
Contents
Hemifacial microsomia
Hemifacial microsomia also called craniofacial microsomia, first and second branchial arch anomaly, branchial arch syndrome, facioauriculovertebral syndrome, oculoauriculovertebral spectrum, or lateral facial dysplasia, is a term used to describe a spectrum of congenital underdevelopment of the tissues on one side of the face that primarily affect the development of the skull (cranium) and face before birth 1). Hemifacial microsomia primarily affects the ear, mouth and jaw areas, though it may also involve the eye, cheek, neck and other parts of the skull, as well as nerves and soft tissue. In 10 to 15 percent of cases, both sides of the face are affected, often times asymmetrically.
Microsomia means abnormal smallness of body structures. Most people with hemifacial microsomia or craniofacial microsomia have differences in the size and shape of facial structures between the right and left sides of the face (facial asymmetry). In about two-thirds of cases, both sides of the face have abnormalities, which usually differ from one side to the other. Other individuals with hemifacial microsomia are affected on only one side of the face. The facial characteristics in hemifacial microsomia typically include underdevelopment of one side of the upper or lower jaw (maxillary or mandibular hypoplasia), which can cause dental problems and difficulties with feeding and speech. In cases of severe mandibular hypoplasia, breathing may also be affected.
Most children with hemifacial microsomia have facial anomalies but no other major medical issues. In some cases, babies born with hemifacial microsomia may also have other health problems such as malformed vertebrae, heart defects or abnormally shaped kidneys.
Hemifacial microsomia is typically nonprogressive, meaning that the areas of the face that are affected at birth will typically remain similarly affected throughout growth and development, neither worsening nor getting better.
Hemifacial microsomia is the second most common facial birth defect behind cleft lip and palate, affecting one in every 3,500 to 5,600 births 2). However, this range may be an underestimate because not all medical professionals agree on the criteria for diagnosis of hemifacial microsomia and because mild cases may never come to medical attention. For reasons that are unclear, hemifacial microsomia occurs about 50 percent more often in males than in females.
Hemifacial microsomia is sometimes confused with Goldenhar syndrome, a rare congenital condition. People with hemifacial microsomia and noncancerous (benign) growths in the eye called epibulbar dermoids may be said to have Goldenhar syndrome or oculoauricular dysplasia. In fact, hemifacial microsomia is just one of the distinctive characteristics of Goldenhar syndrome, which also includes spine anomalies and epibulbar dermoids or lipodermoids.
Hemifacial microsomia treatment is complex and usually requires multiple stages. The skull, eye socket and cheek bones are generally reconstructed when children are young. Timing for jaw reconstruction will vary depending on whether there are breathing or feeding problems. Ear reconstruction usually occurs in the school age years.
Children with hemifacial microsomia require long-term follow up by a multidisciplinary team. This is a complex condition and experts from different medical, surgical, and dental specialties need to work together to provide the best care for your child. Several operations may be needed as children grow.
It is very important for children with hemifacial microsomia to receive dental care from providers experienced in caring for children with craniofacial conditions.
