to do the catheterization.
Most young children who go to school can catheterize their Mitrofanoff on their own. Many children can help care for their own Mitrofanoff, even children who are not going to school yet.
Telling your child’s other doctors about the Mitrofanoff
Tell all doctors who take care of your child that they have a Mitrofanoff. Some doctors may not have heard of this before. You may have to explain it to them.
You should also tell the school nurse that your child has a Mitrofanoff.
Your child needs to wear a medic alert bracelet. Before your child leaves the hospital, the nurse will give you the forms to fill out to get this bracelet.
Mitrofanoff procedure risks
In general, the risks of the Mitrofanoff procedure include those of any surgery, such as infection, redness, swelling, bleeding, reactions to the anesthesia or failure of the operation. During surgery on the bladder, urine can also leak into other areas and cause some irritation.
Between 1 in 50 and 1 in 250 patients (your anaesthetist can estimate your individual risk): anesthetic or cardiovascular problems possibly requiring intensive care (including chest infection, pulmonary embolus, stroke, deep vein thrombosis, heart attack and death)
Mitrofanoff operations also carry several unique risks. Since the appendix is being partially detached and moved, there is a low risk of internal bleeding. It is possible that after a Mitrofanoff there may be problems catheterizing. Sometimes a different size catheter or more lubricant will solve the problem. The catheters put in place during surgery also make infections more likely than with other surgeries, but your child will receive a course of antibiotics during the recovery period to help avoid infections. The new hole in the belly may also leak. Finally, children who gain a lot of weight in the future may have problems catheterizing the opening.
The Mitrofanoff procedure has a high success rate. However, most children will eventually need another operation to adjust the appendix tube or fix problems, such as scarring that blocks the new opening to the belly. In many cases, these surgeries are minor and your child will not need an overnight stay at the hospital.
Mitrofanoff complications
The possible complications and your risk of getting them are shown below. Some are self-limiting or reversible, but others are not. We have not listed very rare after-effects (occurring in less than 1 in 250 patients) individually. The impact of these after-effects can vary a lot from patient to patient; you should ask your surgeon’s advice about the risks and their impact on you as an individual:
- Risk between 1 in 2 and 1 in 10 patients, the Mitrofanoff channel narrows requiring either a catheter to be left in for two weeks or further surgery to correct the problem.
- Risk 1 in 10 patients (10%), the Mitrofanoff channel leaks urine requiring further surgery to correct it.
- Risk between 1 in 10 and 1 in 50 patients, wound infection requiring antibiotics or drainage of any retained infection.
- Risk between 1 in 10 and 1 in 50 patients, late scarring and narrowing of the Mitrofanoff channel requiring further surgery to re-fashion it.
- Risk between 1 in 10 and 1 in 50 patients, leakage of bowel contents or urine from the stitch lines on your bowel and bladder requiring further surgery.
- Risk between 1 in 10 and 1 in 50 patients, significant bleeding requiring further surgery.
- Risk between 1 in 50 and 1 in 250 patients, the catheter in the Mitrofanoff channel falls out requiring a further procedure to replace it or re-fashion the channel.
What is my risk of a hospital-acquired infection?
Your risk of getting an infection in hospital is approximately 8 in 100 (8%); this includes getting MRSA or a Clostridium difficile bowel infection. This figure is higher if you are in a “high-risk” group of patients such as patients who have had:
- long-term drainage tubes (e.g. catheters);
- bladder removal;
- long hospital stays; or
- multiple hospital admissions.
References [ + ]





{kind=link}