Contents
Sever’s disease
Sever’s disease also known as calcaneal apophysitis, is one of the most common causes of heel pain, particularly in growing children and adolescents between 9 and 12 years of age who are physically active. Sever’s disease is an inflammation of the growth plate in the calcaneus (heel). Sever’s disease usually develops around puberty. Boys are slightly more likely to have Sever’s disease than girls. Sever disease occurs more commonly in males, presenting most frequently at a median age of 12 years for males and 11 years for females. Symptoms can be unilateral, but up to 60% of cases can present with bilateral pain. The most commonly involved sports in these cases require repetitive running and jumping such as in basketball, soccer, track, cross-country, and gymnastics. Risk factors for Sever disease include general risk factors for overuse injury such as long or year-round activities, poorly fitting or worn-out footwear, or poor training mechanics. Additional biomechanical factors such as poor heel cord flexibility, pes cavus, pes planus, genu varum, or forefoot varus can predispose patients to the development of Sever’s disease 1).
Sever’s disease is caused by repetitive stress to the heel, and most often occurs during growth spurts, increased body weight, when bones, muscles, tendons, and other structures are changing rapidly. Children and adolescents who participate in athletics—especially running and jumping sports—are at an increased risk for Sever’s disease. However, less active adolescents may also experience Sever’s disease, especially if they wear very flat shoes.
The classic findings from a thorough history taking during the clinical evaluation will often include resolution of pain during periods of rest or inactivity 2). The clinical exam is notable for tenderness over calcaneal insertion of Achilles tendon and a positive squeeze test. Sever’s disease diagnosis is clinical and does not require imaging studies.
Sever’s disease is a self-limiting condition. This means that symptoms often ease with time. Sever’s disease management includes activity modification or relative rest as guided by pain. Symptoms may be managed with ice, anti-inflammatory medications, heel cups or heel lifts, and in severe cases, immobilization. A rehabilitation regimen focusing on heel cord stretching and strengthening should be included in the plan of care to both improve symptoms and correct predisposing underlying biomechanical factors. In most cases of Sever’s disease, simple measures like rest, over-the-counter medication, a change in footwear, and stretching and strengthening exercises will relieve pain and allow a return to daily activities.