Figure 1. Diverse manifestations of hemifacial macrosomia
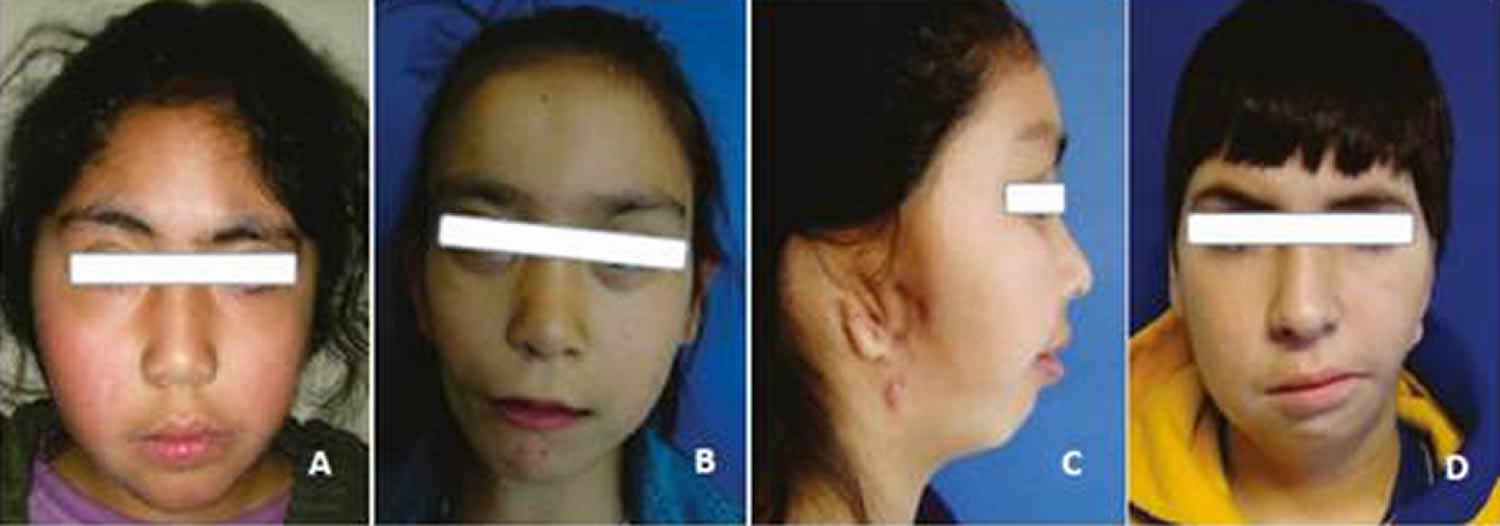
Footnote: The photographs show patients with varying degrees of hemifacial microsomia. In image A, the patient presents a Grade I mandibular disorder, with slight deviation of the lower third. Image B corresponds to a Grade IIA alteration, presenting alteration of symmetry, both at the lower third and the orbits. Image C shows an alteration of the lower third, with full involvement of the right auricle, corresponding to a patient with a Grade IIB anomaly. Image D corresponds to a patient with a Grade III alteration of the left side.
Figure 2. Hemifacial microsomia baby

Figure 3. Hemifacial microsomia teen
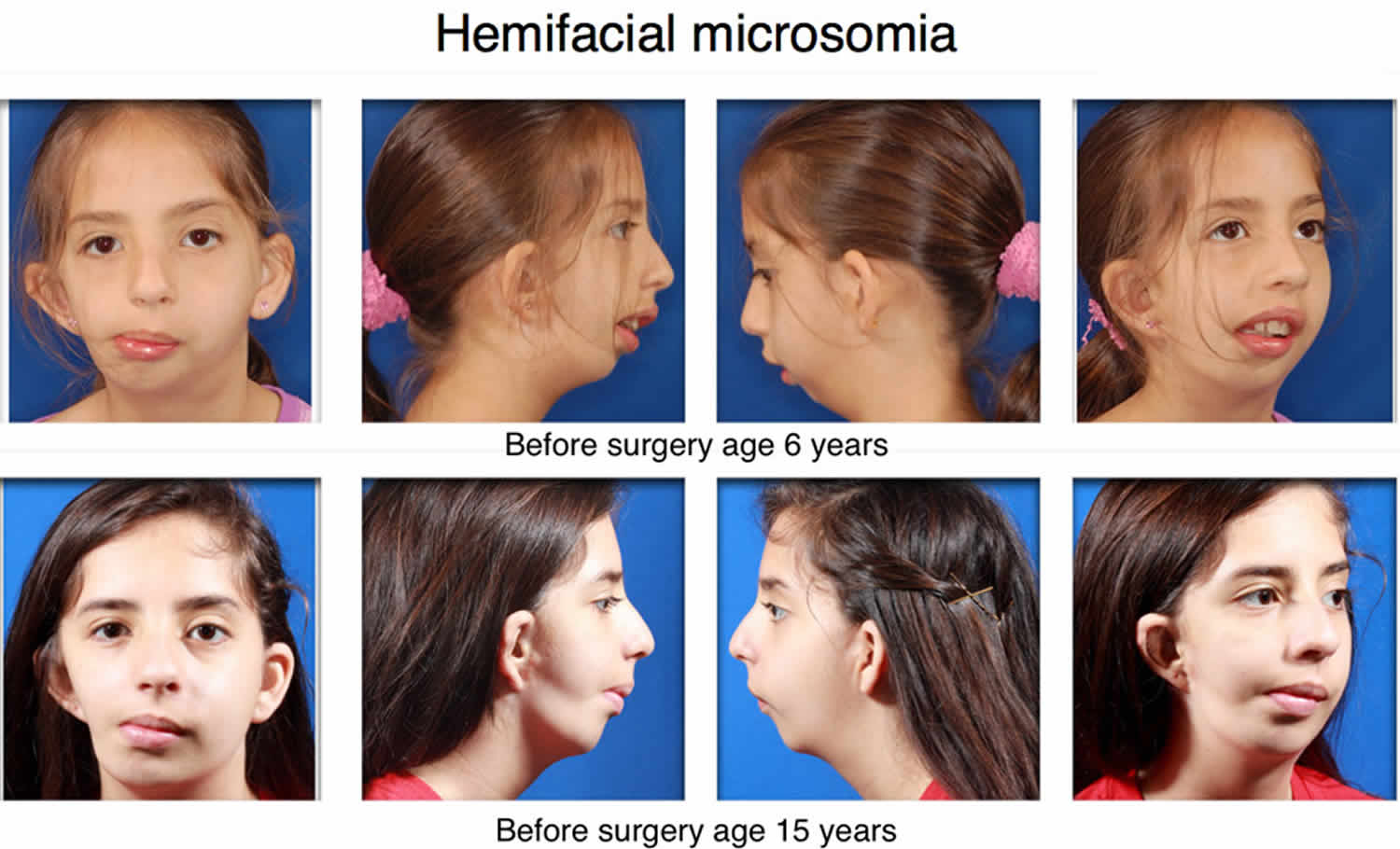
Figure 4. Hemifacial microsomia in adults
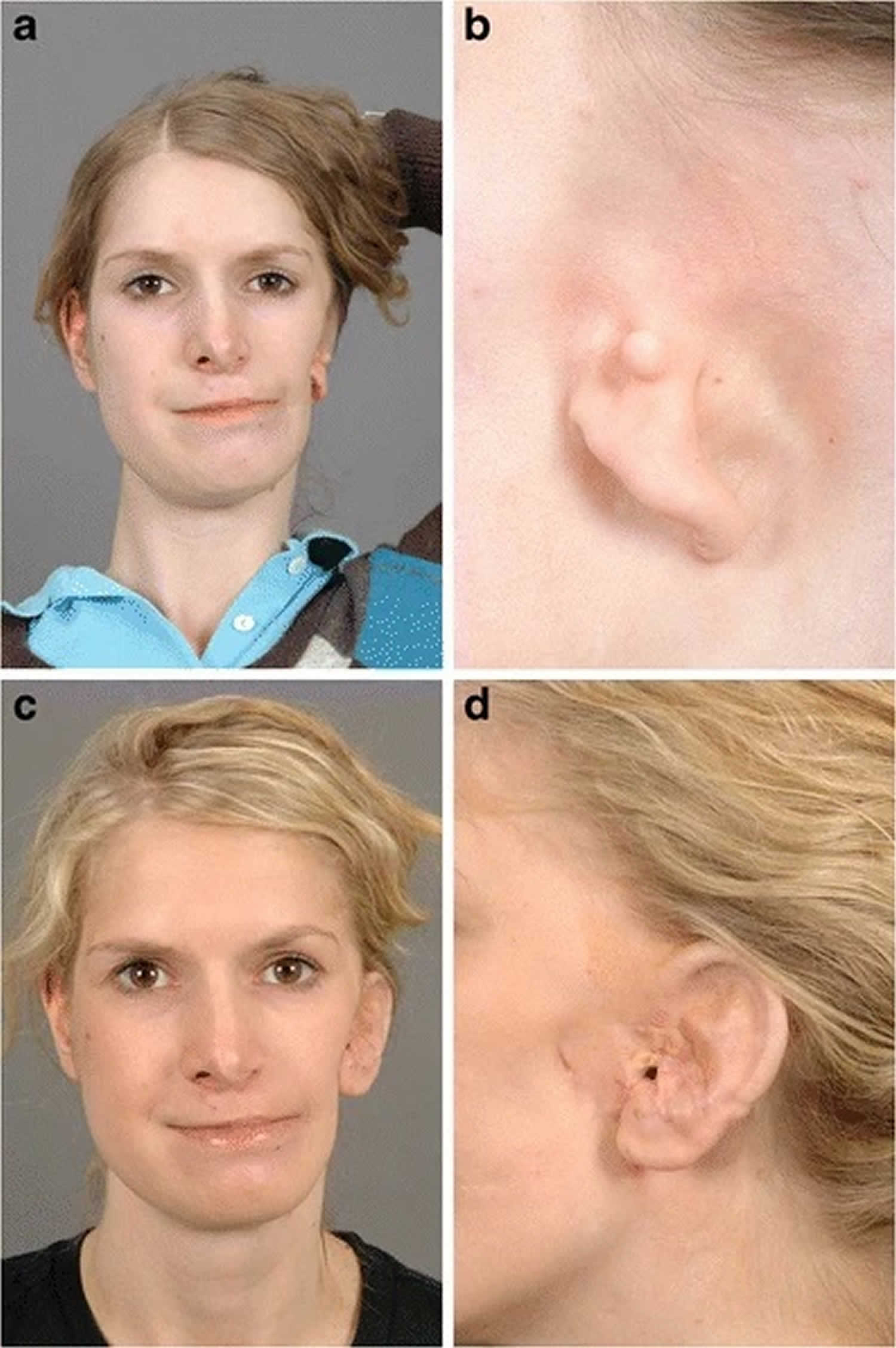
Footnote: Total ear reconstruction in a woman suffering from a severe hemifacial microsomia type 3 with an auricular dysplasia Weerda grade III on the left side, using a porous polyethylene framework and a temporoparietal fascia flap. (A and B) Preoperatively. (C and D) 1 year postoperatively
