
Contents
Ataxic cerebral palsy
Cerebral palsy (CP) is a group of disorders that affect a person’s ability to move and maintain balance and posture. People with ataxic cerebral palsy have problems with balance and coordination. They might be unsteady when they walk. They may walk with their legs farther apart than other kids. They might have a hard time with quick movements or movements that need a lot of control, like writing. They might have a hard time controlling their hands or arms when they reach for something. They can have trouble knowing exactly where something is. They might think it is closer or farther than it actually is.
Ataxic cerebral palsy is the least common form of cerebral palsy. Ataxia means ‘without order’ or ‘incoordination’. Ataxic movements are characterized by clumsiness, imprecision, or instability. Movements are not smooth and may appear disorganized or jerky. The incoordination seen with ataxia occurs when a person attempts to perform voluntary movements such as walking or picking up objects. Ataxia causes an interruption of muscle control in the arms and legs, resulting in a lack of balance and coordination.
Other types of cerebral palsy can lead to muscle stiffness (spastic cerebral palsy) or writhing movements (dyskinetic cerebral palsy). Some kids have more than one kind of cerebral palsy. Some people have symptoms of more than one type of cerebral palsy. The most common type of mixed cerebral palsy is spastic-dyskinetic cerebral palsy. And sometimes, the type of cerebral palsy a child has can change over time.
Figure 1. Human brain
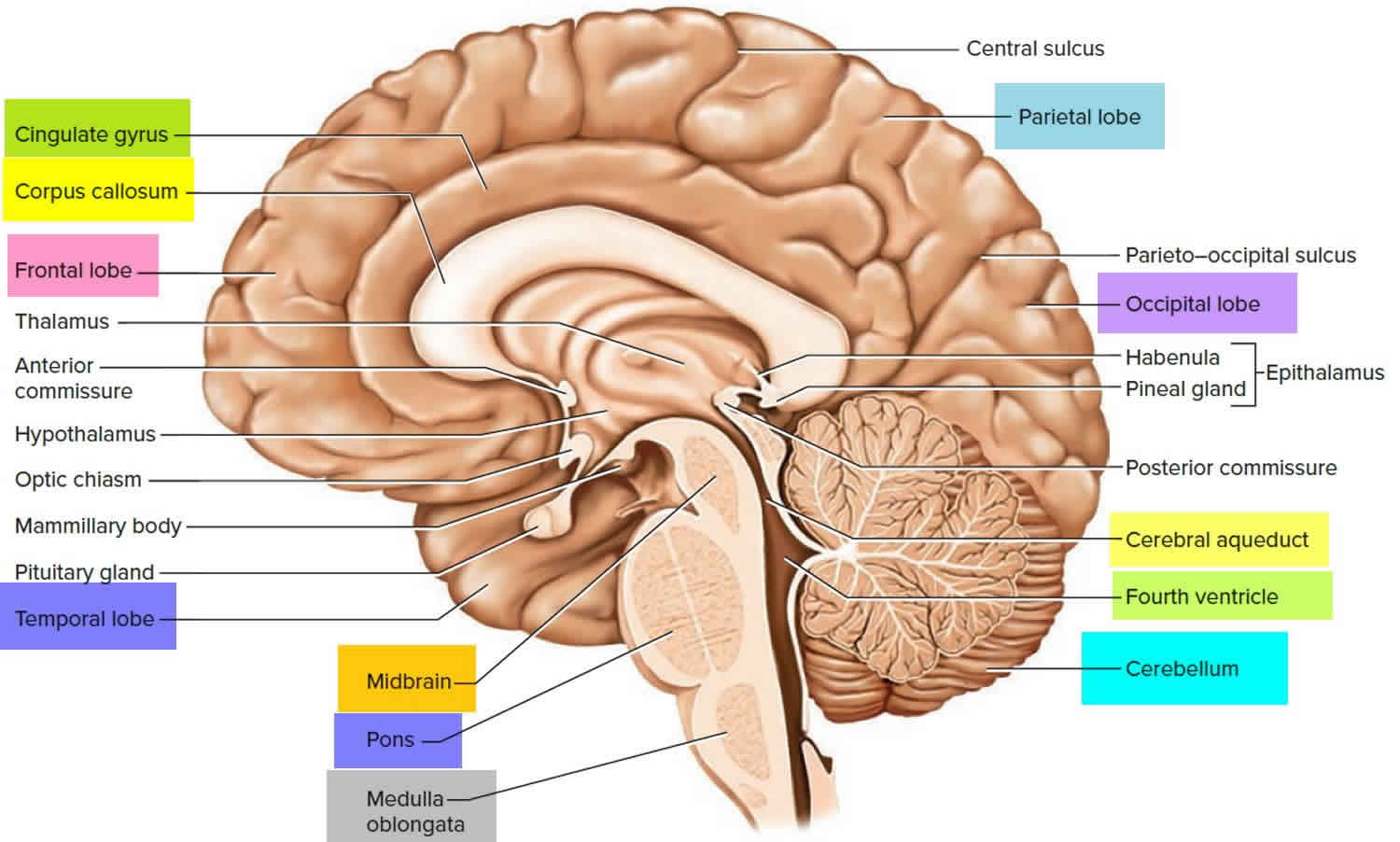
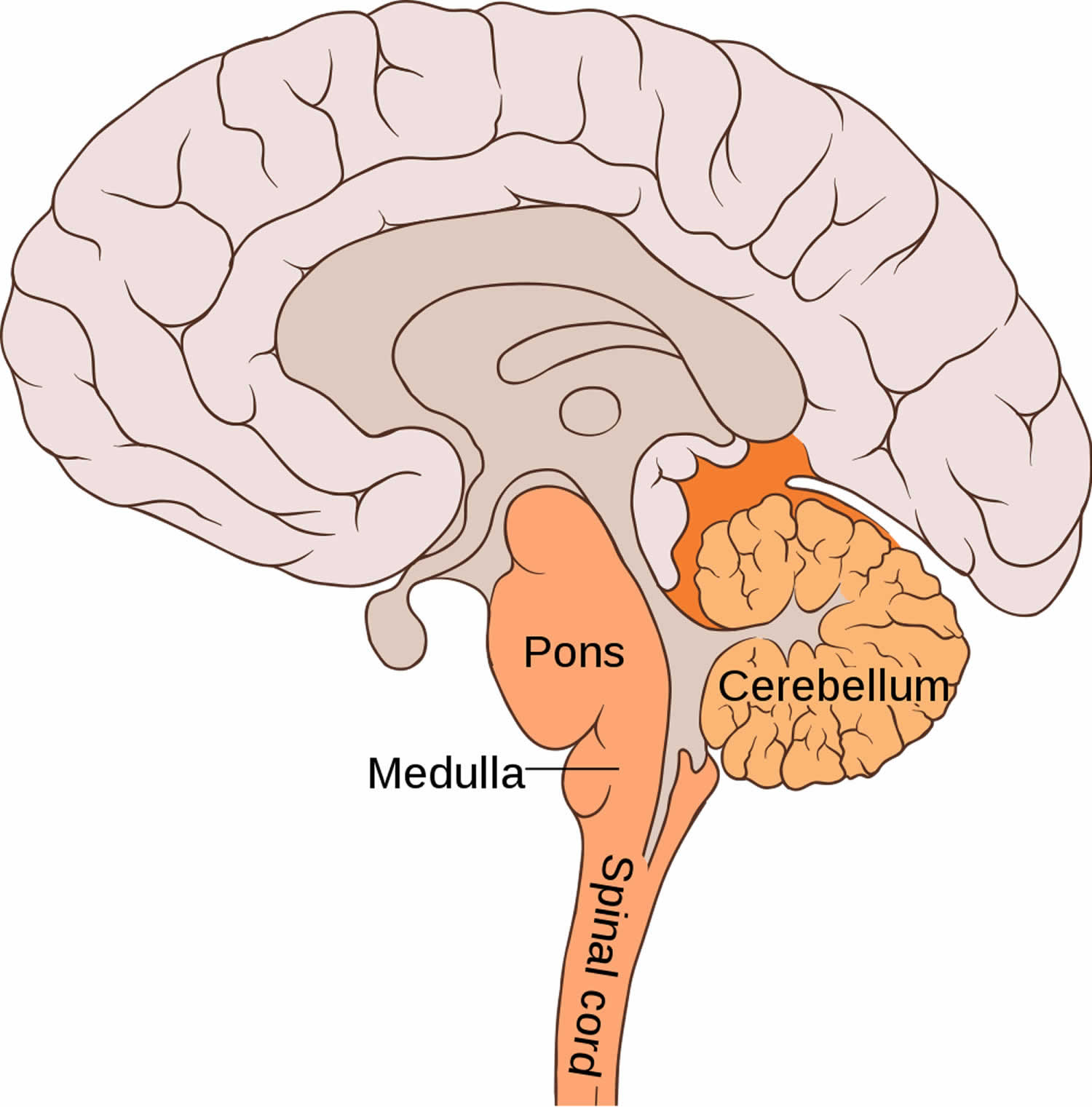