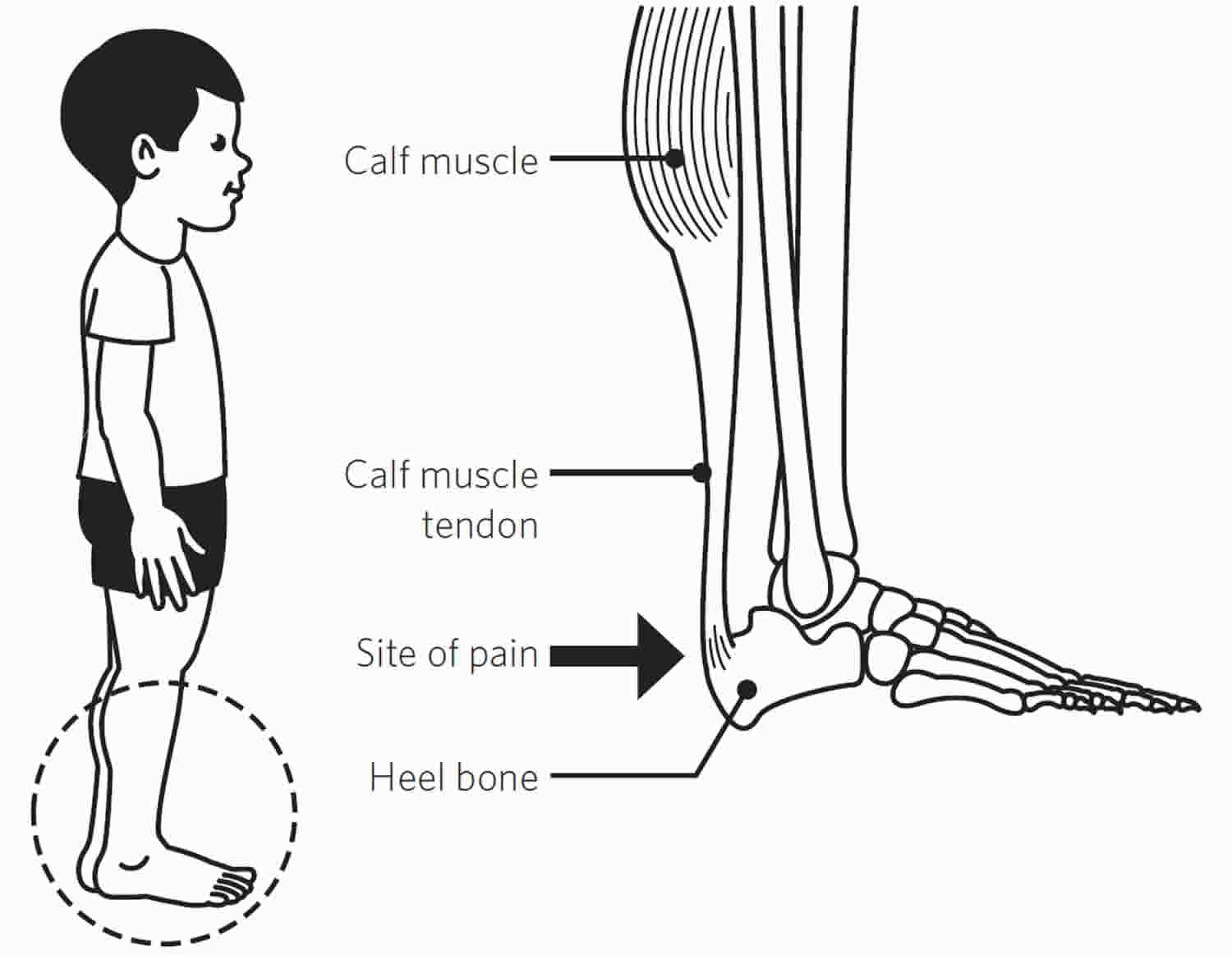
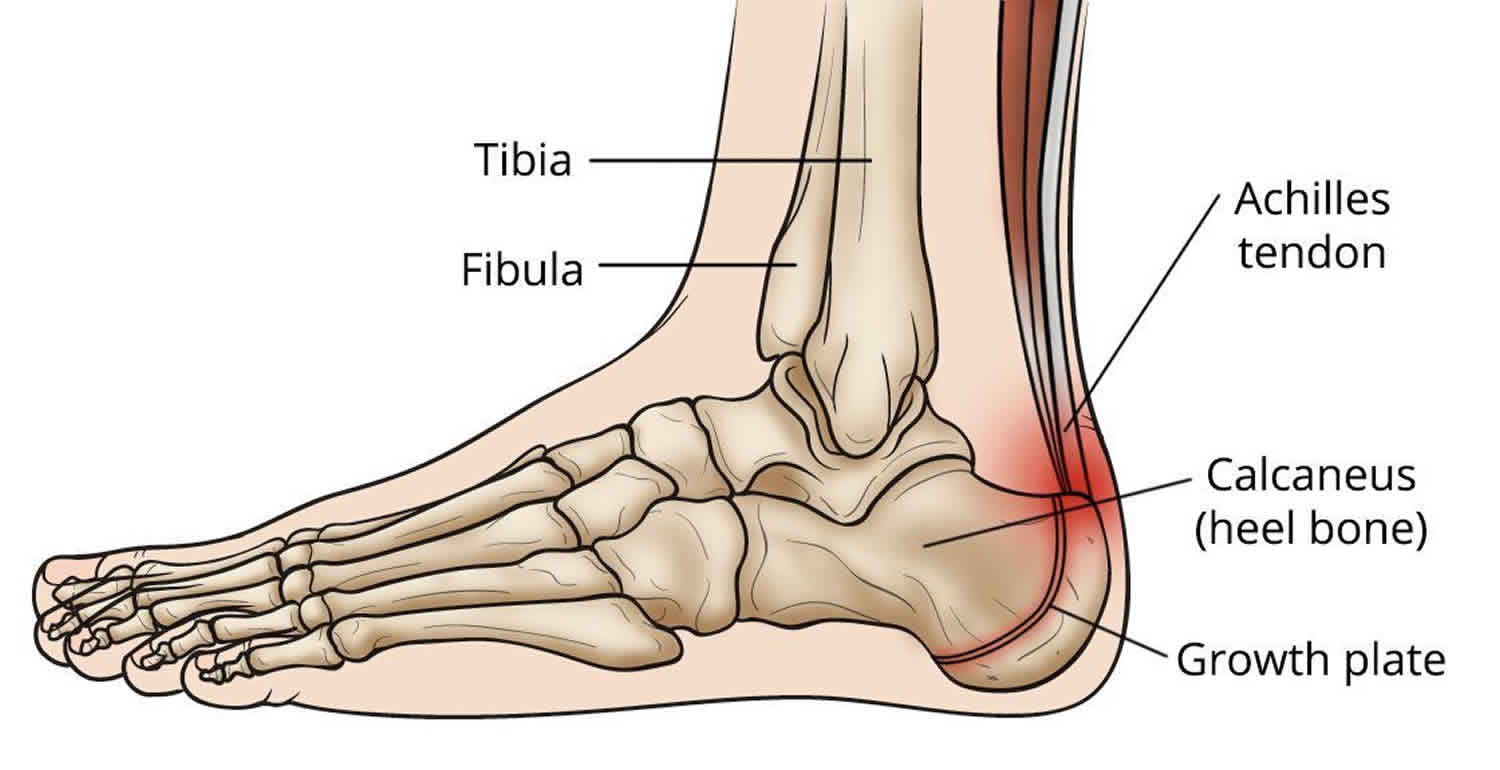
Figure 1. Sever’s disease
Sever’s disease cause
Sever’s disease is an overuse injury due to repetitive strain and microtrauma caused by the force of the strong Achilles tendon and resulting in irritation and potential partial avulsion of the relatively soft calcaneal apophysis. The force is increased after periods of rapid growth and increased activity. Rarely, trauma may lead to a full avulsion fracture. Contributing factors include increased or excessive sports activity (especially sports requiring repetitive running and jumping), heel cord tightness, weak ankle dorsiflexion, poorly cushioned or worn-out athletic shoes, and running on hard surfaces. Additional biomechanical factors contributing to poor shock absorption such as genu varum, forefoot varus, pes cavus, or pes planus can predispose one to Sever’s disease 3).
The bones of children and adolescents possess a special area where the bone is growing called the growth plate. Growth plates are areas of cartilage located near the ends of bones.
When a child is fully grown, the growth plates close and are replaced by solid bone. Until this occurs, the growth plates are weaker than the nearby tendons and ligaments and are vulnerable to trauma.
Sever’s disease affects the part of the growth plate at the back of the heel where bone growth occurs. This growth area serves as the attachment point for the Achilles tendon—the strong band of tissue that connects the calf muscles at the back of the leg to the heel bone.
Repetitive stress from running, jumping, and other high-impact activities can cause pain and inflammation in this growth area of the heel. Additional stress from the pulling of the Achilles tendon at its attachment point can sometimes further irritate the area.
Risk factors for developing Sever’s disease
Sever’s disease is age- and activity-related. It usually starts in pre-teens, and may be more common in pre-teens who are physically active. It occurs when the calcaneal (heel) apophysis is open and active.
Factors that may contribute to Sever’s disease in pre-teens include changes in:
- height and weight
- how much physical activity they are doing – this may be an increase in volume, intensity or frequency of activity. This commonly occurs:
- as one sports season ends and another starts
- where there is crossover in sport
- when a child starts to train and play for a team (the volume of activity increases with multiple weekly training sessions and a game)
- when they are involved in a sports carnival which involves playing multiple games in one day or over a number of days
- frequency of physical activity
- the type of physical activity – such as starting a different activity, or returning to a physical activity after a break. Sever’s disease is most commonly associated with sports and activities that are weight bearing, such as sports that involve running or jumping or both (for example, football, netball, running and gymnastics)
- equipment or external factors – such as changing to shoes with a low heel (for example, football boots or some types of running shoes; the lower heel adds extra load to the apophysis, because it places the Achilles tendon on increased stretch), doing a sport in bare feet, or even walking at the beach in thongs/flip flops.
Physical attributes that may contribute to developing Sever’s disease include:
- foot posture – active children who have a flat foot posture may be slightly more predisposed to Sever’s disease
- increased body weight, or
- a high BMI (body mass index).
Sever’s disease pathophysiology
The posterior calcaneus develops as a secondary ossification center that provides attachment for the Achilles tendon. During the early adolescent growth spurt, bone growth exceeds the ability of the muscle-tendon unit to stretch sufficiently to maintain previous flexibility which in turns leads to increased tension across the unossified or incompletely ossified apophysis. The apophysis is the weakest point in the muscle-tendon-bone-attachment (as opposed to the tendon in an adult), and therefore it is at risk for overuse injury from repetitive stress. Excessive and repetitive traction from the strong Achilles tendon results in microtrauma and chronic irritation causing thickening and pain at the apophysis 4).
Sever’s disease prevention
Preventative measures include general counseling to avoid overuse injuries. Patients should be encouraged to maintain adequate hydration, diet, and sleep and avoid increasing activity level > 10% per week.
Ensure the use of proper equipment and techniques, encourage stretching to maintain flexibility, and consider recommending against early single sport specialization.