[Source 3) ]Hemifacial microsomi causes
It is unclear what causes or genes are involved in hemifacial microsomia. Hemifacial microsomia results from problems in the development of structures in the embryo called the first and second pharyngeal arches (also called branchial or visceral arches). Tissue layers in the six pairs of pharyngeal arches give rise to the muscles, arteries, nerves, and cartilage of the face and neck. Specifically, the first and second pharyngeal arches develop into the lower jaw, the nerves and muscles used for chewing and facial expression, the external ear, and the bones of the middle ear. Interference with the normal development of these structures can result in the abnormalities characteristic of hemifacial microsomia.
There are several factors that can disrupt the normal development of the first and second pharyngeal arches and lead to hemifacial microsomia. Research has shown the process starts in the first trimester of pregnancy and may be caused by a vascular problem leading to poor blood supply to the fetus’ face during early development 4). The facial anomalies are not triggered by a mother’s action or diet.
Some individuals with hemifacial microsomia have chromosomal abnormalities such as deletions or duplications of genetic material; these individuals often have additional developmental problems or malformations. Occasionally, hemifacial microsomia occurs in multiple members of a family in a pattern that suggests inheritance of a causative gene mutation, but the gene or genes involved are unknown. In other families, individuals seem to inherit a predisposition to the disorder. The risk of hemifacial microsomia can also be increased by environmental factors, such as certain drugs taken by the mother during pregnancy. In most affected individuals, the cause of the disorder is unknown.
In the majority of hemifacial microsomia cases, the condition is not inherited, and happens by chance. In a small minority of cases, a child may inherit the condition from his parents. An adult with hemifacial microsomia has about a 3 percent chance or less of having a child with the same condition.
