
Contents
Signs of labor
Labor also called childbirth, is the process of your baby leaving the uterus (womb).
Labor is divided into three stages:
- Labor
- Pushing and birth
- Delivery of the placenta
Every woman’s labor is different. And your labor may be different each time you have a baby. But there are patterns to labor that are true for most women. Learning about the stages of labor and what happens during each one can help you know what to expect once labor begins.
You’re in labor when you have regular contractions that cause your cervix to change. Contractions are when the muscles of your uterus get tight and then relax. Contractions help push your baby out of your uterus. Your cervix is the opening to the uterus that sits at the top of the vagina. When labor starts, your cervix dilates (opens up).
As you get closer to your due date, learning the signs of labor can help you feel ready for labor and birth. If you have any signs of labor, call your doctor.
As you approach your due date, you will be looking for any little sign that labor is about to start. You might notice that your baby has “dropped” or moved lower into your pelvis. This is called “lightening.” If you have a pelvic exam during your prenatal visit, your doctor might report changes in your cervix that you cannot feel, but that suggest your body is getting ready. For some women, a flurry of energy and the impulse to cook or clean, called “nesting,” is a sign that labor is approaching.
Some signs suggest that labor will begin very soon. Call your doctor or midwife if you have any of the following signs of labor. Call your doctor even if it’s weeks before your due date — you might be going into preterm labor. Your doctor or midwife can decide if it’s time to go to the hospital or if you should be seen at the office first.
You know you’re in true labor when:
- You have strong and regular contractions. A contraction is when the muscles of your uterus tighten up like a fist and then relax. Contractions help push your baby out. When you’re in true labor, your contractions last about 30 to 70 seconds and come about 5 to 10 minutes apart. They’re so strong that you can’t walk or talk during them. You have contractions get stronger and closer together over time with increasingly shorter intervals.
- You feel pain in your belly and lower back (backache). This pain doesn’t go away when you move or change positions.
- You have a bloody (brownish or reddish) mucus discharge. This is called bloody show, when the plug of mucus from your cervix (entrance to your womb, or uterus) comes away. Losing your mucus plug usually means your cervix is dilating (opening up) and becoming thinner and softer (effacing). Labor could start right away or may still be days away.
- Your water breaks (rupture of membranes). Your baby has been growing in amniotic fluid (the bag of waters) in your uterus. When the bag of waters breaks, you may feel a big rush of water. Or you may feel just a trickle.
- You have an urge to go to the toilet, which is caused by your baby’s head pressing on your bowel
If you think you’re in labor, call your doctor, no matter what time of day or night. Your doctor can tell you if it’s time to head for the hospital. To see for sure that you’re in labor, your health care provider measures your cervix.
Remember, no one knows for sure what triggers labor, and every woman’s experience is unique. Sometimes it’s hard to tell when labor begins.
Don’t hesitate to call your health care provider if you’re confused about whether you’re in labor. Preterm labor can be especially sneaky. If you have any signs of labor before 37 weeks — especially if you also experience vaginal spotting — consult your health care provider.
If you arrive at the hospital in false labor, don’t feel embarrassed or frustrated. Think of it as a practice run. The real thing is likely on its way.
Did my water break?
It’s not always easy to know. If your water breaks, it could be a gush or a slow trickle of amniotic fluid. Rupture of membranes is the medical term for your water breaking. Let your doctor know the time your water breaks and any color or odor. Also, call your doctor if you think your water broke, but are not sure. An easy test can tell your doctor if the leaking fluid is urine (many pregnant women leak urine) or amniotic fluid. Often a woman will go into labor soon after her water breaks. When this doesn’t happen, her doctor may want to induce (bring about) labor. This is because once your water breaks, your risk of getting an infection goes up as labor is delayed.
What are early signs of labor?
You may be close to starting labor if:
- Your baby drops or moves lower into your pelvis. This is called lightening. It means that your baby is getting ready to move into position for birth. It can happen a few weeks or even just a few hours before your labor begins.
- You have an increase in vaginal discharge that’s clear, pink or slightly bloody. This is called show or bloody show. It can happen a few days before labor starts or at the beginning of labor.
- At a prenatal checkup, your health care provider tells you that your cervix has begun to efface (thin) and dilate (open). Before labor, your cervix is about 3.5 to 4 centimeters long. When it’s fully dilated (open) for labor, it’s 10 centimeters. Once labor starts, contractions help open your cervix.
- You have the nesting instinct. This is when you want to get things organized in your home to get ready for your baby. You may want to do things like cook meals or get the baby’s clothes and room ready. Doing these things is fine as long as you’re careful not to overdo it. You need your energy for labor and birth.
If you have any of these signs, you may start labor soon. Learn the signs of labor so you know when to call your doctor.
Thinning of the cervix (effacement)
Before labor, the lower part of your uterus called the cervix is typically 3.5 cm to 4 cm long. As labor begins, your cervix softens, shortens and thins (effacement). You might feel uncomfortable, but irregular, not very painful contractions or nothing at all.