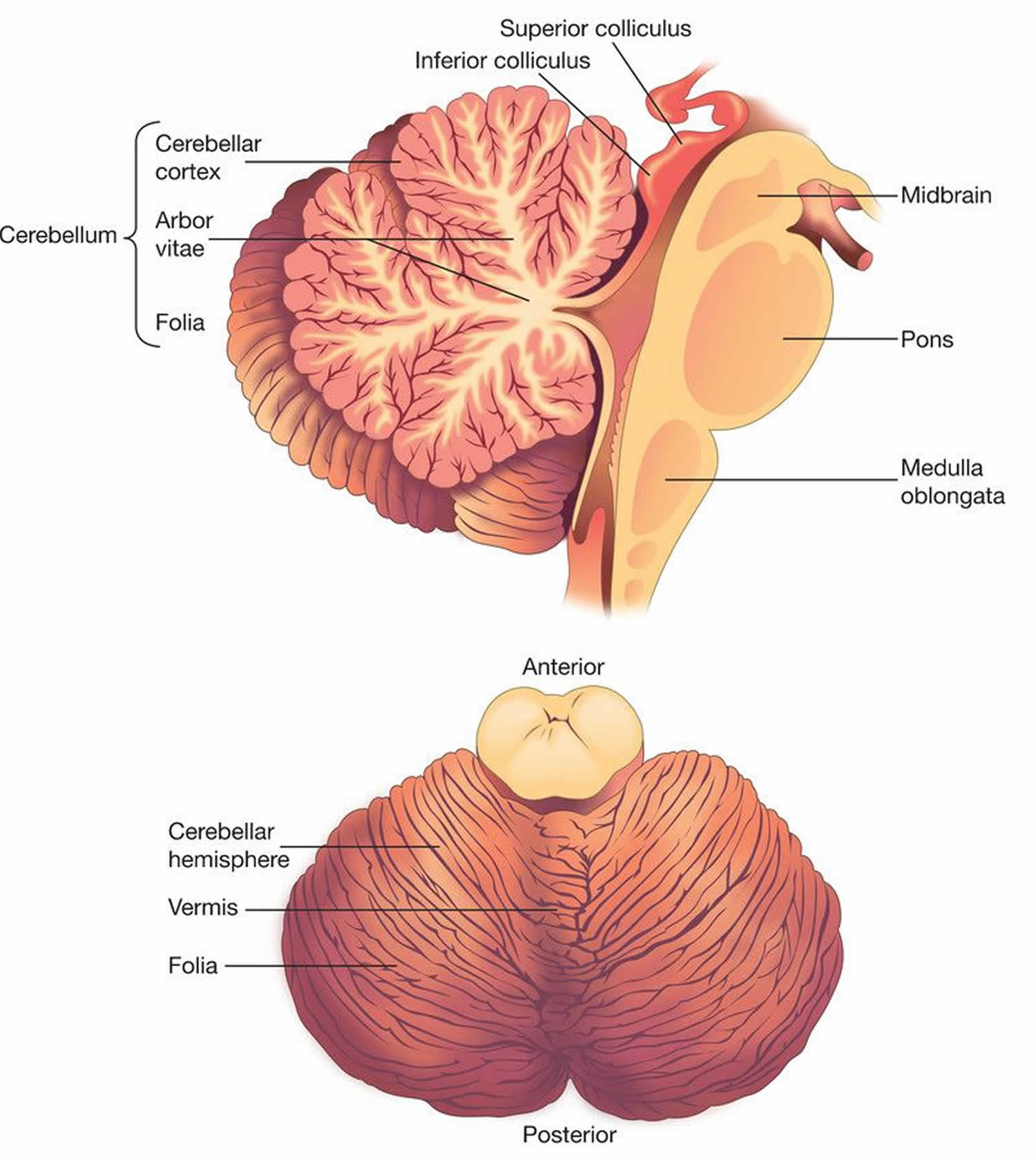
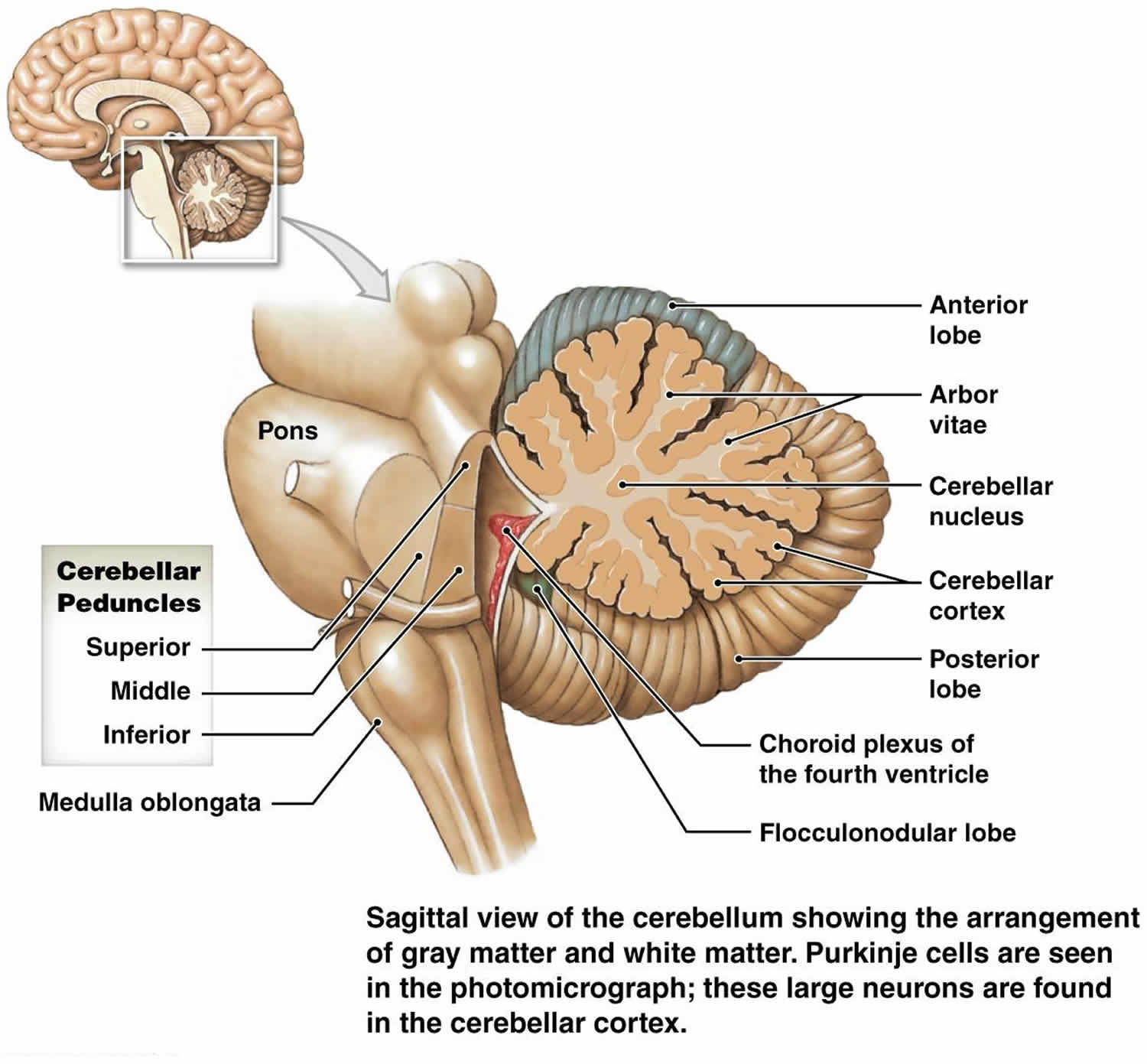
Figure 2. Cerebellum
Ataxic cerebral palsy causes
Cerebral palsy is usually the result of a brain injury or problem. In ataxic cerebral palsy, the brain injury or problem is in a part of the brain called the cerebellum. The cerebellum is the balance center of the brain. The cerebellum fine-tunes movement commands and coordinates movements in order to compensate for whatever posture is being used. The cerebellum also accounts for the various forces being generated by different parts of the body.