It is not well understood why certain disruptions to development affect the first and second pharyngeal arches in particular. Researchers suggest that these structures may develop together in such a way that they respond as a unit to these disruptions.
Hemifacial microsomia inheritance pattern
Hemifacial microsomia most often occurs sporadically (by chance) in a single individual in a family and is not inherited. If the condition is caused by a chromosomal abnormality, it may be inherited from one affected parent or it may result from a new abnormality in the chromosome and occur in people with no history of the disorder in their family.
In 1 to 2 percent of cases, hemifacial microsomia is inherited in an autosomal dominant pattern, which means one copy of an altered gene in each cell is sufficient to cause the disorder. In rare cases, the condition is inherited in an autosomal recessive pattern, which means both copies of a gene in each cell have mutations. The parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition. The gene or genes involved in hemifacial microsomia are unknown.
In some affected families, people seem to inherit an increased risk of developing hemifacial microsomia, not the condition itself. In these cases, some combination of genetic changes and environmental factors may be involved.
Hemifacial microsomi signs and symptoms
People with hemifacial microsomia usually have ear abnormalities affecting one or both ears, typically to different degrees. They may have growths of skin (skin tags) in front of the ear (preauricular tags), an underdeveloped or absent external ear (microtia or anotia), or a closed or absent ear canal; these abnormalities may lead to hearing loss. Eye problems are less common in craniofacial microsomia, but some affected individuals have an unusually small eyeball (microphthalmia) or other eye abnormalities that result in vision loss.
Abnormalities in other parts of the body, such as malformed bones of the spine (vertebrae), abnormally shaped kidneys, and heart defects, may also occur in people with craniofacial microsomia.
The following structures are involved in hemifacial microsomia:
- Jaw and temporomandibular joint (TMJ): asymmetrical mandibular development for hypoplasia, absence of mandibular structures (condyle and ramus), absence or ankylosis of temporomandibular joint (TMJ). Recently published studies showed that hemifacial microsomia patients presented both mandibular and maxillary retrusion in comparison with the control group, along with an increase in the vertical component; these patterns were more marked in the affected side and increased according to severity 5). Mandibular height was always lower along growth, but the growth pattern was similar in both groups 6). In terms of temporomandibular joint (TMJ), it has been observed that the degree of mandible dysplasia does not correspond to the degree of disk dysplasia, which vary among individuals; while the unaffected side does not present major alterations 7)
- Orbit: orbit dystopia (bad position), epibulbar dermoid, anophthalmia/microphthalmia, blepharoptosis, retinal or choroidal coloboma, among other less frequent anomalies 8)
- Ears: microtia, anotia, loss of hearing, disorders of the middle ear.
- Cranial nerves: involvement of facial nerve and, in more severe cases, of the trigeminal and hypoglossal nerves.
- Dental: agenesis 9), dental hypoplasias 10), microdontia, and malocclusions. Delayed tooth development in hemifacial microsomia patients type IIB and III 11), with the most alterations in posterior teeth 12)
- Maxillofacial: labio-palatal fissure 13), macrostomia, hypoplasia of the facial thirds, occlusal plane inclination (highly variable in angle), hypoplasia of masticatory muscles 14), velopharyngeal insufficiency 15)
- Extracranial changes: primarily in kidney, lungs, heart, gastrointestinal, skeletal, and central nervous system (CNS) 16)
Symptoms of hemifacial microsomia range from severe to barely noticeable and depend greatly on the degree of deformity and how much of the face is involved. A child with a mild form of hemifacial microsomia may have a slightly smaller jaw and a skin tag in front of a normal-looking ear. In more severe forms, a child’s face may appear much smaller on one side of his face, with an abnormally shaped or absent ear.