Effacement is often expressed in percentages. At 0 percent effacement, the cervix is at least 2 centimeters (cm) long, or very thick. Your cervix must be 100 percent effaced, or completely thinned out, before a vaginal delivery.
Opening of the cervix (dilation)
Another sign of labor is your cervix beginning to open (dilate). Your health care provider will measure the dilation in centimeters from zero (no dilation) to 10 (fully dilated).
At first, these cervical changes can be very slow. Once you’re in active labor, expect to dilate more quickly.
Increase in vaginal discharge
During pregnancy, a thick plug of mucus blocks the cervical opening to prevent bacteria from entering the uterus. During the late third trimester, this plug might be pushed into your vagina. You might notice an increase in vaginal discharge that’s clear, pink or slightly bloody. This might happen several days before labor begins or at the start of labor.
If vaginal bleeding is as heavy as a normal menstrual period, however, contact your health care provider immediately. Heavy vaginal bleeding could be a sign of a problem.
Nesting or spurt of energy
You might wake up one morning feeling energetic, eager to fill the freezer with prepared meals, set up the crib and arrange your baby’s outfits according to color. This urge is commonly known as the nesting instinct.
Nesting can begin at any time during pregnancy but for some women it’s a sign that labor is approaching. Do what you must, but don’t wear yourself out. Save your energy for the harder work of labor ahead.
Feeling the baby has dropped lower
Lightening is the term used to describe when the baby’s head settles deep into your pelvis. This might cause a change in the shape of your abdomen. This change can happen anywhere from a few weeks to a few hours before labor begins.
Your water breaks (rupture of membranes)
The amniotic sac is a fluid-filled membrane that cushions your baby in the uterus. At the beginning of or during labor, your membranes will rupture also known as your water breaking.
When your water breaks you might experience an irregular or continuous trickle of small amounts of watery fluid from your vagina or a more obvious gush of fluid. If your water breaks — or if you’re uncertain whether the fluid is amniotic fluid, urine or something else — consult your health care provider or head to your delivery facility right away. You and your baby will be evaluated to determine the next steps.
Once your amniotic sac is no longer intact, timing becomes important. The longer it takes for labor to start after your water breaks — if it hasn’t started already — the greater you or your baby’s risk of developing an infection. Your health care provider might stimulate uterine contractions before labor begins on its own (labor induction).
Contractions when labor pains begin
During the last few months of pregnancy, you might experience occasional, sometimes painful, contractions — a sensation that your uterus is tightening and relaxing. These are called Braxton Hicks contractions.
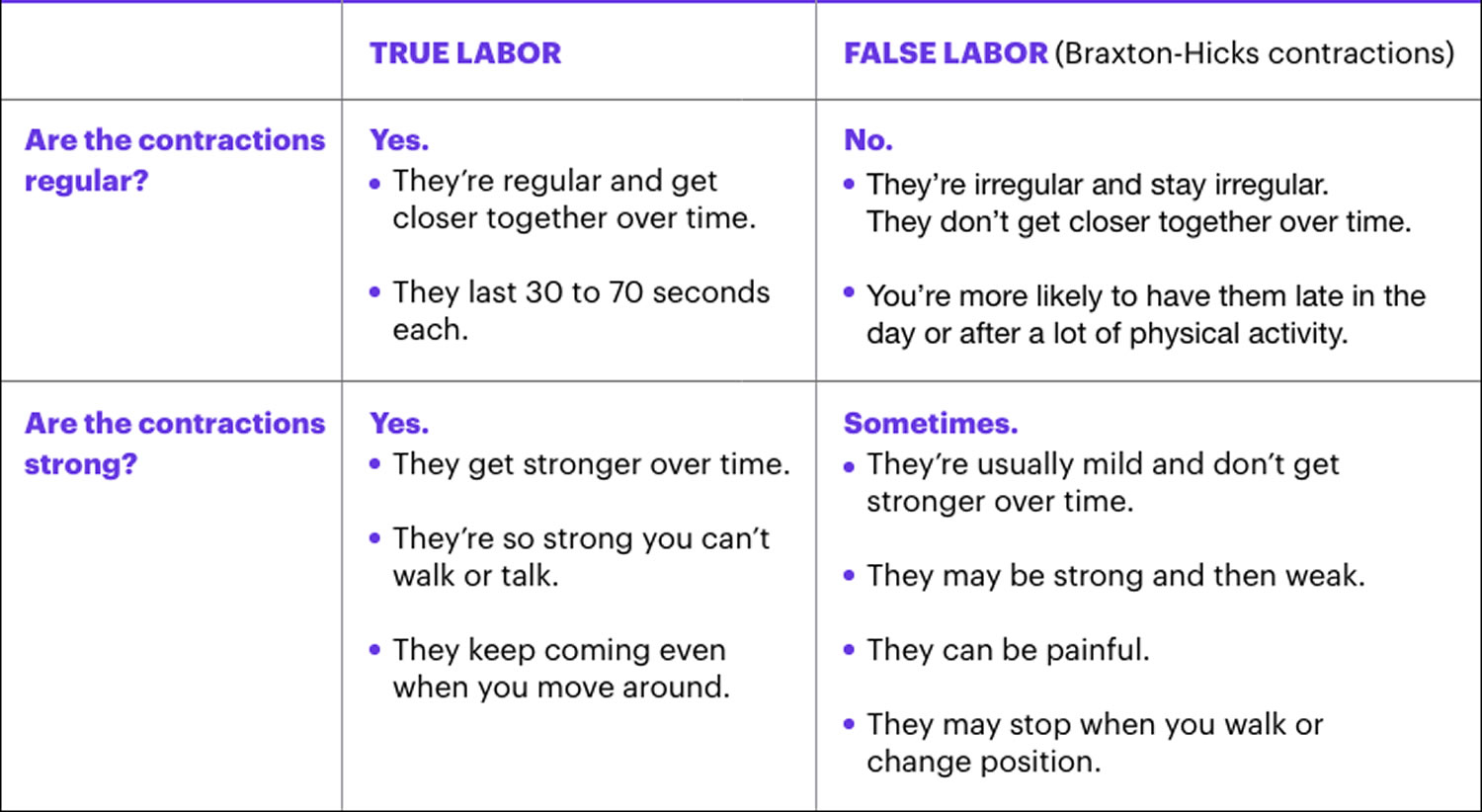
To tell the difference between Braxton Hicks contractions and the real thing, consider these questions:
- Are the contractions regular? Time your contractions from the beginning of one to the beginning of the next. Look for a regular pattern of contractions that get progressively stronger and closer together. False labor contractions will remain irregular.
- How long do they last? Time how long each contraction lasts. True contractions last about 30 to 70 seconds.
- Do the contractions stop? True contractions continue regardless of your activity level or position. With false labor, the contractions might stop when you walk, rest or change position.
