Contents
- Brain tumor in children
- The central nervous system
- Brain tumor in children types
- Brain tumor in children causes
- Brain tumor symptoms in children
- Brain tumor in children diagnosis
- Brain tumor in children treatment
- Brain tumor in children survival prognosis
- Brain tumor in children survival rates
Brain tumor in children
Brain and spinal cord tumors in children tend to be different from those in adults. In general, children diagnosed with a malignant tumor will have a better outlook than adults. They often form in different places, develop from different cell types, and may have a different treatment and prognosis (outlook). In general, brain tumors in children are very rare. Brain and spinal cord tumors are the second most common cancers in children (after leukemia). They account for about 1 out of 4 childhood cancers. More than 4,000 brain and spinal cord tumors are diagnosed each year in children and teens. The incidence rate (number of tumors per 100,000 children) has not changed much in recent years.
Malignant (fast-growing) brain and spinal cord tumors are slightly more common in boys, while non-malignant tumors are slightly more common in girls.
About 3 out of 4 children with brain tumors (all types combined) survive at least 5 years after being diagnosed. But the outlook can vary a great deal based on the type of tumor, where it is, and other factors.
Brain tumors can directly destroy brain cells. They can also indirectly damage cells by pushing on other parts of the brain. This leads to swelling and increased pressure inside the skull.
Brain tumors are not a single kind of tumor, but include several different tumor types. As a group, these are the most common solid tumors in children less than 15 years of age, and account for approximately 20% of all cancers diagnosed in this population. Other important facts about tumors that occur in the brain and spinal cord include the following:
- Tumors can arise at any age in any area of the brain and spinal cord, although some specific types of pediatric tumors tend to occur more often in certain parts of the brain.
- Brain tumors are categorized by the type of malignant cell and by the area of the brain in which they develop.
- The terms “benign” and “malignant” as usually applied to tumors are not as useful when describing CNS tumors. Because the brain and skull are located inside a fixed amount of space, even “benign” or slow-growing tumors can cause serious problems.
- Most brain tumors tend NOT to “metastasize” or spread to distant areas to other parts of the body outside the brain and/or spinal cord (central nervous system). They do, however, tend to recur locally, or spread to other areas of the central nervous system (CNS).
Tumors in any part of the brain might raise the pressure inside the skull (known as intracranial pressure). This can be caused by growth of the tumor, swelling in the brain, or blocked flow of cerebrospinal fluid. Increased pressure can lead to general symptoms such as:
- Headache. Headaches that get worse over time and worse in the morning are a common symptom of brain tumors. But not all brain tumors cause headaches, and most headaches are not caused by tumors.
- Nausea
- Vomiting
- Crossed eyes or blurred vision
- Balance problems
- Behavior changes
- Seizures. In some children, seizures are the first symptom of a brain tumor. Most seizures in children are not caused by brain tumors, but if your child has a seizure, your child’s doctor may refer you to a neurologist (a doctor who specializes in brain and nervous system problems) to make sure it wasn’t caused by a brain tumor or other serious disease.
- Drowsiness or even coma.
In the first few years of life, other symptoms of tumors can include:
- Irritability
- Loss of appetite
- Developmental delays
- Drop in intellectual and/or physical abilities
- Increased head size, sometimes along with bulging of the soft spots of the skull (fontanelles)
In the school-aged child, other general symptoms of tumors can include poor school performance, fatigue, and personality changes.
If the child can cooperate, the doctor can sometimes tell if pressure inside the skull is increased by looking inside the child’s eyes for swelling of the optic nerve (known as papilledema).
Treatment for childhood brain cancer may involve:
- Surgery
- Chemotherapy
- Radiotherapy
- Steroids may also be given to decrease the swelling caused by the tumor.
Your child may undergo some or all of these treatments, depending on their tumor type and grade, your child’s age, overall health and medical history, and your family preferences.
In many children, treatment will cause all signs of the cancer to disappear (remission). Because a child’s nervous system is still developing, some children may have a physical, behavioral or learning disability as a result of the tumor or treatment.
Brain tumor in children key points
- Brain tumors are the most common solid tumors affecting children and adolescents, with close to 5,000 children diagnosed each year.
- There are more than 120 different kinds of brain tumors, depending on where they occur and what kinds of cells they are made of. For instance, meningiomas form in the meninges, and gliomas are composed of glial cells.
- Some forms of brain cancer can be life-threatening. But not all brain tumors are life-threatening. Meningiomas, the most common brain tumor, are often benign and can be treated with surgery.
- Tumor grading is a way of ranking how serious the tumor is – how likely it is to grow and spread.
- Proper diagnosis is essential in determining the best course of treatment for you. Treatment may involve imaging, biopsy and other tests.
- Because of their location, some pediatric brain tumors and their required treatments can cause significant long-term impairment to intellectual and neurological function.
See a doctor if your child develops headaches that do not go away or other symptoms of a brain tumor.
Go to the emergency room if your child develops any of the following:
- Physical weakness
- Change in behavior
- Severe headache of unknown cause
- Seizure of unknown cause
- Vision changes
- Speech changes
What are the differences between cancers in adults and children?
The types of cancers that develop in children are often different from the types that develop in adults. Unlike many cancers in adults, childhood cancers are not strongly linked to lifestyle or environmental risk factors. And only a small number of childhood cancers are caused by DNA (gene) changes that are passed from parents to their child.
- Treatment is often more successful: With some exceptions, childhood cancers tend to respond better to certain treatments. This might be because of differences in the cancers themselves, as well as because children often get more intense treatments. Also, children usually don’t have many of the other health problems that adults with cancer might have, which can often get worse with treatment.
- Long-term side effects are more of a concern: On the other hand, children’s bodies are still growing, and they’re more likely to have side effects from some types of treatment. For example, children (especially very young children) are more likely to be affected by radiation therapy. Many cancer treatments also can cause long-term side effects, so children who have had cancer will need careful follow-up for the rest of their lives.
- Children with cancer are treated at pediatric cancer centers: In the United States, most children and teens with cancer are treated at a center that is a member of the Children’s Oncology Group (https://childrensoncologygroup.org). All of these centers are associated with a university or children’s hospital. These centers offer the advantage of being treated by a team of specialists who know the differences between adult and childhood cancers, as well as the unique needs of children and teens with cancer and their families. This team usually includes pediatric oncologists (childhood cancer doctors), surgeons, radiation oncologists, pediatric oncology nurses, physician assistants and nurse practitioners. These centers also have psychologists, social workers, child life specialists, nutritionists, rehabilitation and physical therapists, and educators who can support and educate the entire family.
Can brain and spinal cord tumors in children be found early?
Screening is testing for a disease (such as brain or spinal cord tumors) in people without any symptoms. At this time there are no widely recommended screening tests for most children to look for brain or spinal cord tumors before they start to cause symptoms. These tumors usually are found as a result of signs or symptoms the child is having.
Most often, the outlook for children with brain or spinal cord tumors depends more on the type of tumor and its location than on how early it is detected. But as with any disease, earlier detection and treatment is likely to be helpful.
For children with certain inherited syndromes that put them at higher risk for brain tumors, such as neurofibromatosis or tuberous sclerosis, doctors often recommend frequent physical exams and other tests. These tests might find tumors when they are still small. Not all tumors related to these syndromes may need to be treated right away, but finding them early might help doctors monitor them so that they can be treated quickly if they begin to grow or cause problems.
The central nervous system
To understand brain and spinal cord tumors, it helps to know about the normal structure and function of the central nervous system (CNS), which is the medical name for the brain and spinal cord.
The brain is the center of thought, feeling, memory, speech, vision, hearing, movement, and much more. The spinal cord and special nerves in the head, called cranial nerves, carry messages between the brain and the rest of the body. These messages tell our muscles how to move, transmit information gathered by our senses, and help coordinate the functions of our internal organs.
The brain is protected by the skull. Likewise, the spinal cord is protected by the bones (vertebrae) of the spinal column.
The brain, like the spinal cord, is composed of gray and white matter. Gray matter—the seat of the neurosomas, dendrites, and synapses—forms a surface layer called the cortex over the cerebrum and cerebellum, and deeper masses called nuclei surrounded by white matter. White matter lies deep to the cortical gray matter in most of the brain, opposite from the relationship of gray and white matter in the spinal cord. As in the spinal cord, white matter is composed of tracts, or bundles of axons, which here connect one part of the brain to another and to the spinal cord.