One of the ways clinicians describe and assess the severity of hemifacial microsomia is the OMENS classification 17). The OMENS classification examines the function and appearance of each of the following, looking for characteristics commonly associated with hemifacial microsomia:
- Orbit (eye socket): small and underdeveloped eyes with impaired vision; absent or unformed eye; growths on the eye; one eye appearing smaller than the other, but with normal vision
- Mandible (the jaw bones): underdeveloped upper and lower jaw on one side; crooked jaw; missing, misaligned or overcrowded teeth; cleft lip and/or cleft palate; limited opening or closing of the mouth
- Ear: small skin tags; misshapen or missing external ear; absent or abnormal development of the ear canal resulting in partial or total hearing loss
- Nerves: ranging from mild weakness to partial or full facial paralysis
- Soft tissues (skin, muscle, fat, tendons and ligaments): flattened forehead or cheekbone, unequal cheek fullness, asymmetrical mouth with lateral cleft.
Table 1. Prevalence of selected anomalies in hemifacial microsomia
| Anomalies | Prevalence 1 | ||
|---|---|---|---|
| Principal | Mandible | Mandibular hypoplasia | 49%-100% |
| Malformed glenoid fossa | 24%-27% | ||
| Ear | Microtia | 66%-99% | |
| Preauricular tags | 34%-61% | ||
| Conductive hearing loss | 50%-66% | ||
| Ocular | Orbital dystopia | 15%-43% | |
| Epibulbar dermoids | 4%-35% | ||
| Nerve | VII nerve palsy | 10%-45% | |
| Soft tissue | Masticatory muscle hypoplasia | 85%-95% | |
| Macrostomia | 17%-62% | ||
| Associated craniofacial |
Velopharyngeal insufficiency | 35%-55% | |
| Palatal deviation | 39%-50% | ||
| Cranial skull base abnormalities | 9%-30% | ||
| Cleft lip and/or palate | 15%-22% | ||
| Coloboma of the upper eyelid | 4%-25% | ||
| Hypodontia/dental hypoplasia | 8%-25% | ||
| Lacrimal duct atresia/stenosis | 11%-14% | ||
| Frontal plagiocephaly | 10%-12% | ||
| Sensorineural hearing loss | 6%-16% | ||
| Preauricular sinus | 6%-9% | ||
| Other | Vertebral/rib | 16%-60% | |
| Cervical spine | 21%-42% | ||
| Scoliosis | 11%-26% | ||
| Cardiac | 4%-33% | ||
| Pigmentation | 13%-14% | ||
| Limb | 3%-21% | ||
| Central nervous system | 5%-18% | ||
| Genitourinary | 4%-15% | ||
| Pulmonary | 1%-15% | ||
| Gastrointestinal | 2%-12% | ||
Hemifacial microsomi diagnosis
Hemifacial microsomia diagnosis is mainly clinical, although various complementary tests allow a better analysis of this pathology. The diagnosis of hemifacial microsomia can be made before or after birth. Some of the abnormal facial features are visible during prenatal ultrasound. The majority of children are not diagnosed with hemifacial microsomia until after birth. In this case, craniofacial experts in your hospital will evaluate your child. Experienced physicians will make the diagnosis based on your child’s appearance: the mandibular (jaw) deformity is the hallmark of hemifacial microsomia, and is classified based on the development of the jaw. In the mildest formation, the mandible is nearly normal and only slightly hypoplastic (underdeveloped), while in the most severe cases, a portion of the jaw is missing on the affected side.
Some of the facial characteristics of hemifacial microsomia mimic those seen in children with Treacher Collins syndrome; but hemifacial microsomia differences are typically one-sided or asymmetric, whereas in Treacher Collins, characteristics are similar on both sides of the face.
Diagnostic tests such as X-rays and CT scans may also be used to better examine your child’s bone and cartilage structure in order to make appropriate treatment recommendations.
Hemifacial microsomi treatment
The treatment of hemifacial microsomia varies tremendously from patient to patient and depends on the severity of the condition and long-term needs of the child. Consultation with an experienced craniofacial team is extremely important in achieving the best outcomes for your child 19).
As is the case for any patient with a complex craniofacial deformity, individual treatment varies depending upon the degree of involvement of the various structures. Your child’s individual treatment plan may vary from others similarly affected due to a variety of other factors. It is important that you see an experienced craniofacial team to manage and assess your child’s condition.