What are false labor and Braxton-Hicks contractions?
Not all contractions mean you’re in labor. You may have contractions on and off before true labor starts. These contractions are called false labor or Braxton-Hicks contractions. They soften and thin the cervix to help your body get ready for labor and birth. You may feel them in the weeks right before your due date. Learning the differences between true labor contractions and false labor contractions can help you know when you’re really in labor.
It can be hard to tell the difference between true labor and false labor. When you first feel contractions, time them. Write down how much time it takes from the start of one contraction to the start of the next. Make a note of how strong the contractions feel. Keep a record of your contractions for 1 hour. Walk or move around to see if the contractions stop when you change positions.
Table 1. True labor versus false labor (Braxton-Hicks contractions)
What are stages of labor?
Stages of labor include the whole process of labor, from your first contractions (stage 1) to pushing (stage 2) to delivery of the placenta (stage 3) after your baby is born. When regular contractions begin, the baby moves down into the pelvis as the cervix both effaces (thins) and dilates (opens). How labor progresses and how long it lasts are different for every woman. But each stage features some milestones that are true for every woman.
Learning about the stages of labor can help you know what to expect during labor and birth.
What happens in the first stage of labor?
The first stage of labor is the longest stage. The first stage is divided into three parts: early labor, active labor and transition to stage 2 of labor. For first-time moms, it can last from 12 to 19 hours . It may be shorter (about 14 hours) for moms who’ve already had children. It’s when contractions become strong and regular enough to cause your cervix to dilate (open) and thin out (efface). This lets your baby move lower into your pelvis and into your birth canal (vagina). This stage of labor ends when you are 10 centimeters dilated.
The first stage begins with the onset of labor and ends when the cervix is fully opened. It is the longest stage of labor, usually lasting about 12 to 19 hours. Many women spend the early part of this first stage at home. You might want to rest, watch TV, hang out with family, or even go for a walk. Most women can drink and eat during labor, which can provide needed energy later. Yet some doctors advise laboring women to avoid solid food as a precaution should a cesarean delivery be needed. Ask your doctor about eating during labor. While at home, time your contractions and keep your doctor up to date on your progress. Your doctor will tell you when to go to the hospital or birthing center.
At the hospital, your doctor will monitor the progress of your labor by periodically checking your cervix, as well as the baby’s position and station (location in the birth canal). Most babies’ heads enter the pelvis facing to one side, and then rotate to face down. Sometimes, a baby will be facing up, towards the mother’s abdomen. Intense back labor often goes along with this position. Your doctor might try to rotate the baby, or the baby might turn on its own.
As you near the end of the first stage of labor, contractions become longer, stronger, and closer together. Many of the positioning and relaxation tips you learned in childbirth class can help now. Try to find the most comfortable position during contractions and to let your muscles go limp between contractions. Let your support person know how he or she can be helpful, such as by rubbing your lower back, giving you ice chips to suck, or putting a cold washcloth on your forehead.