The decision to avoid or limit activity should be shared between provider, patient, and parent and include a discussion of short term and long term goals and primarily be driven by the degree of pain.
As patients generally are very active in multiple arenas (multiple sports or multiple teams in same sport) in the same season, consider eliminating one team/sport as opposed to complete cessation of activity which can be difficult to achieve patient buy-in 5).
Sever’s disease symptoms
A few signs and symptoms point to Sever’s disease, which may affect one or both heels, although one heel may be worse than the other. Symptoms may include:
- heel pain during physical exercise and other sports-related activities, especially activities that require running or jumping
- heel pain and tenderness underneath the heel
- worsening of pain after exercise
- mild swelling at the heel
- limping – often in the morning, or during or after sport
- a tendency to tiptoe (Sever sign).
Typical presentation includes an active adolescent with unilateral or bilateral heel pain that is worse during and after activity, especially running and jumping, and often in the setting of a recent growth spurt or starting a new sport/training. There is usually no preceding trauma. Pain improves with rest and typically is absent in the morning. Over time, the pain may progress in severity enough to limit activity. The physical exam should be negative for erythema or ecchymosis, but tenderness and mild swelling may be present at the Achilles insertion on the heel. The exam may also reveal pain with passive ankle dorsiflexion. Pain is reproduced with compression of the posterior calcaneus (squeeze test) and aggravated by standing on tiptoes (Sever sign). Poor heel cord flexibility or weakness with dorsiflexion may be present as predisposing factors 6).
Sever’s disease diagnosis
Sever’s disease is a clinical diagnosis, and imaging is usually not necessary. A doctor can diagnose Sever’s disease by asking the young person to describe their symptoms and by conducting a physical examination. If the presentation is atypical, severe, or persistent, medical imaging may be required to evaluate and rule out infection, neoplasm, or occult fracture. Plain radiographs may show fragmentation, sclerosis, or increased density of the calcaneal apophysis.; however, these changes also can be seen in normal variants. If ordering radiographs, consider bilateral imaging to delineate osseous abnormality versus normal variants in the individual patient 7).
When an apophysis is active it is changing from cartilage to bone. During this phase, the normal x-ray appearance will vary from no bony tissue to small deposits of bone to a fully united bony tendon attachment.
However, there is usually no difference in what can be seen in a heel x-ray of a child experiencing Sever’s disease-related pain, and that of another child of the same age who is pain free. For this reason, x-rays are generally not used to diagnose Sever’s disease.
Sever’s disease differential diagnosis
Causes of heel pain in pre-teens, other than Sever’s disease, include:
- bursitis – bursae are small sacs that contain fluid to lubricate moving parts such as joints and muscles. Common causes of bursitis at the back of the heel include injury, overuse and tight shoes
- posterior ankle impingement (not common in this age group) – can occur after an ankle sprain and in activities such as dance, gymnastics and football where participants spend a lot of time on their toes
- stress fracture (not common in this age group) – can result when loading on the bone leads to weakening of the bone
- heel fracture – can occur with a fall from a height directly onto the heel
- juvenile rheumatoid arthritis – causes persistent joint pain, swelling and stiffness
- tumor – this is a less common cause of heel pain, but is important to consider and rule out.
Sever’s disease treatment
No one treatment method has been proven to be better than others in the long-term management of pain from Sever’s disease. Sever’s disease is a self-limiting condition (will get better on its own) and treatment depends on the how much pain is present.
Treatment for Sever’s disease focuses on reducing pain and swelling. This typically requires limiting exercise activity until your child can enjoy activity without discomfort or significant pain afterwards. In some cases, rest from activity is required for several months, followed by a strength conditioning program. However, if your child does not have a large amount of pain or a limp, participation in sports may be safe to continue.
Your doctor may recommend additional treatment methods, including:
- Heel pads. Heel cushions inserted in sports shoes can help absorb impact and relieve stress on the heel and ankle.
- Wearing shoes with a slightly elevated heel. Elevating the heel may relieve some of the pressure on the growth plate.