Mainly through plastic/orthognathic surgery and orthodontics, the treatment seeks to improve functionality, along with optimum facial symmetry, in order to 20):
- Increase the size of the affected mandibular side and its associated soft tissue.
- Create a joint simulating the temporomandibular joint (TMJ) in cases where it is absent.
- Correct secondary deformities in maxilla.
- Achieve functional occlusion, as well as aesthetic facial and dental appearance.
- Improve and horizontalize the occlusal plane.
- Achieve mouth opening if it is limited.
Conventional orthodontic treatment may initially include functional appliances with the use of rigid acrylic activators, which are individualized according to each case. These devices allow for expansion of affected tissue, taking advantage of patient′s physiological growth. Sometimes they can have height planes on the healthy side, allowing for vertical compensation of the affected area, always bearing in mind that facial midline should be centered with tooth midline. This can later be complemented with conventional fixed orthodontics.
Supportive treatment at birth
If your child is born with hemifacial microsomia, he may require respiratory support or a tracheostomy if the jaw is severely deficient. In most cases, your child’s airway can be managed conservatively.
Due to the presence of the jaw deformity and clefts, your child may experience feeding difficulties. He may receive supplemental feedings through a nasogastric tube to support his growth and weight gain.
If facial paralysis or eyelid abnormalities are present, eye closure may be incomplete and eye protection must be provided either via lubricants or surgical procedures.
Hemifacial microsomia surgery
As your child with hemifacial microsomia grows, he may need surgical treatment based on the severity and area affected. Not all children with hemifacial microsomia have problems in all of these areas.
Being a malformation with abundant phenotypic variation, hemifacial microsomia patients may need other surgeries, depending on the involved structures. A review of craniofacial microsomia performed by Birgfeld and Heike in 2012 21) shows a timeline as a guide in the medical and surgical management of hemifacial microsomia patients, proposed by members of the Seattle Children′s Craniofacial Center, monitoring its progress from birth to adulthood.
Below are some of the interventions your child may need:
- Ears: Some children with abnormally-shaped or missing ears may choose to have a series of reconstructive surgeries to make the ear appear more normal. The first surgery typically occurs after age 6, when your child’s ears have almost reached adult-size. Another option is to make an artificial or prosthetic ear, which also requires several surgeries. In patients with hearing loss, the possibility of repairing atresia of the auditory canal should be evaluated.
- Orbit and eyelid differences: It may involve surgeries of epibulbar dermoid and eyelid coloboma. In cases of changes in size or position of the orbit, the replacement is done around the age of 3 to 4 years. For children with eyelid differences, surgical procedures to reposition the lower lids and corners of the eyes may be required.
- Soft tissue deficiencies: Children with skin, cheek and other soft tissue deficiencies may need augmentation procedures such as fat grafting or tissue transfer.
- Facial nerve: In cases of nerve palsy, the area and degree of involvement should be evaluated; this involvement may be upper (affects the temporal and zygomatic area), lower (buccal, mandibular and cervical area), or total. In the case of oral involvement, the need for facial reanimation should be evaluated. In case of alteration of eyelid movement, some type of treatment should be considered in order to prevent corneal keratitis by exposure.
- Cleft lip or cleft palate: Babies born with cleft lip or palate can have surgical repairs done during the child’s first year. Cleft lip repair is typically performed when your child is 3 to 6 months old, while cleft palate surgery is generally performed when your child is about a year old.
- Lateral facial cleft: A lateral facial cleft is one of the most severe deficiencies found with hemifacial microsomia. It requires a staged reconstruction, similar to the process used in routine repair of cleft lip and palate. In this procedure, surgeons will create a ring of muscle around your child’s mouth, connecting the corners and drawing up the lateral line of the lower lip. This reconstructive procedure also helps with feeding and speaking.