The brain and spinal cord are surrounded and cushioned by a liquid called cerebrospinal fluid (CSF). Cerebrospinal fluid is made by the choroid plexus, which is in spaces in the brain called ventricles. The ventricles and the spaces around the brain and spinal cord are filled with CSF.
The main areas of the brain include the cerebrum, cerebellum, and brain stem. Each area has a special function.
- Cerebrum: The cerebrum is the large, outer part of the brain. It is made up of 2 hemispheres (halves) and controls reasoning, thought, emotion, and language. It is also responsible for planned (voluntary) muscle movements (throwing a ball, walking, chewing, etc.) and for taking in and interpreting sensory information such as vision, hearing, smell, touch, and pain.
- Cerebellum: The cerebellum lies under the cerebrum at the back part of the brain. It helps coordinate movement.
- Brain stem: The brain stem is the lower part of the brain that connects to the spinal cord. It has bundles of very long nerve fibers that carry signals controlling muscles and sensation or feeling between the cerebrum and the rest of the body. Special centers in the brain stem also help control breathing and the heart beating. In addition, most cranial nerves (described below) start in the brain stem. Because the brain stem is a small area that is so essential for life, it might not be possible to surgically remove tumors in this area.
- The brain stem is divided into 3 main parts: the midbrain, pons, and medulla oblongata.
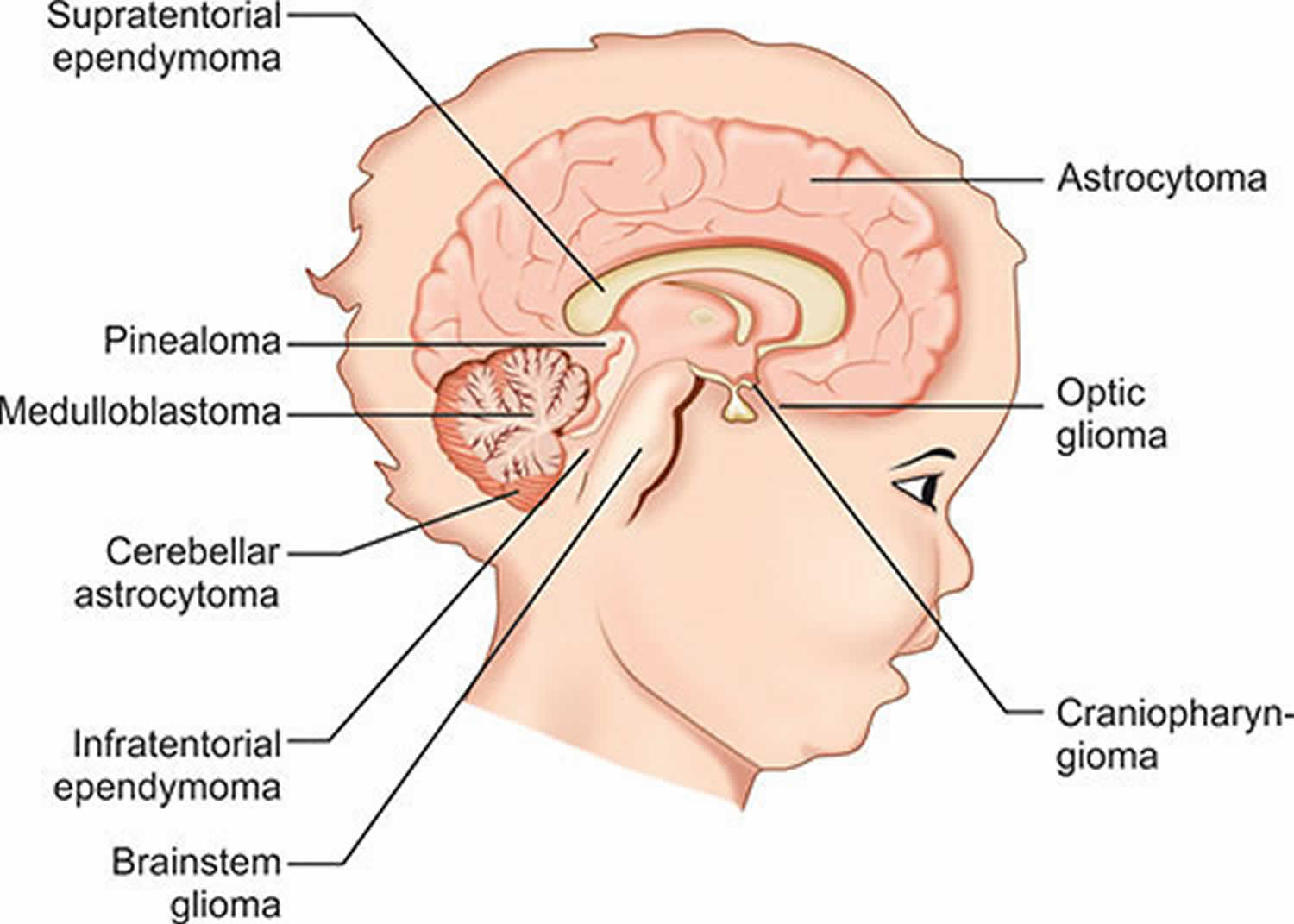
- Cranial nerves: The cranial nerves extend directly out of the base of the brain (as opposed to coming out of the spinal cord). These nerves carry signals directly between the brain and the face, eyes, tongue, mouth, and some other areas. The most common cranial nerve tumors in children are called optic gliomas, which are tumors of the optic nerve (the large nerve that runs between the brain and each eye).
- Spinal cord: The spinal cord has bundles of very long nerve fibers that carry signals that control muscles, sensation or feeling, and bladder and bowel control.