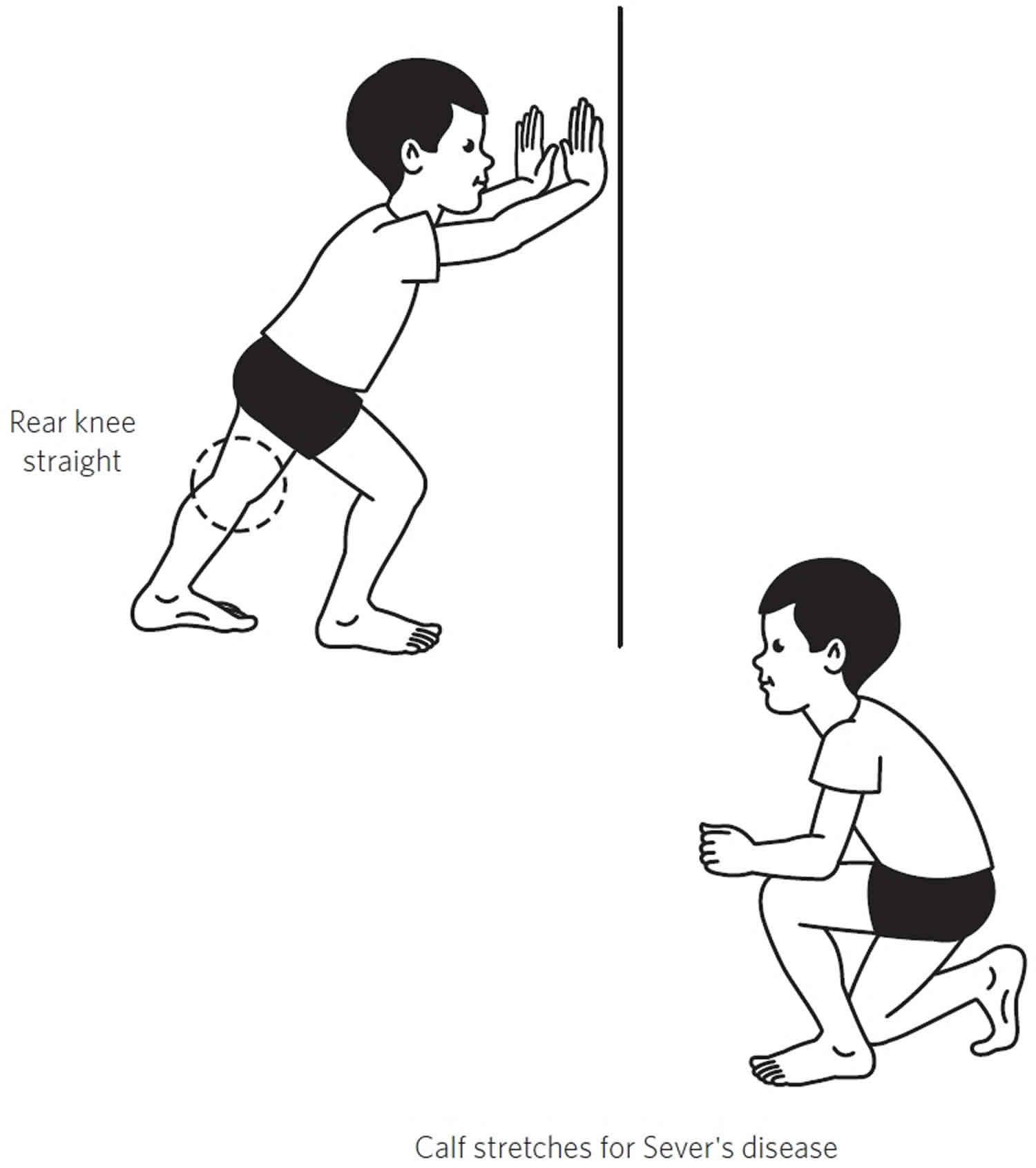
- Stretching exercises. Stretches for the Achilles tendon can reduce stress on the heel, help relieve pain, and hopefully prevent the disease from returning.
- Nonsteroidal anti-inflammatory medication. Drugs like ibuprofen and naproxen can help reduce pain and swelling.
In cases where the pain is bad enough to interfere with walking, a “walker boot” might be required to immobilize the foot while it heals.
A rehabilitation regimen is essential and should include heel cord stretching in addition to dorsiflexor strengthening. If the pain does not respond to conservative measures, a walking boot or short leg cast may be used for short-term immobilization. Symptoms are usually self-limited with improvement within 6 to 12 months and a complete resolution with apophyseal closure. There is no role for injection therapy or surgical intervention in the treatment of Sever disease. There are no long-term complications, and the prognosis is excellent 8).
Figure 2. Sever’s disease stretching exercises
Sever’s disease prognosis
It is not unusual for Sever’s disease to recur. This typically happens when a child once again increases sports activities. Wearing sports shoes that provide good support to the foot and heel may help prevent recurrence.
Sever’s disease will not return once a child is fully grown and the growth plate in the heel has matured into solid bone.
References [ + ]





{kind=link}