Contents
Tibial torsion
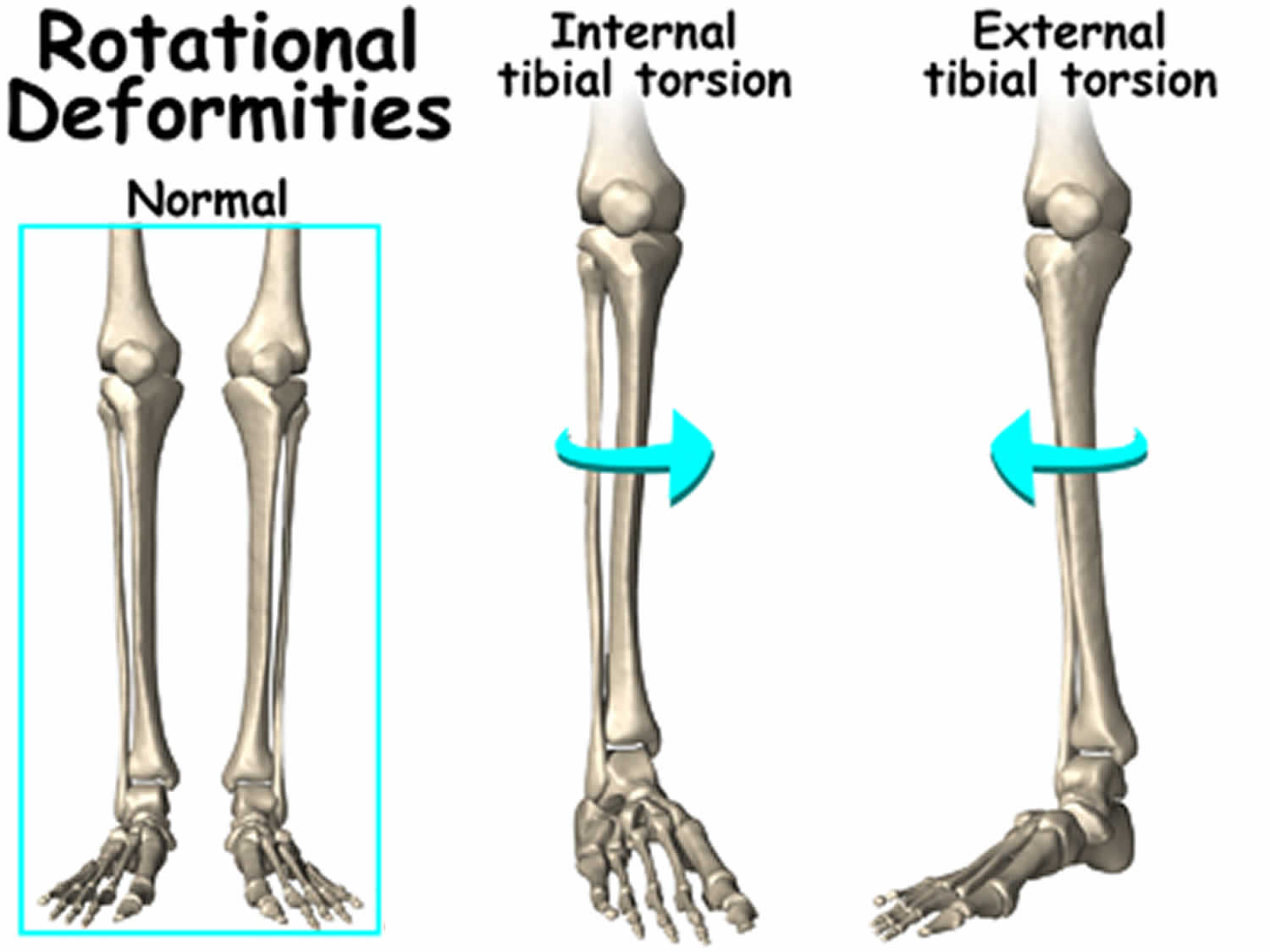
Tibial torsion is an internal or medial rotation of the shin bone (the tibia bone that is located between the knee and the ankle) relative to the upper leg bone (femur). Tibial torsion causes the child’s feet to turn inward, or have what is also known as a “pigeon-toed” appearance. Tibial torsion is typically seen among toddlers (2 to 4-year-old age group) and as the child grows taller, the tibia usually untwists and the condition usually resolves by age 8. Males and females are affected equally, and about two thirds of patients are affected bilaterally 1).