Figure 1. Human brain
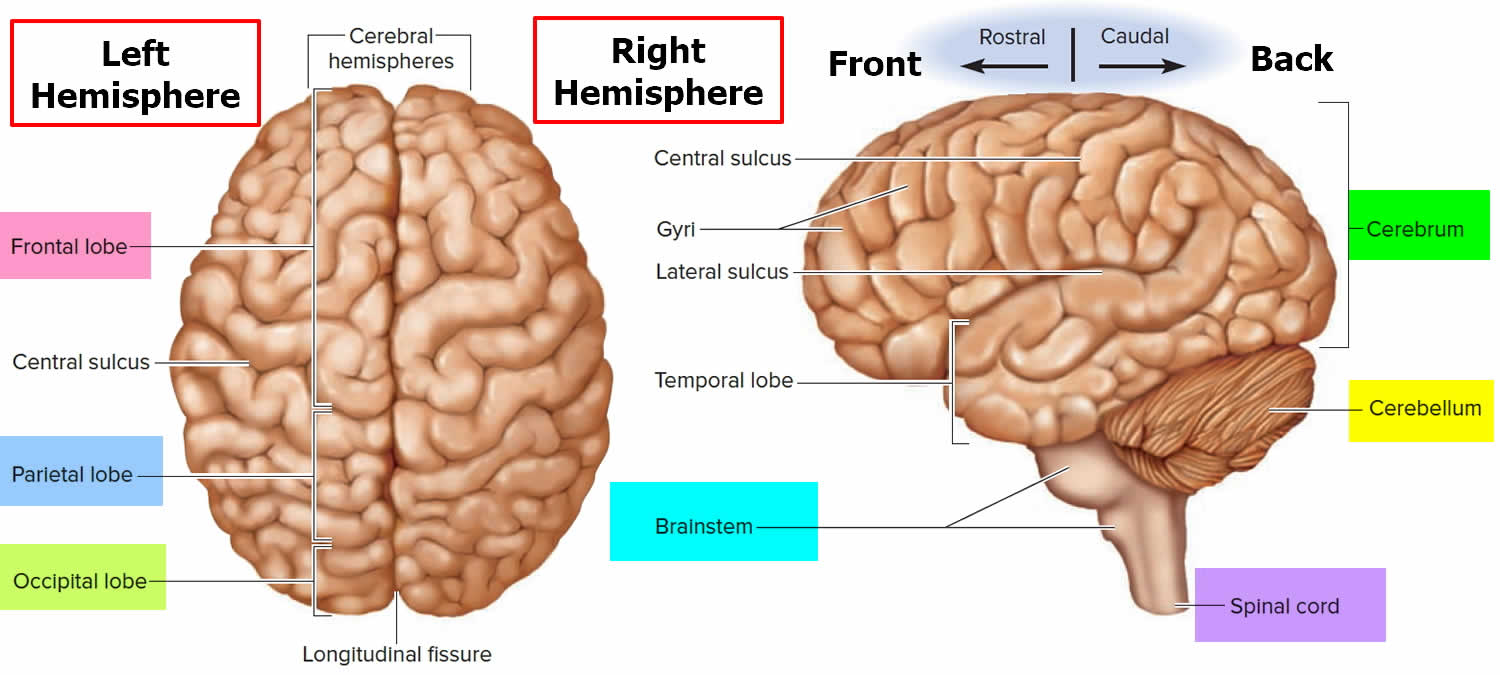
Figure 2. Medial aspect of the human brain
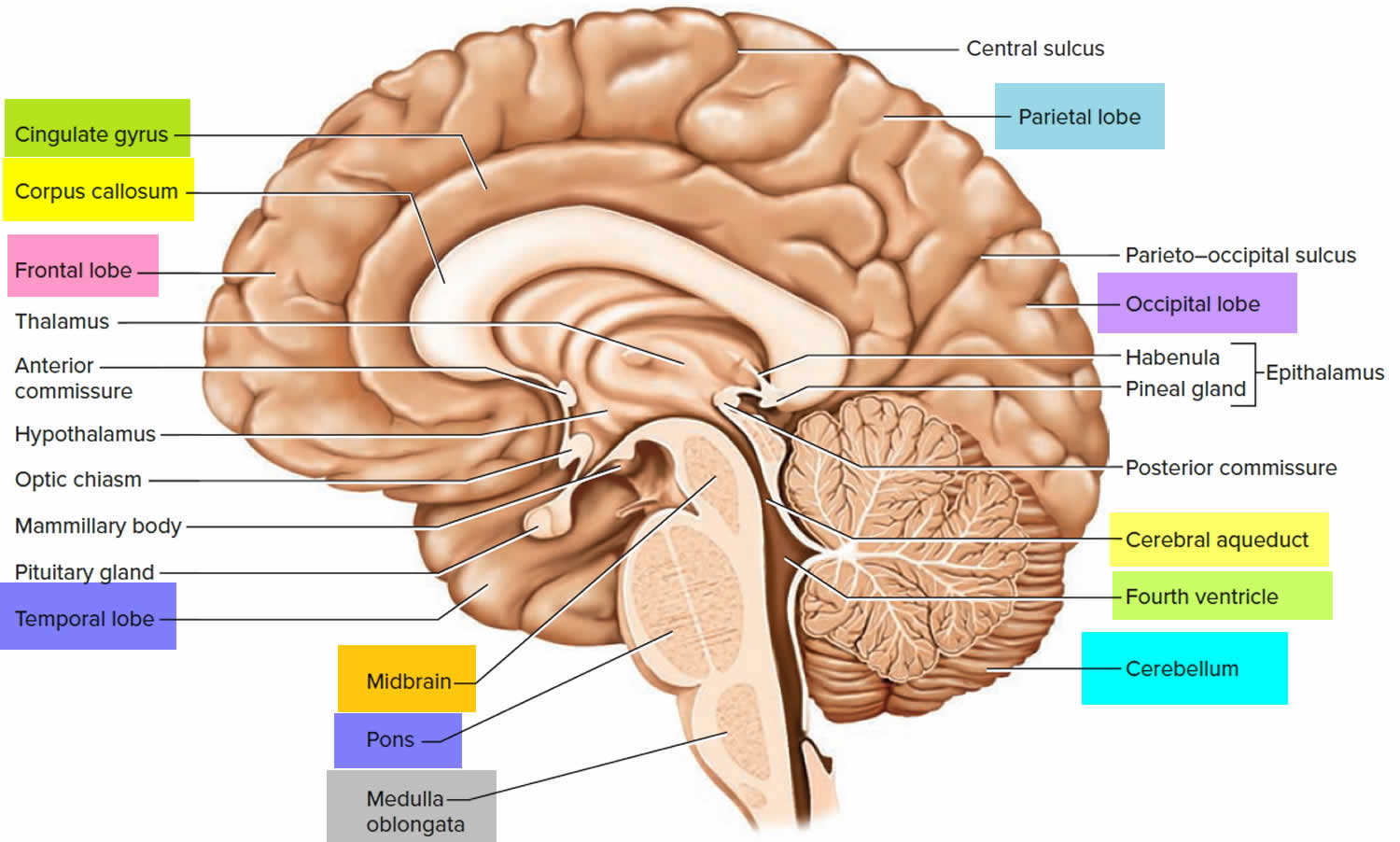
Figure 3. Ventricles of the brain
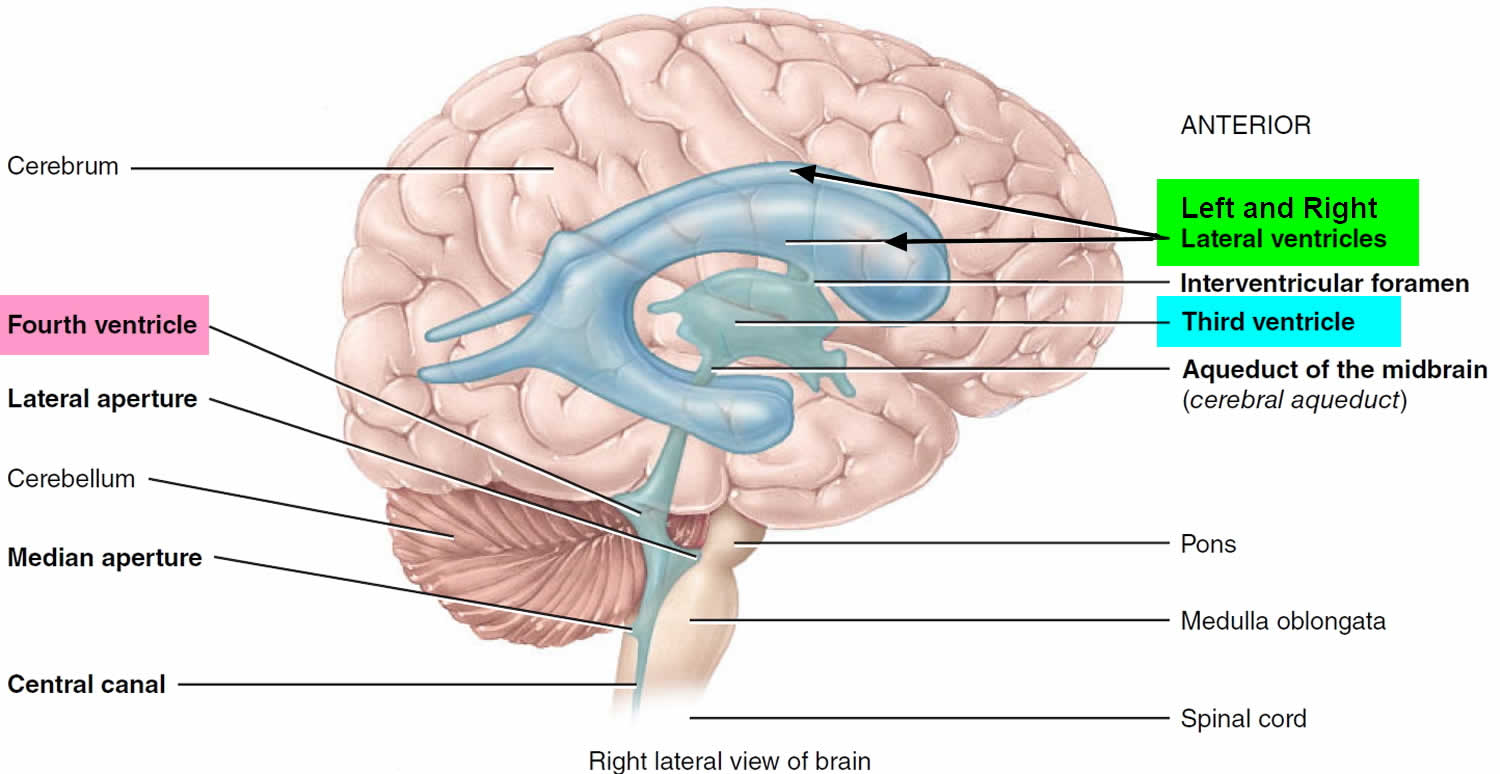
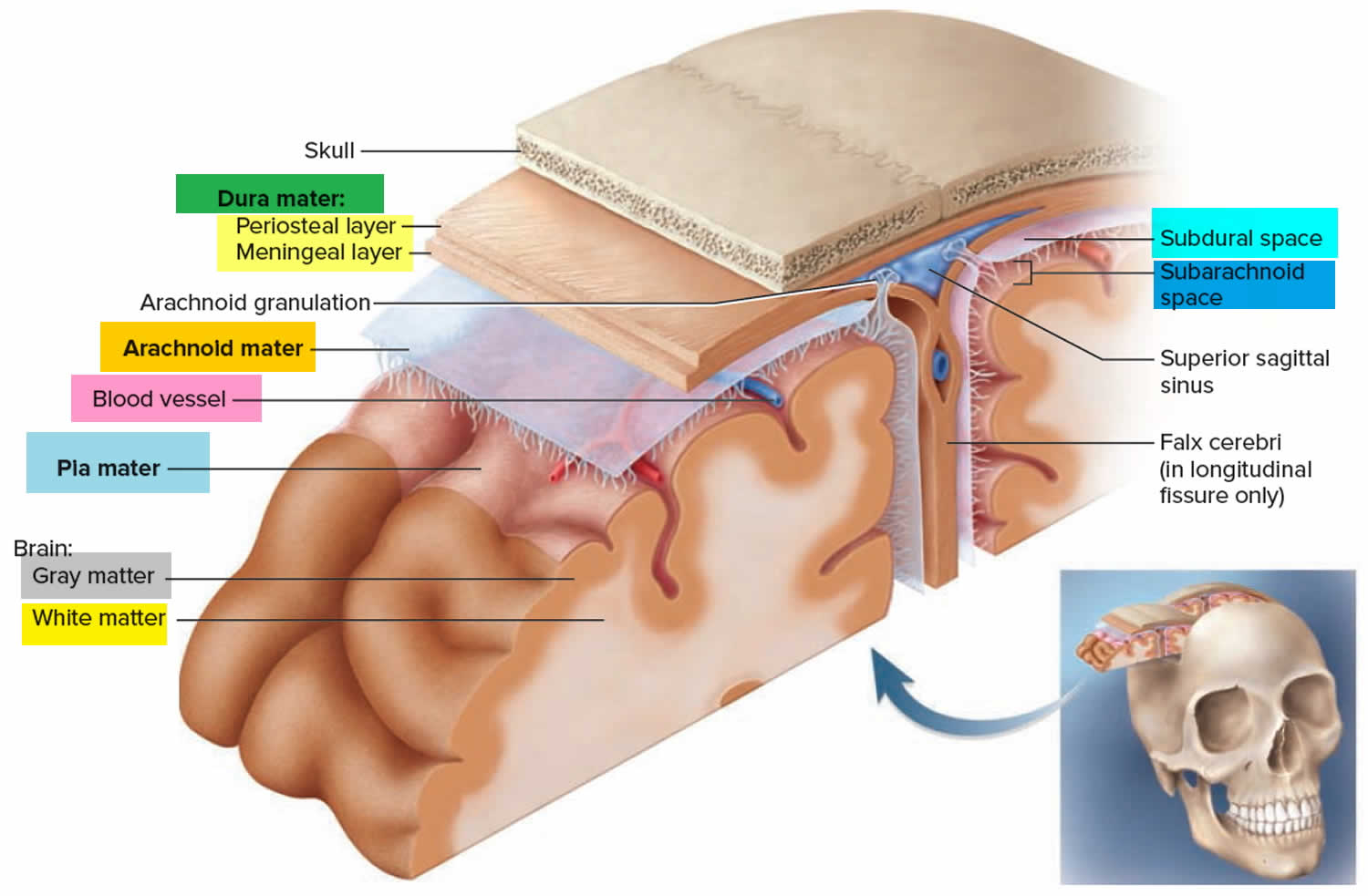
Figure 4. Meninges of the brain
Types of cells and body tissues in the brain and spinal cord
The brain and spinal cord have many kinds of tissues and cells, which can develop into different types of tumors.
- Neurons (nerve cells): These are the cells in the brain that help determine thought, memory, emotion, speech, muscle movement, sensation, and just about everything else that the brain and spinal cord do. They do this by transmitting chemical and electric signals through their nerve fibers (axons). Axons in the brain tend to be short, while those in the spinal cord can be as long as several feet. Unlike many other types of cells that can grow and divide to repair damage from injury or disease, neurons in the brain and spinal cord largely stop dividing about a year after birth (with a few exceptions). Neurons do not usually form tumors, but they can be damaged by tumors that start nearby.
- Glial cells: Glial cells are the supporting cells of the brain. Most brain and spinal cord tumors develop from glial cells. These tumors are sometimes referred to as a group called gliomas.
- There are 3 main types of glial cells:
- Astrocytes help support and nourish neurons. When the brain is injured, astrocytes form scar tissue that helps repair the damage. The main tumors starting in these cells are called astrocytomas or glioblastomas.
- Oligodendrocytes make myelin, a fatty substance that surrounds and insulates the nerve cell axons of the brain and spinal cord. This helps neurons send electric signals through the axons. Tumors starting in these cells are called oligodendrogliomas.
- Ependymal cells line the ventricles (fluid-filled areas) within the central part of the brain and form part of the pathway through which cerebrospinal fluid (CSF) flows. Tumors starting in these cells are called ependymomas.
- A fourth type of cell, called microglia, are the infection-fighting cells of the central nervous system. They are part of the immune system and are not truly glial cells.
- There are 3 main types of glial cells:
- Neuroectodermal cells: These are very early forms of nervous system cells that are probably involved in brain cell development. They are found throughout the brain. The most common tumors that come from these cells are called medulloblastomas, which start in the cerebellum.