Sometimes, medicines and other methods are used to help speed up labor that is progressing slowly. Many doctors will rupture the membranes. Although this practice is widely used, studies show that doing so during labor does not help shorten the length of labor.
Your doctor might want to use an electronic fetal monitor to see if blood supply to your baby is okay. For most women, this involves putting two straps around the mother’s abdomen. One strap measures the strength and frequency of your contractions. The other strap records how the baby’s heartbeat reacts to the contraction.
The most difficult phase of this first stage is the transition. Contractions are very powerful, with very little time to relax in between, as the cervix stretches the last, few centimeters. Many women feel shaky or nauseated. The cervix is fully dilated when it reaches 10 centimeters.
Figure 1. First stage of labor
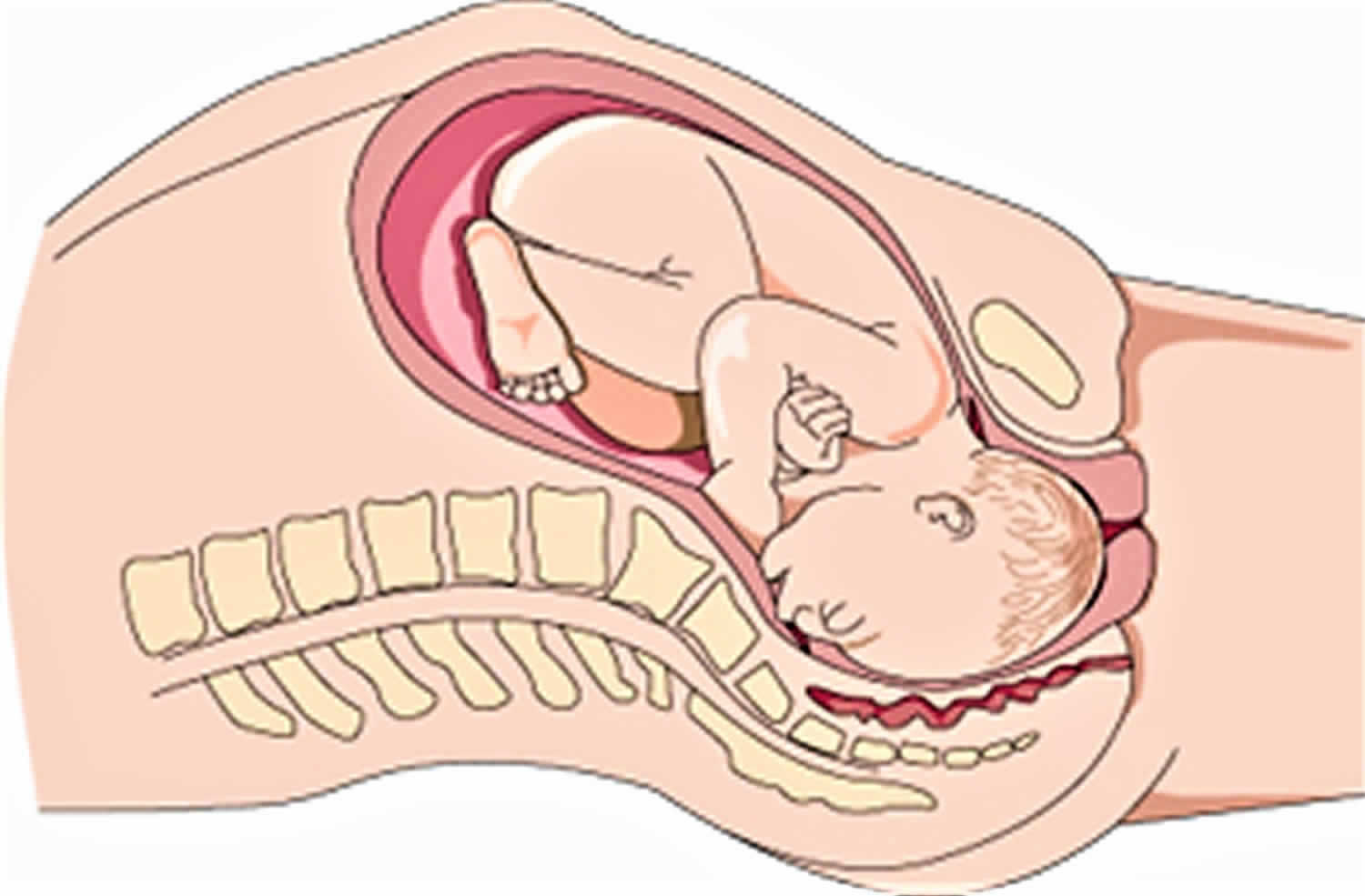
Footnote: Most babies’ heads enter the pelvis facing to one side, and then rotate to face down.