Normally, lateral rotation of the tibia increases from approximately 5º at birth to approximately 15º at maturity 2). Whereas medial tibial torsion improves with time, lateral torsion often worsens because the natural progression is toward increasing external torsion. The ability to compensate for tibial torsion depends on the amount of inversion and eversion present in the foot and on the amount of rotation possible at the hip. Internal torsion causes the foot to adduct, and the patient tries to compensate by everting the foot, externally rotating at the hip, or both. Similarly, persons with external tibial torsion invert at the foot and internally rotate at the hip 3).
The natural history of femoral torsion is to resolve by the time the patient is aged 8 to 10 years. Beyond this age, all remodeling will have occurred, and any further correction is due to a conscious modification of posture 4). However, that does not mean that the child won’t continue to have some intoeing. The child generally grows up to have legs that resemble those of the parent from whom they inherited the trait.
While occasional tripping may occur, most children learn to compensate for any rotation and have no symptoms. There is no need to restrict activities. Many studies have suggested that intoeing may even improve sports function, as intoers tend to be more effective runners and jumpers.
Bars, shoes, orthotics, and twister cables were used in the past to treat intoeing, but there is no scientific evidence that these devices have any effect on the natural tendency toward partial or complete correction by the 8 to 10 years of age.
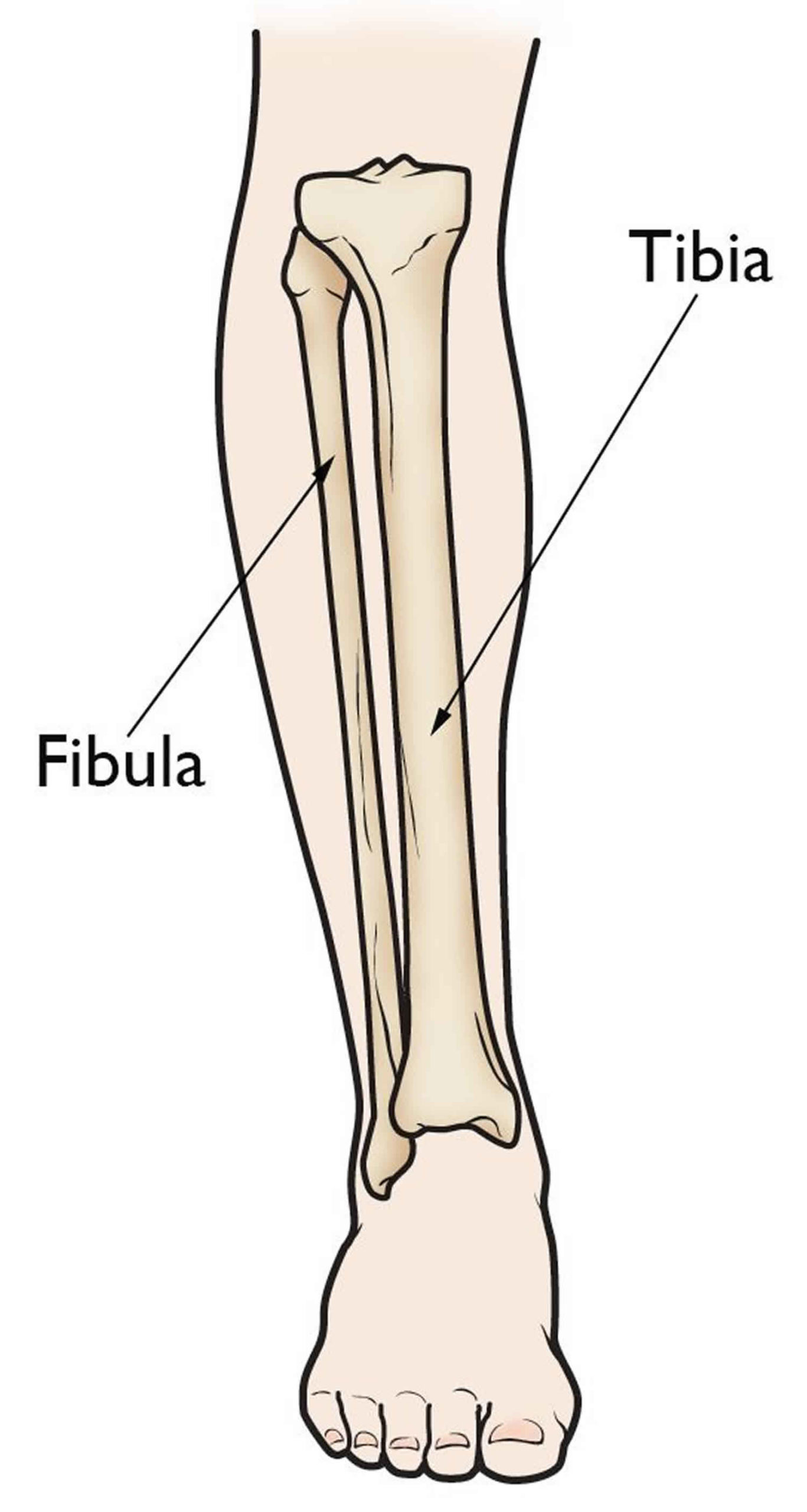
Figure 1. Leg bones
Tibial torsion causes
Tibial torsion can occur due to the position of the baby in the uterus. Tibial torsion also has a tendency to run in families. Typically, a child’s walking style looks like that of his or her parents.