- Meninges: These are layers of tissue that cover and protect the brain and spinal cord. The meninges help form the spaces through which CSF travels. The most common tumors that start in these tissues are called meningiomas.
- Choroid plexus: The choroid plexus is the area of the brain within the ventricles that makes CSF, which nourishes and protects the brain. Tumors that start here include choroid plexus papillomas and choroid plexus carcinomas.
- Pituitary gland and hypothalamus: The pituitary is a small gland at the base of the brain. It is connected to a part of the brain called the hypothalamus. Both make hormones that help regulate the activity of several other glands in the body. For example, they control the amount of thyroid hormone made by the thyroid gland, the production and release of milk by the breasts, and the amount of male or female hormones made by the testicles or ovaries. They also make growth hormone, which stimulates body growth, and vasopressin, which regulates water balance by the kidneys. The growth of tumors in or near the pituitary or hypothalamus, as well as surgery and/or radiation therapy in this area, can affect these functions. For example, tumors starting in the pituitary gland sometimes make too much of a certain hormone, which can cause problems. On the other hand, a child may have low levels of one or more hormones after treatment and may need to take hormones to make up for this.
- Pineal gland: The pineal gland is not really part of the brain. It is a small endocrine gland that sits between the cerebral hemispheres. It makes melatonin, a hormone that regulates sleep, in response to changes in light. The most common tumors of the pineal gland are called pineoblastomas.
- Blood-brain barrier: The inner lining of the small blood vessels (capillaries) in the brain and spinal cord creates a very selective barrier between the blood and the tissues of the central nervous system. This barrier normally helps maintain the brain’s metabolic balance and keeps harmful toxins from getting into the brain. Unfortunately, it also keeps out most chemotherapy drugs that are used to kill cancer cells, which in some cases limits their usefulness.
Brain tumor in children types
Brain tumors can be categorized as:
- Primary: Primary brain tumor starts with an abnormal brain cell and grows in the brain.