A child might be born with cerebral palsy or develop it later. The brain injury or problem doesn’t get worse, but someone with cerebral palsy may have different needs over time.
Cerebral palsy can be caused by:
- infections during pregnancy
- stroke either in the womb or after birth
- untreated jaundice (a yellowing of the skin and whites of eyes)
- genetic disorders
- medical problems in the mom during pregnancy
- being shaken as a baby (shaken baby syndrome)
- injury during delivery
- injury from an accident (such as a car accident)
Premature babies (babies born early) are at higher risk for cerebral palsy than babies born at full-term. So are low-birthweight babies (even if carried to term) and multiple births, such as twins and triplets.
Ataxic cerebral palsy symptoms
Ataxia means that someone has trouble coordinating muscles to do something. Ataxia can affect any part of the body and impact upon the movements required to do many day-to-day activities. Ataxia can affect a person’s legs, arms, hands, fingers, speech, eye movements and even muscles involved in swallowing. Kids with ataxic cerebral palsy may walk with their feet spread apart, and their walk may look unbalanced or jerky. They might not be able to get their muscles to do other things too, like reach for a fork.
People with ataxic cerebral palsy may have:
- Unsteady, shaky movements or tremor
- Difficulties maintaining balance
- People with ataxia appear very unsteady and shaky because their sense of balance and depth perception is affected.
Kids with all types of cerebral palsy can have vision, hearing, speech, eating, behavior, and learning problems. Some kids have seizures.
Effect on the upper limbs (arms and hands)
When ataxia affects the arms and hands it may cause a tremor or shakiness due to the over-correction of inaccurate movements – this means that when a person reaches for an object, they overshoot the target. It also results in difficulty performing tasks requiring precise finger movements such as handwriting or using cutlery, or movements that require regular repetition such as clapping.
Effect on the lower limbs (legs)
When ataxia affects walking, a person is unstable and likely to fall. As a result, the person usually walks with the feet spread further apart than the hips, which is known as a ‘wide-base gait’. This is done to try to compensate for their instability and poor balance. This way of walking can sometimes give the mistaken impression that the person is under the influence of alcohol or drugs. Because their balance is affected, the person may also fall without reason, or be unable to compensate for being accidentally bumped or for variations in the ground surfaces or an accidental mild bump from the side.
Effect on speech and swallowing
Ataxia may have an effect on speech and swallowing. When ataxia affects speech, it is sometimes called ‘scanning’ speech – the person uses a monotone voice with a breathy sound; sometimes there are unusual accelerations or pauses between their syllables.
Effect on the eyes
Ataxia may sometimes cause slow eye movements. When the person attempts to change their eye-gaze quickly, their eyes may miss the target. The eyes overshoot or underestimate their mark and then have to make ‘catch-up’ movements.
Ataxic cerebral palsy life diagnosis
Most children with ataxic cerebral palsy are diagnosed in the first 2 years of life. If a baby is premature or has another health problem that can be associated with cerebral palsy, this will alert health care providers to start looking for signs of cerebral palsy.