In a study by Mullaji et al 5) to determine tibial torsion norms, individuals in India were found to have less tibial torsion than Caucasians but about the same amount as the Japanese population. The differences in normal tibial torsion values are expected to be caused by the different lifestyles and postures of the different populations, such as cross-legged sitting positions 6).
Tibial torsion signs and symptoms
Tibial torsion, the most common cause of in-toeing. When the child is first learning how to walk, tibial torsion can create an intoeing appearance. As the feet toe in, the legs look like they are bowed. The bowed leg stance actually helps children achieve greater balance as they stand. Their balance is not as steady when they try to stand and walk with their feet close together or with their feet turned out. Besides the cosmetic concerns, internal tibial torsion can predispose kids to tripping and falling, mostly at the end of the day and when they are tired. Children tend to compensate for their tibial torsion by turning their feet outwards (making the feet parallel) during gait. This can give the false impression of geno varum, or bowlegs, because the patella is facing outwards during the gait and creates a “false deformity” during gait.
Parents are generally more concerned about in-toeing than the children are. Severe in-toeing can cause the child to trip or run awkwardly, and it can interfere with participation in sports. Excessive wear is seen along the lateral border of the shoe, mainly in the front half, because the child uses this as the presenting border of the foot on the heel- or foot-strike.
Tibial torsion signs and symptoms include:
- When viewing the child standing, the foot and lower leg appear to be rotated internally. If there is an isolated problem, the kneecaps appear to be straight, thus distinguishing this condition from femoral anteversion in which the kneecaps are pointed in.
- When walking or running the feet excessively turn in occasionally causing tripping and falling. During running the kneecaps continue to stay straight.
- At the end of the day when fatigue sets in the in toe appear to be worse. Maybe asymmetrical (one side worse than the other).
- May appear to be bowlegged (because the musculature in the calf is rotated towards the outside of the lower leg).
- Could be associated with metatarsus adductus in an infant.
Tibial torsion diagnosis
Tibial torsion diagnosis is based on clinical findings, and other investigations generally are not required. Imaging studies may be helpful. However, not every child who undergoes an evaluation because of torsional issues requires any or all imaging tests.
Physical examination
Physical examination must include tests to exclude hip dysplasia, hip and ankle ranges of motion, and knee varus or valgus, which can cause apparent errors in examination.
A rotational profile consists of the following 7):
- Foot progression angle (FPA) 8)
- Tibial version or torsion – Thigh-foot angle (TFA), transmalleolar angle
- Femoral anteversion (hip rotation)
- Shape of the foot
The foot progression angle (FPA) is the angular difference between the axis of the foot and the line of progression.
Foot progression angle (FPA):
- a rough measurement which is obtained during gait by observing the angle of the foot off of the line of progression;
- note that severe foot deformities (club foot) which interfere with the usual measurement;
- normal values: normal FPA is 10-15° of external rotation ;
By convention, external rotation values are positive, and internal rotation values are negative. Degrees of in-toeing are as follows:
- Mild is –5 to –10°
- Moderate is –10 to –15°
- Severe is more than –15°
Tibial version or torsion is the degree of rotation of the tibia along its long axis from the knee to the ankle. It is measured with the patient prone with his or her knees flexed to 90°. It is assessed by using two measures, the thigh-foot angle (TFA) and the transmalleolar angle.
The thigh-foot angle (TFA) is measured with the patient prone and the knees flexed to 90°, with the examiner looking at the feet from above. It is the angle between the line of axis of the thigh and the line along axis of foot. A normal thigh-foot angle (TFA) is 10-15° of external rotation. By convention, external rotation values are positive, and internal rotation values are negative.
The transmalleolar axis is the axis of the line joining the two malleoli. Because the lateral malleolus is normally posterior to the medial malleolus, the transmalleolar axis is externally rotated by 15-20°, as measured with reference to the coronal plane axis. A transmalleolar axis that is externally rotated more than 20° signifies external tibial torsion, and a transmalleolar axis externally rotated less than 10° signifies internal tibial torsion.