- Metastatic: Metastatic (secondary) tumor starts as a cancer in another part of the body and then spreads to the brain, where it forms a new tumor.
- Benign: Slow-growing; non-cancerous. Benign tumors can still be difficult to treat if they are growing in or around certain structures of the brain.
- Malignant: Cancerous. Unlike benign tumors that tend to stay contained, malignant tumors can be very aggressive. They grow rapidly and can spread to areas near the original tumor and to other areas in the brain.
- The type of tumor (based on the type of cell it starts from): Tumors can form in almost any type of tissue or cell in the brain or spinal cord. Some tumors have a mix of cell types. Different types of tumors tend to start in certain parts of the brain or spinal cord, and tend to grow in certain ways.
- The grade of the tumor: Some types of brain and spinal cord tumors are more likely to grow into nearby tissues (and to grow quickly) than are others. Brain and spinal cord tumors are typically divided into 4 grades (using Roman numerals I to IV), based largely on how the tumor cells look under a microscope. The higher the grade, the more quickly the tumor is likely to grow:
- Lower grade (grade 1 or 2) tumors tend to grow more slowly and are less likely to grow into (invade or infiltrate) nearby tissues.
- Higher grade (grade 3 or 4) tumors tend to grow quickly and are more likely to grow into nearby tissues. These tumors often require more intensive treatment.
- Gene changes in the tumor cells: Even for a specific type of tumor, the changes in the genes of the tumor cells can be different. For example, many types of tumors are now divided based on whether the cells have mutations in one of the IDH genes. For a specific type of tumor, those with IDH mutations tend to have a better outlook than those without a mutation. Other gene mutations can also be important for certain types of tumors.
- The location of the tumor: Where the tumor is in the brain and spinal cord can affect what symptoms it causes, as well as which treatments might be best. Brain tumors in children are more likely to start in the lower parts of the brain, such as the cerebellum and brain stem, than they are in adults. But they can start in the upper parts of the brain as well.
Gliomas
Gliomas are not a specific type of tumor. Glioma is a general term for a group of tumors that start in glial cells (the supporting cells of the brain). A number of tumors can be considered gliomas, including:
- Astrocytomas (which include glioblastomas)
- Oligodendrogliomas
- Ependymomas
- Brain stem gliomas
- Optic gliomas
About half of all brain and spinal cord tumors in children are gliomas.
Astrocytomas
Astrocytomas are the most common type of glioma, accounting for about half of all childhood brain tumors, most often in the cerebrum (the large upper part of the brain), but also in the cerebellum (the lower back part of the brain). Astrocytomas are most common in children between the ages of 5 and 8. Astrocytomas are tumors that start in glial cells called astrocytes, a kind of glial cell that helps support and nourish nerve cells.
The grade of an astrocytoma is important. Your child’s treatment will be based on whether or not the tumor is slow-growing (low-grade, grade 1 or 2) or fast-growing (high-grade, grade 3 or 4). Most astrocytomas in children (80 percent) are low-grade. Sometimes they begin in the spine or spread there.
Some astrocytomas can spread widely throughout the brain and blend with the normal brain tissue, which can make them hard to remove by surgery. Sometimes they spread along the cerebrospinal fluid (CSF) pathways. It is very rare for them to spread outside of the brain or spinal cord.
As with other brain tumors, astrocytomas are often grouped by grade.
Low-grade (grade 1 or 2) astrocytomas tend to grow slowly and are the most common type in children. Some types, known as non-infiltrating astrocytomas, are grade I tumors that tend to grow very slowly and do not grow into (infiltrate) nearby tissues, so they often have a good prognosis.
- Pilocytic astrocytomas are grade 1 tumors that tend to grow slowly and rarely grow into nearby tissues. Pilocytic astrocytoma is often cystic (fluid-filled). They most commonly occur in the cerebellum but can also begin in the optic nerve, hypothalamus, brain stem, or other areas. Pilocytic astrocytoma slow-growing tumor is the most common brain tumor found in children. They account for nearly 1 out of 5 brain tumors in children. When this tumor develops in the cerebellum, surgical removal is often the only treatment necessary. Pilocytic astrocytomas growing in other locations may require other therapies.
- Subependymal giant cell astrocytomas (SEGAs) occur in the ventricles (spaces in the brain). They are grade 1 tumors that tend to grow slowly and rarely grow into nearby tissues. These tumors are almost always linked with an inherited condition called tuberous sclerosis.
- Diffuse astrocytomas are also slow-growing tumors, but they are grade 2 tumors that can grow into nearby tissues, which makes them hard to remove with surgery. This brain tumor infiltrates the surrounding normal brain tissue, making complete surgical removal more difficult. Though these tumors are thought of as low grade, they tend to become more aggressive and fast growing over time. A fibrillary astrocytoma may cause seizures.
- Pleomorphic xanthoastrocytomas (PXAs) are grade 2 tumors that tend to grow slowly, and most can be cured by surgery alone.
- Optic gliomas are astrocytomas that start in the optic nerves (the nerves leading from the eyes to the brain). They usually grow slowly, and are often linked with an inherited condition called neurofibromatosis type 1. These tumors are rarely fatal, but they may cause vision loss and injury to nearby brain tissue.
High-grade (grade 3 or 4) astrocytomas tend to grow quickly and spread into the surrounding normal brain tissue. These include:
- Glioblastomas or glioblastoma multiforme, which are the fastest growing type of astrocytoma (grade 4). This is the most malignant type of astrocytoma. It grows rapidly, and often causes pressure in the brain. These tumors require a combination of treatments.
- Anaplastic astrocytomas, which are grade 3. This brain tumor is malignant. Symptoms depend on the location of the tumor. These tumors require a combination of treatments.
Oligodendrogliomas
These tumors start in brain cells called oligodendrocytes (a type of glial cell that makes a fatty substance that helps nerve cells send electric signals). These are grade II tumors that tend to grow slowly, but most of them can grow into nearby brain tissue and can’t be removed completely by surgery. Oligodendrogliomas rarely spread along the CSF pathways and even less frequently spread outside the brain or spinal cord. As with astrocytomas, they can become more aggressive over time.
Only about 1% of brain tumors in children are oligodendrogliomas.
Ependymomas
About 5% of brain tumors in children are ependymomas. These tumors start in the ependymal cells that line the ventricles or central canal of the spinal cord. They can range from fairly low-grade (slow growing) tumors to grade III (fast growing) tumors, which are called anaplastic ependymomas.
Ependymomas may spread along the CSF pathways but do not spread outside the brain or spinal cord. These tumors can block the flow of CSF out of the ventricles, causing the ventricles to become very large – a condition called hydrocephalus.
Unlike astrocytomas and oligodendrogliomas, ependymomas usually do not grow into normal brain tissue. As a result, some (but not all) ependymomas can be removed and cured by surgery. But because they can spread along ependymal surfaces and CSF pathways, treating them can sometimes be difficult.
Brain stem gliomas
A brain stem glioma is any type of glioma that starts in the brain stem. This term refers to the location of the tumor, rather than the type of cell it starts in.
- A small number of brain stem gliomas occur as tumors with very distinct edges called focal brain stem gliomas.
- More often, brain stem gliomas grow diffusely throughout the brain stem (where the tumor cells are spread throughout normal tissue), rather than growing as a focal tumor (where the tumor cells are clustered together). These are referred to as diffuse midline gliomas. These tumors most often start in the pons, where they are called diffuse intrinsic pontine gliomas. These tumors can be hard to treat.
About 10% to 20% of brain tumors in children are brain stem gliomas. Nearly all of these tumors are some type of astrocytoma.
Embryonal tumors
These tumors start in early forms of nerve cells in the central nervous system. About 10% to 20% of brain tumors in children are embryonal tumors. They are more common in younger children than older ones, and are rare in adults. Embryonal tumors tend to grow quickly and often spread throughout the CSF pathways.
Medulloblastomas are the most common type of embryonal tumor. These tumors start in the cerebellum. There are several different types of medulloblastomas, based on how the tumor cells look under a microscope, and on which gene mutations the cells have. Some types of medulloblastoma tend to have a better outlook than others, and doctors are now trying to determine how this might affect treatment.