No single test can diagnose ataxic cerebral palsy. So health care professionals look at many things, including a child’s:
- development
- growth
- reflexes
- movement
- muscle tone
- interactions with others
Testing may include:
- brain MRI, CT scan, or ultrasound
- blood and urine (pee) tests to check for other medical conditions, including genetic conditions
- electroencephalography (EEG) to look at electrical activity in the brain
- electromyography (EMG) to check for muscle weakness
- evaluation of how a child walks and moves
- speech, hearing, and vision testing
Ataxic cerebral palsy life treatment
There is no cure for cerebral palsy. The health care team works with the child and family to make a treatment plan. The health care team includes a:
- pediatrician
- developmental behavioral pediatrician
- occupational therapist
- physical therapist
- speech therapist
- dietitian
- neurologist (nervous system doctor)
- ophthalmologist (eye doctor)
- orthopedic surgeon (bone doctor)
- otolaryngologist (ear, nose, and throat doctor)
The treatment plan may include:
- physical therapy and occupational therapy. Physical therapy and occupational therapy are among some of the main treatments for ataxic cerebral palsy. These treatments can help children with ataxic cerebral palsy become more independent later in life.
- leg braces, a walker, and/or a wheelchair
- medicine for muscle pain or stiffness
- special nutrition to help the child grow
- surgery to improve movement in the legs, ankles, feet, hips, wrists, and arms
Living with cerebral palsy is different for every child. To help your child move and learn as much as possible, work closely with your care team to develop a treatment plan. Then, as your child grows and his or her needs change, adjust the plan as necessary.
Physical therapy
Often the first step of treatment, physical therapy combines strength and flexibility exercises with massage therapy and orthotic devices, such as splints and casts. Orthotic devices are helpful when it comes to walking and posture by providing children with balance and stability.
The overall goal of physical therapy is to help children manage their movement problems and become more independent. In children with ataxic cerebral palsy, it may be difficult to balance or control reflexes. Physical therapists use various exercises when working with children who have this type of cerebral palsy to prevent muscles that are not used regularly from growing weak or shrinking.
Occupational therapy
Occupational therapy can help improve problems with balance or coordination in children with ataxic cerebral palsy while increasing their upper body strength. A main goal of occupational therapy is to provide a child with ataxic cerebral palsy with the skills they need to perform daily tasks on their own and decrease the use of assistive devices.
An occupational therapist will typically use various exercises to evaluate a child’s ability to perform daily tasks and age-appropriate activities. These exercises may also improve issues with strength, hand-eye coordination, sensory processing skills and playing with children their age.
Speech therapy
Children with ataxic cerebral palsy often struggle with expressing thoughts or emotions through speech, as well as having trouble swallowing. Speech therapy entails the use of articulation therapy, breathing exercises and word association to help a child with ataxic cerebral palsy to better communicate.
Speech-language pathologists (SLPs) will evaluate a child’s communication skills by conducting a series of auditory or listening training tests. Speech-language pathologists will also use language intervention activities that incorporates books, objects and pictures to stimulate language development. Swallowing and tongue exercises will allow children with conditions such as dysphagia to strengthen the muscles in their mouth and face.
Medication
Many children with ataxic cerebral palsy are prescribed medication as a supplement to physical therapy. Muscle relaxants and anti-anxiety medication, such as Valium, can calm shakiness and tremors.
Medications can also be used to treat co-occurring conditions, such as epilepsy, attention deficit hyperactivity disorder (ADHD) and incontinence. Physicians will typically evaluate the level of tremors a child with ataxic cerebral palsy experiences and prescribe medication based on the severity and frequency.
Ataxic cerebral palsy life expectancy
With appropriate therapeutic services, people with cerebral palsy may be able to fully integrate academically and socially.
Patients with severe forms of cerebral palsy may have a significantly reduced life span, although this continues to improve with improved health care and gastrostomy tubes 1). Patients with milder forms of this disorder have a life expectancy close to the general population, although it is still somewhat reduced 2).
The morbidity and mortality of cerebral palsy relate to the severity of this condition and concomitant medical complications, such as respiratory and gastrointestinal difficulties. In patients with quadriplegia, the likelihood of epilepsy, extrapyramidal abnormalities, and severe cognitive impairment is greater than in those with diplegia or hemiplegia.