Early labor
For most first-time moms, early labor lasts about 6 to 12 hours. You can spend this time at home or wherever you’re most comfortable. During early labor:
- You may feel mild contractions that come every 5 to 15 minutes and last 60 to 90 seconds.
- You may have a bloody show. This is a pink, red or bloody vaginal discharge. If you have heavy bleeding or bleeding like your period, call your doctor right away.
What you can do in early labor:
This is a great time for you to rely on your doula or labor support person. Try the methods you learned about in childbirth education classes about how to relax and cope with pain. During early labor:
- Rest and relax as much as you can.
- Take a shower or bath.
- Go for a walk.
- Change positions often.
- Make sure you’re ready to go to the hospital.
- Take slow, relaxing breaths during contractions.
Active labor
This is when you head to the hospital! Active labor usually lasts about 4 to 8 hours. It starts when your contractions are regular and your cervix has dilated to 6 centimeters. In active labor:
- Your contractions get stronger, longer and more painful. Each lasts about 45 seconds and they can be as close as 3 minutes apart.
- You may feel pressure in your lower back, and your legs may cramp.
- You may feel the urge to push.
- Your cervix will dilate up to 10 centimeters.
- If your water hasn’t broken, it may break now.
- You may feel sick to your stomach.
What you can do in active labor:
- Make sure the hospital staff has a copy of your birth plan.
- Try to stay relaxed and not think too hard about the next contraction.
- Move around or change positions. Walk the hallways in the hospital.
- Drink water or other liquids. But don’t eat solid foods.
- If you’re going to take medicine to help relieve labor pain, you can start taking it now. Your choice about pain relief is part of your birth plan.
- Go to the bathroom often to empty your bladder. An empty bladder gives more room for your baby’s head to move down.
- If you feel like you want to push, tell your doctor. You don’t want to start pushing until your doctor checks your cervix to see how dilated it is.
Transition to the second stage of labor
This can be the toughest and most painful part of labor. It can last 15 minutes to an hour. During the transition:
- Contractions come closer together and can last 60 to 90 seconds. You may feel like you want to bear down.
- You may feel a lot of pressure in your lower back and rectum. If you feel like you want to push, tell your doctor.
What happens in the second stage of labor?
In the second stage of labor, your cervix is fully dilated and ready for childbirth. It usually lasts 20 minutes to two hours. The second stage is the most work for you because your doctor wants you to start pushing your baby out. This stage can be as short as 20 minutes or as long as a few hours. It may be longer for first-time moms or if you’ve had an epidural. And epidural is pain medicine you get through a tube in your lower back that helps numb your lower body during labor. It’s the most common kind of pain relief used during labor. The second stage ends when your baby is born.
The second stage involves pushing and delivery of your baby. You will push hard during contractions, and rest between contractions. Pushing is hard work, and a support person can really help keep you focused. A woman can give birth in many positions, such as squatting, sitting, kneeling, or lying back. Giving birth in an upright position, such as squatting, appears to have some benefits, including shortening this stage of labor and helping to keep the tissue near the birth canal intact. You might find pushing to be easier or more comfortable one way, and you should be allowed to choose the birth position that feels best to you.
When the top of your baby’s head fully appears (crowning), your doctor will tell you when to push and deliver your baby. Your doctor may make a small cut, called an episiotomy, to enlarge the vaginal opening. Most women in childbirth do not need episiotomy. Sometimes, forceps (tool shaped like salad-tongs) or suction is used to help guide the baby through the birth canal. This is called assisted vaginal delivery. After your baby is born, the umbilical cord is cut. Make sure to tell your doctor if you or your partner would like to cut the umbilical cord.
During the second stage of labor:
- Your contractions may slow down to come every 2 to 5 minutes apart. They last about 60 to 90 seconds.
- You may get an episiotomy. This is a small cut made at the opening of the vagina to help let the baby out. Most women don’t need an episiotomy.
- Your baby’s head begins to show. This is called crowning.
- Your doctor guides your baby out of the birth canal. She may use special tools, like forceps or suction, to help your baby out.
- Your baby is born, and the umbilical cord is cut. Instructions about who’s cutting the umbilical cord are in your birth plan. What you can do:
- Find a position that is comfortable for you. You can squat, sit, kneel or lie back.
- Push during contractions and rest between them. Push when you feel the urge or when your doctor tells you.
- If you’re uncomfortable or pushing has stopped, try a new position.