Medulloblastomas can often be treated effectively and tend to have a better outlook than embryonal tumors in other parts of the brain.
Other, less common types of embryonal tumors include:
- Medulloepithelioma
- Atypical teratoid/rhabdoid tumor (ATRT)
- Embryonal tumor with multilayered rosettes
In the past, many embryonal tumors were referred to as primitive neuroectodermal tumors (PNETs).
Pineal tumors
Some types of tumors occur in the pineal gland (a small gland in the middle of the brain). The most common (and fastest growing) of these are called pineoblastomas. These tumors can be hard to treat.
Germ cell tumors, which are described below, can also start in the pineal gland.
Craniopharyngiomas
These slow-growing tumors start above the pituitary gland but below the brain itself. They account for about 4% of brain tumors in children. These tumors may press on the pituitary gland and the hypothalamus, causing hormone problems. Because craniopharyngiomas start very close to the optic nerves, they can also cause vision problems. This makes them hard to remove completely without damaging the child’s vision or hormone balance.
Mixed glial and neuronal tumors
Certain tumors that develop in children and young adults (and rarely in older adults) have both glial and neuronal cell components. They tend to have a fairly good outlook.
- Dysembryoplastic neuroepithelial tumors (DNETs) tend to be slow growing (grade II) tumors, and most can be cured by surgery alone.
- Ganglioglioma is a type of grade I tumor that has both mature neurons and glial cells. Most can be cured by surgery alone or surgery combined with radiation therapy.
Choroid plexus tumors
These rare tumors start in the choroid plexus, the area that makes cerebrospinal fluid (CSF) within the ventricles of the brain. Most are benign (choroid plexus papillomas) and can be cured by surgery. However, some are malignant (choroid plexus carcinomas).
Schwannomas (neurilemmomas)
These tumors start in Schwann cells that surround and insulate cranial nerves and other nerves. Schwannomas are usually benign . They often form near the cerebellum on the cranial nerve responsible for hearing and balance, in which case they are called vestibular schwannomas or acoustic neuromas. They may also develop on spinal nerves, just past the point where the nerve leaves the spinal cord. When this is the case, the tumor can press on the spinal cord, causing weakness, sensory loss, and bowel and bladder problems.
These tumors are rare in children. When schwannomas are found in a child, particularly if there are tumors on both sides of the head, it often means the child has an inherited tumor syndrome such as neurofibromatosis type 2.
Other tumors that start in or near the brain
Meningiomas
These tumors begin in the meninges, the layers of tissue that surround the outer part of the brain and spinal cord. Meningiomas cause symptoms by pressing on the brain or spinal cord. They are much less common in children than in adults.
Meningiomas are almost always benign and are usually cured by surgery. Some, however, are located very close to vital structures in the brain and can’t be cured by surgery alone.
Meningiomas are often assigned a grade based on how the tumor cells look.
- Grade 1 meningiomas, which look most like normal cells, account for most meningiomas.
- Grade 2 (atypical) meningiomas look slightly more abnormal.
- Grade 3 (anaplastic or malignant) meningiomas, which look the most abnormal, make up only about 1% to 3% of meningiomas.
Higher-grade meningiomas are more likely to come back after treatment, and some grade 3 meningiomas can spread to other parts of the body.
Chordomas
These tumors start in the bone at the base of the skull or at the lower end of the spine. Chordomas don’t start in the central nervous system, but they can injure nearby parts of the brain or spinal cord by pressing on them. These tumors tend to come back if they are not removed completely, causing more damage. They usually do not spread to other organs. Chordomas are much more common in adults than in children.
Germ cell tumors
These rare tumors develop from germ cells, which normally form egg cells in women and sperm cells in men. During normal development before birth, germ cells travel to the ovaries or testicles and develop into egg or sperm cells. But sometimes some germ cells don’t move where they should and end up in abnormal locations such as the brain. They may then develop into germ cell tumors, similar to those that can form in the ovaries or testicles.
Germ cell tumors of the nervous system usually occur in children, most often in the pineal gland or above the pituitary gland. These tumors can sometimes be diagnosed without a biopsy by measuring certain chemicals in the cerebrospinal fluid (CSF) or blood.
Types of germ cell tumors include:
- Germinomas (the most common type of brain and spinal cord germ cell tumor)
- Choriocarcinomas
- Embryonal carcinomas
- Teratomas
- Yolk sac tumors (endodermal sinus tumors)
Neuroblastomas
These nerve cell tumors are the third most common cancer in children. But neuroblastomas rarely develop in the brain or spinal cord; most develop from nerve cells inside the abdomen or chest. This type of cancer is most common during early infancy.
Lymphomas
Lymphomas are cancers that start in cells called lymphocytes, which are white blood cells that are part of the immune system. Most lymphomas start in other parts of the body, but a small portion start in the central nervous system (CNS), and are called primary CNS lymphomas. These tumors are rare in children.
Pituitary tumors
Tumors that start in the pituitary gland are almost always benign (non-cancerous). But they can still cause problems if they grow large enough to press on nearby structures or if they make too much of any kind of hormone. These tumors are more common in teens than in younger children.
Cancers that spread to the brain from other parts of the body
Sometimes tumors in the brain are found to have metastasized (spread) there from some other part of the body. Tumors that start in other organs and then spread to the brain are called metastatic or secondary brain tumors (as opposed to primary brain tumors, which start in the brain). This is important because metastatic and primary brain tumors are often treated differently.
In children, metastatic brain tumors are much less common than primary brain tumors. Childhood leukemias can sometimes spread to the CSF around the brain and spinal cord. When this happens, the cancer is still considered a leukemia (the cancer cells in the CSF are leukemia cells), so doctors use treatments directed at the leukemia.
Brain tumor in children causes
The cause of primary brain tumors in kids is usually unknown. Only a few risk factors for brain tumors are known for sure.
- Genetic conditions: Children with some genetic syndromes are more likely to develop brain tumors than other children. The syndromes are neurofibromatosis, von Hippel-Lindau disease, Li-Fraumeni syndrome, ataxia telangiectasia, basal cell nevus syndrome and hereditary non-polyposis colon cancer (Gorlin syndrome). Children with these genetic conditions are more at risk for brain tumors, but these account for only a small fraction of cases. These syndromes are usually recognized early in childhood, so it is most likely that you would know if your child has one of these conditions.
- Prior radiation: Children who have received radiation therapy to the head as part of treatment for an earlier cancer are at an increased risk for a new brain tumor.
- Sex Male/Female: The patterns differ depending on the type of brain tumor. Boys and girls are equally likely to develop an astrocytoma. Boys are more likely to develop a medulloblastoma, ependymoma or germ cell tumor than girls.
- Race and Ethnicity: Caucasian children are more likely than African American children to develop a medulloblastoma or ependymoma. Other types of brain tumors affect Caucasian and African American children equally. Differences in other ethnic groups have not yet been identified.
According to the current state of medical knowledge, the following exposures have NOT been shown to increase a child’s risk of developing a brain tumor:
- Electromagnetic fields such as those from power lines and electric appliances (such as televisions)
- Mother’s consumption of alcohol during pregnancy
- Mother’s smoking during pregnancy
Risk factors for brain tumors in children
A risk factor is anything that affects a person’s chance of getting a disease such as a brain or spinal cord tumor. Different types of cancer have different risk factors.
Radiation exposure
The only well-established environmental risk factor for brain tumors is radiation exposure to the head, which most often comes from the treatment of other conditions.
For example, before the risks of radiation were well known (more than 50 years ago), children with ringworm of the scalp (a fungal infection) often received low-dose radiation therapy. This was later found to increase their risk of some types of brain tumors as they got older.
Today, most radiation-induced brain tumors are caused by radiation given to the head to treat other cancers, such as leukemia. These brain tumors usually develop around 10 to 15 years after getting radiation therapy.
Radiation-induced tumors are still fairly rare, but because of the increased risk (as well as the other possible side effects), radiation therapy is only given to the head after carefully weighing the possible benefits and risks. For most patients with cancer in or near the brain, the benefits of getting radiation therapy as part of their treatment far outweigh the small risk of developing a brain tumor years later.