- Bony deficiencies: In mild cases of bony deficiencies, no treatment may be needed. In more severe cases, surgery may be required. Two of the most commonly performed procedures include distraction lengthening of the mandible (most common) and reconstruction of the mandible with a rib or free vascularized fibula graft (less common). For a distraction lengthening of the mandible, a surgeon cuts the mandible (jaw) in the center of its deficient region and implants a small device that allows the two bone segments to be distracted (pulled apart), creating a gap in the bone. New bone begins to form in the gap of the small jaw and the device is slowly widened until the jaw is appropriately-sized. When the jaw bone has been adjusted, it improves facial form and the way the top and bottom teeth fit together. Mandibular distraction may need to be repeated as your child grows.
Mandibular surgery
While the literature is broad in terms of techniques and surgical times, the treatment of hemifacial microsomia patients can be divided into two groups, according to the classification by Kaban-Prusansky: Grade I and Grade IIA patients are treated in the same way, while Grade IIB and Grade III patients are treated similarly among them but different to the first group 22).
Surgical management of the mandible is essential, and mandible bone distraction has several advantages over costochondral graft. These include: increase mandible vertical length, improve asymmetry of soft tissue, produce less blood loss, have better control of progress vector, and obtain a substantial improvement in the biomechanics of the lower mandible 23).
Bone distraction is based on the principle of tension-stress to allow elongation of bone and soft tissue from the controlled separation of bone segments. There are different types of distraction, which can be classified into two areas. According to location, distractors can be extraoral and intraoral; while, according to the amount of vectors with which they work, they can be univectorial or unidirectional or bi-directional (horizontal and vertical plane) or multidirectional (horizontal, vertical and transversal plane) 24).
The choice of distraction appliance depends on various factors, including patient′s age, the degree of malformation severity and the need for mobility of segments. In general, extraoral appliances require a less complex surgery, can achieve longer distraction distances, and allow handling the distraction in the three directions of space, but they leave scars on the skin, are more visible, and may be heavier, presenting patient discomfort. Intraoral devices are less visible and don′t leave facial scars, but have a limited range of motion in space, and their surgery is more complex for both insertion and removal. Re-absorbable devices have recently been developed, allowing for mandibular distraction in a single stage, and achieving progress of 15 to 30 mm 25). In anyways, the surgical simulation in a solid model can help achieve better mandible symmetry, especially in bone distraction with multivector 26).
It is important to stress the need to take into account, besides patient′s growth state, his or her treatment needs, since they vary among patients, and therefore each must be analyzed as a unique case.
Complications
A 2009 literature review 27) compared the stability and complications of bone distraction and the costochondral graft. It found out that both techniques have a similar relapse rate when performing mandibular advancement of 6 to 10 mm. While this review suggests that mandibular bone distraction is less susceptible to major complications, it also points out the it may produce minor complications that also cause patient morbidity, in addition to being affected by other factors such as a long phase of consolidation, distractor cost, patient compliance in activating the distractor and the need for a second surgery to remove the distractor.
Follow-up care
As your child with hemifacial microsomia grows into adolescence, he or she should continue to be monitored by experienced physicians who can adjust treatment plans as needed.
Because multiple body systems may be involved in hemifacial microsomia, continued monitoring for complications and any treatment as needed are important to optimal long-term outcomes.
The many specialists your child may need to see, including:
- A plastic surgeon to manage the stages of surgical repair
- An otolaryngologist (ear, nose and throat specialist) to monitor and treat any nose or throat issues
- A speech therapist to address any speech problems
- An expert from the Pediatric Feeding and Swallowing Center to address any feeding-related issues
- A dentist and/or orthodontist to assess dental health, crowding of teeth and how well the jaw fits together
- A psychologist or social worker to address emotional and psychological issues related to appearance differences and any other concerns
- An orthopedic doctor if your child has cervical spine issues
- A nephrologist if your child has any kidney abnormalities
- A cardiologist is your child has any heart issues
During follow-up visits, diagnostic testing may be done. The goal of continued monitoring is to help spot any irregularities in growth or development and to address health issues as they develop, optimizing long-term outcomes for your child.
References [ + ]





{kind=link}