Figure 2. Second stage labor
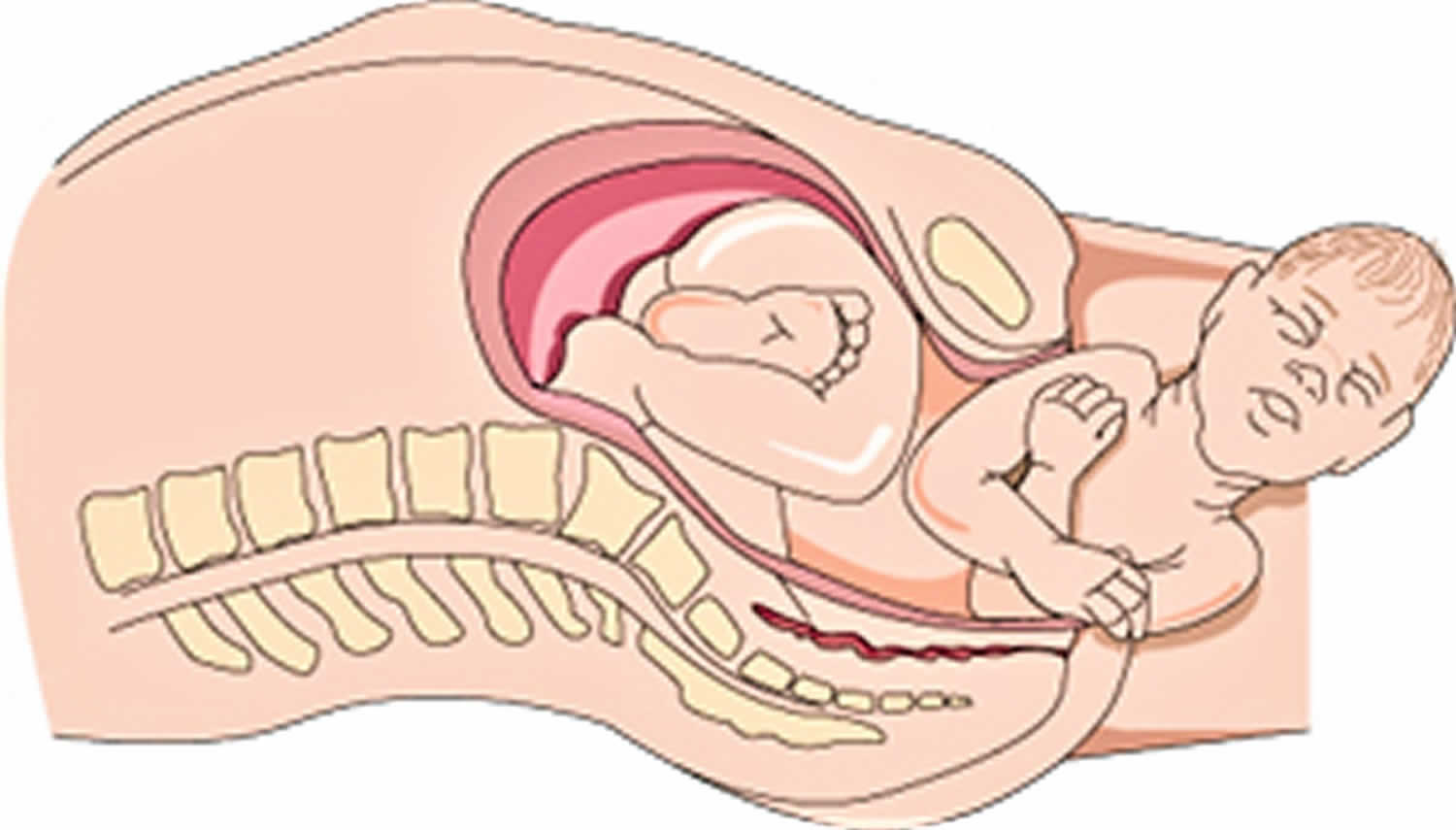
Footnote: The baby twists and turns through the birth canal.
What happens in the third stage of labor?
The third stage involves delivery of the placenta (afterbirth). The third stage is the shortest stage, lasting five to 30 minutes. The placenta grows in your uterus and supplies your baby with food and oxygen through the umbilical cord. Contractions will begin five to 30 minutes after birth, signaling that it’s time to deliver the placenta. You might have chills or shakiness. Labor is over once the placenta is delivered. Your doctor will repair the episiotomy and any tears you might have. Now, you can rest and enjoy your newborn.
During the third stage of labor:
- You have contractions that are closer together and not as painful as earlier. These contractions help the placenta separate from the uterus and move into the birth canal. They begin 5 to 30 minutes after birth.
- You continue to have contractions even after the placenta is delivered. You may get medicine to help with contractions and to prevent heavy bleeding.
- Your doctor squeezes and presses on your belly to make sure the uterus feels right.
- If you had an episiotomy, your doctor repairs it now.
- If you’re storing your umbilical cord blood, your doctor collects it now. Umbilical cord blood is blood left in the umbilical cord and placenta after your baby is born and the cord is cut. Some moms and families want to store or donate umbilical cord blood so it can be used later to treat certain diseases, like cancer. Your instructions about umbilical cord blood can be part of your birth plan.
- You may have chills or feel shaky. Tell your doctor if these are making you uncomfortable.
What you can do:
- Enjoy the first few moments with your baby.
- Start breastfeeding. Most women can start breastfeeding within 1 hour of their baby’s birth.