The possible risk from fetal or childhood exposure to imaging tests that use radiation, such as x-rays or CT scans, is not known for sure. These tests use much lower levels of radiation than those used in radiation treatments, so if there is any increase in risk, it is likely to be very small. But to be safe, most doctors recommend that pregnant women and children not get these tests unless they are absolutely needed.
Inherited and genetic conditions
Rarely, children have inherited abnormal genes from a parent that put them at increased risk for certain types of brain tumors. In other cases, these abnormal genes are not inherited but occur as a result of changes (mutations) in the gene before birth.
People with inherited tumor syndromes often have many tumors that start when they are young. Some of the better known syndromes include:
- Neurofibromatosis type 1 (von Recklinghausen disease): This is the most common syndrome linked to brain or spinal cord tumors. It is often inherited from a parent, but it can also start in some children whose parents don’t have it. Children with this syndrome may have optic gliomas or other gliomas of the brain or spinal cord, or neurofibromas (benign tumors of peripheral nerves). Changes in the NF1 gene cause this disorder.
- Neurofibromatosis type 2: This condition is less common than von Recklinghausen disease. It can also either be inherited or may start in children without a family history. It is associated with cranial or spinal nerve schwannomas, especially vestibular schwannomas (acoustic neuromas), which almost always occur on both sides of the head. It is also linked to an increased risk of meningiomas, as well as spinal cord gliomas or ependymomas. Changes in the NF2 gene are nearly always responsible for neurofibromatosis type 2.
- Tuberous sclerosis: Children with this condition may develop subependymal giant cell astrocytomas (SEGAs), as well as other benign tumors of the brain, skin, heart, kidneys, or other organs. This condition is caused by changes in either the TSC1 or the TSC2 gene.
- Von Hippel-Lindau disease: Children with this disease tend to develop blood vessel tumors (hemangioblastomas) of the cerebellum, spinal cord, or retina, as well as tumors in the kidney, pancreas, and some other parts of the body. It is caused by changes in the VHL gene.
- Li-Fraumeni syndrome: People with this syndrome have an increased risk of gliomas, as well as breast cancer, soft tissue sarcomas, leukemia, and some other types of cancer. It is caused by changes in the TP53 gene.
Other syndromes
Other inherited conditions linked with increased risks of certain types of brain and spinal cord tumors include:
- Gorlin syndrome (basal cell nevus syndrome)
- Turcot syndrome
- Cowden syndrome
- Hereditary retinoblastoma
- Rubinstein-Taybi syndrome
Some families may have genetic disorders that are not well recognized or that could even be unique to a particular family.
Factors with uncertain, controversial, or unproven effects on brain tumor risk
Cell phone use
Cell phones give off radiofrequency (RF) rays, a form of electromagnetic energy on the spectrum between FM radio waves and those used in microwave ovens, radar, and satellite stations. Cell phones do not give off ionizing radiation, the type that can cause cancer by damaging the DNA inside cells. Still, there have been concerns that the phones, whose antennae are built-in and therefore are placed close to the head when being used, might somehow raise the risk of brain tumors.
Some studies have suggested a possible increased risk of brain tumors or of vestibular schwannomas (acoustic neuromas) in adults with cell phone use, but most of the larger studies done so far have not found an increased risk, either overall or among specific types of tumors. Still, there are very few studies of long-term use (10 years or more), and cell phones haven’t been around long enough to determine the possible risks of lifetime use. The same is true of any possible higher risks in children, who are increasingly using cell phones. Cell phone technology also continues to change, and it’s not clear how this might affect any risk.
These risks are being studied, but it will likely be many years before firm conclusions can be made. In the meantime, for people concerned about the possible risks, there are ways to lower their (and their children’s) exposure, such as using the phone’s speaker or an earpiece to move the phone itself away from the head when used.
Other factors
Exposure to aspartame (a sugar substitute), exposure to electromagnetic fields from power lines and other sources, and infection with certain viruses have been suggested as possible risk factors, but most researchers agree that there is no convincing evidence to link these factors to brain tumors. Research on these and other potential risk factors continues.
Brain tumor symptoms in children
When a child develops a brain tumor, early diagnosis is essential. The skull does not have excess room for anything other than the brain. Therefore, as brain tumors develop and expand, they cause extra pressure in this closed space. This is called intracranial pressure (ICP). Increased intracranial pressure is caused by extra tissue in the brain as well as blockage of the cerebrospinal fluid (CSF) flow pathways.
Typical symptoms of brain tumors are directly related to the location of the tumor, how fast it is growing and any associated tissue swelling that occurs in conjunction with the tumor. Parents often are the first to notice symptoms related to the development of a brain tumor. Occasionally, the child’s teacher or physician may note signs and symptoms that are worrisome.
The most common signs and symptoms that could point to a potential brain tumor are:
- Headaches: Many children with a brain tumor experience headaches before their diagnosis. Headaches that is frequent and recurrent, especially after waking up in the morning. But a lot of children have headaches, and most of them don’t have a brain tumor. One red flag to watch out for: a headache that’s worse in the morning. This is partly because pressure in the brain increases when you’re lying down, and a tumor can make that worse.
- Nausea and vomiting: Vomiting, especially in the morning. Nausea and vomiting are two common signs of the flu or flulike illnesses. However, in rare instances, these symptoms can be due to a brain tumor causing increased pressure inside the brain. If these symptoms persist or coincide with a headache, ask your child’s pediatrician for an expert medical opinion.
- Sleepiness: A sleepy child isn’t usually cause for alarm. But pay attention to your gut instinct. If your child is acting lethargic, or extra sleepy, for no apparent reason, call your doctor for guidance on whether further evaluation may be necessary.
- Vision, hearing or speech changes: Depending on a brain tumor’s location, it can affect vision, hearing and speech. Eye movement problems and/or vision changes. Of course, many children have challenges in these areas that have nothing to do with a brain tumor. Still, sudden changes in how your child sees, hears or talks should be evaluated by a medical professional.
- Personality changes: Personality changes can be a completely normal (if frustrating) part of parenting. In rare cases, they can be due to a brain tumor that’s affecting the cerebral cortex. If your child’s mood swings or personality changes seem sudden or severe, tell your child’s pediatrician.
- Balance problems: If a tumor sits near the brain stem, it can cause balance problems. Tumbles and falls are a regular part of life for most toddlers. But severe or worsening balance problems in young children warrant a call to your doctor. If your older child suddenly has a hard time keeping his or her balance, a doctor can help you determine why.
- Seizures: When a brain tumor sits on the surface of the brain, it can cause seizures. Many actions can trigger a seizure, including laughing. If your child is experiencing seizures, you should see a doctor. The cause may be a tumor or something else, but seizures must always be evaluated.
- Increased head size (macroencephaly): When babies are young, their skull bones haven’t fused or grown together yet. Because these bones are still malleable, a brain tumor could cause their head to grow in abnormal ways. If you notice a bulging on one side or any other severe changes to your baby’s head shape, your doctor can help you decide whether it requires further evaluation.
Less common symptoms include:
- Changes in eating or thirst
- Growth problems
- Dizziness
- Lethargy, irritability or other behavior changes
- Deterioration in school performance
- Loss of sensation in the arms or legs
- Loss of consciousness, without history of injury
- Changes in, or loss of control of, bowel or bladder
- Hearing loss, without evidence of infection
- Coma and death, if left untreated
Brain tissue dysfunction caused by a growing tumor may cause other symptoms, depending on the tumor’s location. For example, if a brain tumor is located in the cerebellum at the back of the head, a child may have trouble with movement, walking, balance and coordination. If the tumor affects the optic pathway, which is responsible for sight, the child may experience vision changes.
Many of these symptoms can be caused by common health conditions and that’s most often the case. However, if you’re concerned about one or more of these symptoms in your child, seek out the medical opinion of a health professional you trust. Often, an MRI scan can determine whether a brain abnormality is causing the symptoms.
If your child does have a brain tumor, advanced pediatric neurosurgery can offer effective treatment and a successful recovery for the majority of young patients who have this rare condition.
Symptoms of tumors in different parts of the brain or spinal cord
Tumors in different parts of the brain or spinal cord can cause different symptoms. But these symptoms can be caused by any abnormality in that particular location – they don’t always mean a child has a brain or spinal cord tumor.