Femoral anteversion is the axial angle between the plane of the neck of the femur and the femoral condyles. It can be clinically deduced by measuring hip rotation. Normal range of external rotation is 45-70°, and internal rotation is 10-45°. As femoral anteversion increases, internal rotation increases and external rotation decreases. These children can have as much as 90° of internal rotation and 0° of external rotation. They sit in the W position with their legs turned out (a position not attainable by normal adults), but they cannot sit cross-legged.
The shape of the foot is best assessed with the patient standing and examined from the back, or else the patient can be prone and the feet assessed by looking at the soles. Metatarsus adductus (or, uncommonly, abductus) can be seen.
Imaging studies
Plain radiographs of the hip are obtained to rule out hip dysplasia. Erect-leg full-length radiographs are important for measuring leg lengths, and anteroposterior (AP) and lateral views are important for measuring the distal femoral and proximal and distal tibial angles.
Computed tomography (CT) is the criterion standard 9). Axial sections should be obtained through the hips and femoral necks, the femoral transcondylar axis, and the transmalleolar axis 10). Fluoroscopy and biplane radiography are alternatives.
Rosskopf et al 11) conducted a study to evaluate the interchangeability and reliability of femoral and tibial torsion measurements in children using three-dimensional (3D) models based on biplanar radiography in comparison with CT measurements. They found that femoral and tibial torsion measurements in children using 3D models based on biplanar radiography were comparable with results with CT and that torsion measurements in children on biplanar radiography were as reliable as those on CT images, despite skeletal immaturity.
In children and adolescents, some prefer magnetic resonance imaging (MRI) so as to avoid exposing the patient to radiation 12). Basaran et al 13) assessed the use of MRI to measure tibial torsion in 34 limbs in 17 children (mean age, 7.3 years; range, 3-12 years) and concluded that the most useful parameters for this purpose were the anterior talus angle and the posterior malleolar angle.
Rosskopf et al also compared tibial torsion measurements in children obtained by means of MRI with those from 3D models based on low-dose biplanar radiography 14). They found that tibial torsion measurements differed between the two modalities but that these differences were comparable to measurement variations between CT and biplanar radiography 15).
Tibial torsion treatment
Medial tibial torsion has a benign natural history, because most cases resolve spontaneously, observation with yearly review is all that is generally needed.
Tibial torsion almost always improves without treatment, and usually before school age. Splints, special shoes, and exercise programs do not help. Surgery to re-set the bone may be done in a child who is at least 8 to 10 years old and has a severe twist that causes significant walking problems.
Surgical therapy
Osteotomy for tibial torsion is indicated if the deformity is more than three standard deviations from the mean (less than –10º or more than +35º) 16). Osteotomies (supramalleolar osteotomy) can be performed at any level 17).
Long-term monitoring
The lower extremity is immobilized in a nonweightbearing short leg cast for 4-6 weeks. The cast merely augments the initial stability achieved by using internal fixation. Once the cast is removed at 4-6 weeks after surgery, the healing is generally solid enough to allow removal of the K-wires. Immediate unprotected weightbearing is allowed.
Tibial torsion prognosis
Drexler et al 18) conducted a study to evaluate the clinical and radiographic outcomes of 12 patients (15 knees) undergoing tibial derotation osteotomy and tibial tuberosity transfer for recurrent patella subluxation associated with excessive external tibial torsion. Clinical evaluation was carried out using preoperative and postoperative Knee Society Score, Kujala Patellofemoral score, the Western Ontario and McMaster Universities Osteoarthritis Index questionnaire, the Short Form (SF)-12, and a visual analogue score (VAS) pain scale.
Significant improvement was achieved on all measures 19). Two patients had a nonunion of the tibial osteotomy site, one patient required bone grafting, and another patient required revision to total knee arthroplasty. The investigators concluded that for patients with recurrent patella subluxation secondary to excessive external tibial torsion, satisfactory outcomes in terms of pain relief and improved function can be achieved through tibial derotation osteotomy and tibial tuberosity transfer.
In a study of surgical treatment of 44 children with torsional malalignment of the tibia, Erschbamer et al 20) performed 71 percutaneous derotational osteotomies of the distal tibia. followed by application of an external fixator. On postoperative radiographs, accurate tibial derotation and pin placement were noted in all patients. In nine patients, superficial pin-tract infections developed but resolved with administration of antibiotics; in two. fractures developed after the external fixator was removed but healed in a plaster cast. The investigators found this approach to be safe, effective, and well tolerated.
References [ + ]





{kind=link}