- Give yourself a big pat on the back for all your hard work. You’ve made it through childbirth!
What happens after my baby is born?
Congratulations! It’s time to hold your baby! Right after birth your doctor places your baby skin-to-skin on your chest and covers him with a blanket. Holding your baby skin-to-skin helps your baby stay warm as he gets used to being outside the womb. It’s also a great way to get started breastfeeding. You can start breastfeeding even within an hour of your baby’s birth. Even if you don’t plan to breastfeed, hold your baby skin-to-skin so you get to know each other right away. Your baby will welcome your gentle touch, and this closeness can help you and your baby bond.
After birth, your body starts to change to help you heal. Your doctor takes your temperature and checks your heart and blood pressure to make sure you’re doing well. If you had anesthesia during labor, your doctor makes sure you’re recovering without any complications.
What is preterm labor?
Preterm and premature mean the same thing — early. Preterm labor is labor that begins too early, before 37 weeks of pregnancy. Preterm labor can lead to premature birth. Premature birth is when your baby is born early, before 37 weeks of pregnancy. Your baby needs about 40 weeks in the womb to grow and develop before birth. Babies born before 37 weeks of pregnancy are called premature. Premature babies (babies born before 37 weeks of pregnancy) can have health problems at birth and later in life. If you’re not to 37 weeks of pregnancy and you have signs or symptoms of preterm labor, call your doctor. Getting help quickly is the best thing you can do. About 1 in 10 babies is born prematurely each year in the United States.
What are the signs and symptoms of preterm labor?
Signs of a condition are things someone else can see or know about you, like you have a rash or you’re coughing. Symptoms are things you feel yourself that others can’t see, like having a sore throat or feeling dizzy.
If you have any of these signs or symptoms before 37 weeks of pregnancy, you may be having preterm labor:
- Change in your vaginal discharge (watery, mucus or bloody) or more vaginal discharge than usual
- Pressure in your pelvis or lower belly, like your baby is pushing down
- Constant low, dull backache
- Belly cramps with or without diarrhea
- Regular or frequent contractions that make your belly tighten like a fist. The contractions may or may not be painful.
- Your water breaks.
What should I do if I think I’m having preterm labor?
If you have even one sign or symptom of preterm labor, call your health care provider right away. If you have preterm labor, getting help quickly is the best thing you can do.
When you see your provider, he may do a pelvic exam or a transvaginal ultrasound to see if your cervix has started to thin out and open for labor. Your cervix is the opening to the uterus (womb) that sits at the top of the vagina (birth canal). A transvaginal ultrasound is done in the vagina instead of on the outside of your belly. Like a regular ultrasound, it uses sound waves and a computer to make a picture of your baby. If you’re having contractions, your provider monitors them to see how strong and far apart they are. You may get other tests to help your provider find out if you really are in labor.
If you’re having preterm labor, your doctor may give you treatment to help stop it or to help improve your baby’s health before birth. Talk to your provider about which treatments may be right for you.
What causes preterm labor and premature birth?
Scientists don’t always know for sure what causes preterm labor and premature birth. Sometimes labor starts on its own without warning. Even if you do everything right during pregnancy, you can still give birth early.
Scientists do know some things may make you more likely than others to have preterm labor and premature birth. These are called risk factors. Having a risk factor doesn’t mean for sure that you’ll have preterm labor or give birth early. But it may increase your chances. Talk to your doctor about what you can do to help reduce your risk.
Because many premature babies are born with low birthweight, many risk factors for preterm labor and premature birth are the same as for having a low-birthweight baby. Low birthweight is when a baby is born weighing less than 5 pounds, 8 ounces.
These three risk factors make you most likely to have preterm labor and give birth early:
- You’ve had a premature baby in the past.
- You’re pregnant with multiples (twins, triplets or more).
- You have problems with your uterus or cervix now or you’ve had them in the past. Your uterus (also called the womb) is where your baby grows inside you.
Medical risk factors before pregnancy for preterm labor and premature birth
- Being underweight or overweight before pregnancy. This can include having an eating disorder, like anorexia or bulimia.
- Having a family history of premature birth. This means someone in your family (like your mother, grandmother or sister) has had a premature baby. If you were born prematurely, you’re more likely than others to give birth early.
- Getting pregnant again too soon after having a baby. For most women it’s best to wait at least 18 months before getting pregnant again. Talk to your provider about the right amount of time for you.
Medical risk factors during pregnancy for preterm labor and premature birth
Having certain health conditions during pregnancy can increase your risk for preterm labor and premature birth, including:
- Connective tissue disorders, like Ehlers-Danlos syndromes (EDS) and vascular Ehlers-Danlos syndrome (vEDS). Connective tissue is tissue that surrounds and supports other tissues and organs. Ehlers-Danlos syndromes can cause joints to be loose and easy to dislocate; skin to be thin and easily stretched and bruised; and blood vessels to be fragile and small. It also can affect your uterus and intestines. Vascular Ehlers-Danlos syndrome is the most serious kind of Ehlers-Danlos syndromes because it can cause arteries and organs (like the uterus) to rupture (burst). Ehlers-Danlos syndromes and vascular Ehlers-Danlos syndrome are genetic conditions that can be passed from parent to child through genes.