Cognitive impairment occurs more frequently in persons with cerebral palsy than in the general population. The overall rate of mental retardation in affected persons is thought to be 30–50%. Some form of learning disability (including mental retardation) has been estimated to occur in perhaps 75% of patients. However, standardized cognitive testing primarily evaluates verbal skills and may result in the underestimation of cognitive abilities in some individuals.
In some studies, 25% of patients with cerebral palsy are unable to walk. However, many patients with this disorder (particularly those with spastic diplegia and spastic hemiplegia types) can ambulate independently or with assistive equipment. Thus, approximately 25% of children with cerebral palsy have mild involvement with minimal or no functional limitation in ambulation, self-care, and other activities. Approximately half are moderately impaired to the extent that complete independence is unlikely but function is satisfactory. Only 25% are so severely disabled that they require extensive care and are nonambulatory.
A prospective study of children has suggested that being able to sit by age 2 years is a good predictive sign of eventual ambulation. The suppression of obligatory primitive reflex activity by age 18–24 months was a sensitive indicator for distinguishing children who ultimately walked from those who were not expected to walk. Children who did not sit by age 4 years did not ambulate.
In patients with spastic quadriplegia, a less favorable prognosis correlated with a longer delay in the resolution of extensor tone. At times, hypertonicity and spasticity may improve or resolve over time in patients with cerebral palsy. Spasticity in patients with spastic quadriplegia can be more resistant even with services and orthopedic and rehabilitative intervention.
Complications
Cerebral palsy complications may affect multiple systems. For example, skin complications include decubitus ulcers and sores; orthopedic complications may include contractures, hip dislocation, and/or scoliosis.
Maintaining weight close to idea body weight is important for wheelchair-bound patients or those with ambulatory dysfunction. Nutrition consultation should be done early and periodically to ensure proper growth. Parents and medical professionals must keep on top of the potential nutritional difficulties in children with cerebral palsy. These patients are especially at risk of developing osteoporosis because of decreased weight bearing, so following their calcium intake and vitamin D levels is important 3).
Gastrointestinal and nutritional complications include the following:
- Failure to thrive due to feeding and swallowing difficulties secondary to poor oromotor control; patients may require a gastrostomy tube (G-tube) or a jejunostomy tube (J-tube) to augment nutrition.
- Obesity, less frequently than failure to thrive
- Gastroesophageal reflux and associated aspiration pneumonia
- Constipation
- Dental caries
Dental problems also include enamel dysgenesis, malocclusion, and gingival hyperplasia. Malocclusion is twice as prevalent as in the normal population. The increased incidence of dental problems is often secondary to the use of medications, especially drugs administered to premature infants and antiepileptic agents.
Respiratory complications include the following:
- Increased risk of aspiration pneumonia because of oromotor dysfunction
- Chronic lung disease/bronchopulmonary dysplasia
- Bronchiolitis/asthma
Neurologic complications include the following:
- Epilepsy
- Hearing loss (particularly in patients who had acute bilirubin encephalopathy (also known as kernicterus); also seen in patients who were born prematurely or who were exposed to ototoxic drugs)
- Vision
- Visual-field abnormalities due to cortical injury
- Strabismus
Epilepsy occurs in 15-60% of children with cerebral palsy and is more common in patients with spastic quadriplegia or mental retardation. When compared with controls, children with cerebral palsy have a higher incidence of epilepsy with onset within the first year of life and are more likely to have a history of neonatal seizures, status epilepticus, polytherapy, and treatment with second-line anticonvulsants. Factors associated with a seizure-free period of at least 1 year include normal intelligence, single seizure type, monotherapy, and spastic diplegia.
Visual acuity decreases in premature infants because of retinopathy of prematurity with hypervascularization and possible retinal detachment.
Cognitive/psychologic/behavioral complications include the following:
- Mental retardation (30-50%), most commonly associated with spastic quadriplegia
- Attention-deficit/hyperactivity disorder
- Learning disabilities
- Impact on academic performance and self-esteem
- Increased prevalence of depression
- Sensory integration difficulties
- Increased prevalence of pervasive developmental disorder or autism associated with concurrent diagnosis of cerebral palsy.
References [ + ]





{kind=link}