- Diabetes. Diabetes is when your body has too much sugar (called glucose) in your blood.
- High blood pressure and preeclampsia. High blood pressure (also called hypertension) is when the force of blood against the walls of the blood vessels is too high. This can stress your heart and cause problems during pregnancy. Preeclampsia is a kind of high blood pressure some women during or right after pregnancy. If not treated, it can cause serious problems and even death.
- Infections, including sexually transmitted infections (STIs) and infections of the uterus, urinary tract or vagina
- Intrahepatic cholestasis of pregnancy. This is the most common liver condition that happens during pregnancy.
- Thrombophilias. These are conditions that increase your risk of making abnormal blood clots.
Other medical risk factors during pregnancy include:
- Getting late or no prenatal care. Prenatal care is medical care you get during pregnancy.
- Not gaining enough weight during pregnancy. This can include having an eating disorder, like anorexia or bulimia.
- Bleeding from the vagina in the second or third trimester
- Preterm premature rupture of the membranes (also called PPROM). Premature rupture of membranes (also called PROM) is when the amniotic sac around your baby breaks (your water breaks) before labor starts. PPROM is when this happens before 37 weeks of pregnancy. If you have any fluid leaking from your vagina, call your provider and go to the hospital.
- Being pregnant after in vitro fertilization (IVF). IVF is a fertility treatment used to help women get pregnant.
- Being pregnant with a baby who has certain birth defects, like heart defects or spina bifida. Birth defects are health conditions that are present at birth. They change the shape or function of one or more parts of the body. Birth defects can cause problems in overall health, how the body develops or how the body works. Spina bifida is a birth defect of the spine.
Risk factors in your everyday life for preterm labor and premature birth:
- Smoking, drinking alcohol, using street drugs or abusing prescription drugs
- Having a lot of stress in your life.
- Low socioeconomic status. Socioeconomic status is a combination of things like your education, your job and your income (how much money you make).
- Domestic violence. This is when your partner hurts or abuses you. It includes physical, sexual and emotional abuse.
- Working long hours or having to stand a lot
- Exposure to air pollution, lead, radiation and chemicals in things like paint, plastics and secondhand smoke. Secondhand smoke is smoke from someone else’s cigarette, cigar or pipe.
Age and race as risk factors for preterm labor and premature birth
Being younger than 17 or older than 35 makes you more likely than other women to give birth early. In the United States, black women are more likely to give birth early. Almost 17 percent of black babies are born prematurely each year. Just more than 10 percent of American Indian or Alaska Native and Hispanic babies are born early, and less than 10 percent of white and Asian babies. We don’t know why race plays a role in premature birth; researchers are working to learn more about it.
Can I reduce my risk for preterm labor and premature birth?
Yes, you may be able to reduce your risk for early labor and birth. Some risk factors are things you can’t change, like having a premature birth in a previous pregnancy. Others are things you can do something about, like quitting smoking.
Here’s what you can do to reduce your risk for preterm labor and premature birth:
- Get to a healthy weight before pregnancy and gain the right amount of weight during pregnancy. Talk to your doctor about the right amount of weight for you before and during pregnancy.
- Don’t smoke, drink alcohol use street drugs or abuse prescription drugs. Ask your doctor about programs that can help you quit.
- Go to your first prenatal care checkup as soon as you think you’re pregnant. During pregnancy, go to all your prenatal care checkups, even if you’re feeling fine. Prenatal care helps your doctor make sure you and your baby are healthy.
- Get treated for chronic health conditions, like high blood pressure, diabetes, depression and thyroid problems. Depression is a medical condition in which strong feelings of sadness last for a long time and interfere with your daily life. It needs treatment to get better. The thyroid is a gland in your neck that makes hormones that help your body store and use energy from food.
- Protect yourself from infections. Talk to your provider about vaccinations that can help protect you from certain infections. Wash your hands with soap and water after using the bathroom or blowing your nose. Don’t eat raw meat, fish or eggs. Have safe sex. Don’t touch cat poop.
- Reduce your stress. Eat healthy foods and do something active every day. Ask family and friends for help around the house or taking care of other children. Get help if your partner abuses you. Talk to your employer about how to lower your stress at work.
- Wait at least 18 months between giving birth and getting pregnant again. Use birth control until you’re ready to get pregnant again. If you’re older than 35 or you’ve had a miscarriage or stillbirth, talk to your provider about how long to wait between pregnancies. Miscarriage is the death of a baby in the womb before 20 weeks of pregnancy. Stillbirth is the death of a baby in the womb after 20 weeks of pregnancy.





{kind=link}