- Tumors in the parts of the cerebrum (the large, outer part of the brain) that control movement or sensation can cause weakness or numbness in a part of the body, often on just one side.
- Tumors in or near the parts of the cerebrum responsible for language can cause problems with speech or even understanding words.
- Tumors in the front part of the cerebrum can sometimes affect thinking, personality, and language skills.
- Tumors in the cerebellum (the lower, back part of the brain that controls coordination) can cause trouble walking, trouble with precise movements of hands, arms, feet, and legs, problems swallowing or synchronizing eye movements, and changes in speech rhythm.
- Tumors in the back part of the cerebrum, or around the pituitary gland, the optic nerves, or certain other cranial nerves can cause vision problems.
- Tumors in or near other cranial nerves might lead to hearing loss (in one or both ears), balance problems, weakness of some facial muscles, facial numbness or pain, or trouble swallowing.
- Spinal cord tumors may cause numbness, weakness, or lack of coordination in the arms and/or legs (usually on both sides of the body), as well as bladder or bowel problems.
Having one or more of the symptoms above does not necessarily mean that your child has a brain or spinal cord tumor. All of these symptoms can have other causes. Still, if your child has any of these symptoms, especially if they don’t go away or get worse over time, see your child’s doctor so that the cause can be found and treated, if needed.
Brain tumor in children diagnosis
A child experiencing brain tumor symptoms should be thoroughly evaluated by a pediatrician or pediatric neurologist (a doctor specializing in medical treatment of nervous system diseases) or a neurosurgeon (a surgeon specializing in nervous system diseases), or in the emergency room to find the source of the problem.
The doctor’s evaluation usually includes imaging of the brain by an MRI scan. If the scan shows a brain tumor, the next step is a neurosurgical consultation. The pediatric neurosurgeon will work with the whole family to develop the best treatment plan for the child.
Other specialists may join the child’s treatment team, such as a pediatric oncologist (childhood cancer specialist), an ophthalmologist (if the child’s tumor affects the vision pathways), an epileptologist (to address seizures), a radiation oncologist, and advanced practitioners and technologists.
Imaging tests
Your child’s doctors may order one or more imaging tests. These tests use x-rays, strong magnets, or radioactive substances to create pictures of internal organs such as the brain and spinal cord. The pictures may be looked at by doctors specializing in this field (neurosurgeons, neurologists, and neuroradiologists) as well as by your child’s primary care doctor.
Magnetic resonance imaging (MRI) and computed tomography (CT) scans are used most often for brain diseases. These scans will almost always show a brain or spinal cord tumor, if one is present. Doctors can often also get an idea about what type of tumor it might be, based on how it looks on the scan and where it is in the brain (or spinal cord).
Magnetic resonance imaging (MRI) scan
MRI scans are very good for looking at the brain and spinal cord and are considered the best way to look for tumors in these areas. MRI images are usually more detailed than those from CT scans (described below). But they don’t show the bones of the skull as well as CT scans and therefore might not show the effects of tumors on the skull.
MRI scans use radio waves and strong magnets (instead of x-rays) to make pictures, so they don’t expose the child to radiation. A contrast material called gadolinium may be injected into a vein before the scan to help see details better.
MRI scans can take a long time, and require a person to stay still for several minutes at a time. Some children might need medicine to help them relax or even go to sleep during the test.
Special types of MRI can be useful in some situations:
- Magnetic resonance angiography (MRA) and magnetic resonance venography (MRV): These special forms of MRI may be done to look at the blood vessels in the brain, especially in and around a tumor. This can be very useful before surgery to help the surgeon plan an operation.
- Magnetic resonance spectroscopy (MRS): This test can be done as part of an MRI. It measures biochemical changes in an area of the brain (which are displayed in graph-like results called spectra). By comparing the results from a tumor to that of normal brain tissue, it can sometimes help determine the type of tumor (or how quickly it is likely to grow), although a biopsy of the tumor is often still needed to get an accurate diagnosis. MRS can also be used after treatment if another test shows an area still looks abnormal. The MRS can help determine if the area is remaining tumor or if it is more likely to be scar tissue.
- Magnetic resonance perfusion (perfusion MRI): For this test, a contrast dye is injected quickly into a vein. Then this type of MRI can show the amount of blood going through different parts of the brain and tumor. Tumors often have a bigger blood supply than normal areas of the brain. A faster growing tumor may need more blood. Perfusion MRI can give doctors an idea of the best place to take a biopsy. It can also be used after treatment to help determine if an area that still looks abnormal is remaining tumor or if it is more likely to be scar tissue.
- Functional MRI (fMRI): This test looks for tiny blood flow changes in an active part of the brain. It can be used to determine what part of the brain handles a function such as speech, thought, sensation, or movement. Doctors can use this to help determine which parts of the brain to avoid when planning surgery or radiation therapy. This test is like a regular MRI, except that your child will be asked to do certain tasks (like answering simple questions or moving their fingers) to activate different areas of the brain while the scans are being done.
- Diffusion tensor imaging (DTI), also known as tractography: This is a type of MRI test that can show the major pathways (tracts) of white matter in the brain. This information can be used by surgeons to help avoid these important parts of the brain when removing tumors.
Computed tomography (CT) scan
The CT scan uses x-rays to make detailed cross-sectional images of your child’s brain and spinal cord. Unlike a regular x-ray, a CT scan creates detailed images of the soft tissues in the body.
For brain and spinal cord tumors, CT scans are not used as often as MRI scans, which give slightly more detailed images and do not use radiation. Still, there are instances where CT scans may have advantages over MRI scans:
- CT scans take much less time than MRIs, which can be particularly helpful for children who have trouble staying still.
- CT scans provide greater detail of the bone structures near the tumor than MRIs do.
- CT angiography (CTA), described below, can provide better details of the blood vessels in and around a tumor than MRA in some cases.
Before the scan, your child may get an injection of a contrast dye through an IV (intravenous) line. This helps better outline any tumors that are present.
- CT angiography (CTA): For this test, your child gets an injection of contrast material through an IV line while he or she is in the CT scanner. The scan creates detailed images of the blood vessels in the brain, which can help doctors plan surgery.
Positron emission tomography (PET) scan
For a PET scan, a radioactive substance (usually a type of sugar known as FDG) is injected into the blood. The amount of radioactivity used is very low and passes out of the body within a day or so. Because tumor cells in the body are growing quickly, they absorb larger amounts of the sugar than most other cells. A special camera is then used to create a picture of areas of radioactivity in the body. Some children might need medicine to help them relax or even go to sleep during the test.
The PET scan image is not as detailed as a CT or MRI scan, but it can provide helpful information about whether abnormal areas seen on other tests (such as MRIs) are likely to be tumors or not. This test is more likely to be helpful for fast-growing (high-grade tumors) than for slower-growing tumors.
This test is also useful after treatment to help determine if an area that still looks abnormal on an MRI scan is remaining tumor or if it is more likely to be scar tissue. Remaining tumor might show up on the PET scan, while scar tissue will not.
Brain or spinal cord tumor biopsy
Imaging tests such as MRI and CT scans may show that a child has a brain or spinal cord tumor. But often the type of tumor can only be determined by removing a sample of it, which is called a biopsy. A biopsy may be done as a procedure on its own for diagnosis, or it may be part of surgery to treat the tumor.
In some cases (such as for many astrocytomas or brain stem gliomas), it may not be necessary or possible to biopsy the tumor safely, so the diagnosis is made based only on how the tumor looks on imaging tests.
Biopsies can be done in different ways.
Stereotactic needle biopsy
This type of biopsy may be used if imaging tests show surgery to remove the tumor might be too risky (such as with some tumors in vital areas or deep within the brain), but a sample is still needed to make a diagnosis.
Depending on the situation, the biopsy may be done with the child awake or under general anesthesia (asleep). If the child is awake, the neurosurgeon injects a local anesthetic into areas of skin over the skull to numb them. (The skull and brain itself do not feel pain.)
The biopsy itself can be done in 2 main ways:
- The most common approach is to get an MRI or CT scan, and then use either markers (each about the size of a nickel) placed on different parts of the scalp, or facial and scalp contours, to create a map of the inside of the head. An incision (cut) is then made in the scalp, and a small hole is drilled in the skull. An image-guidance system is then used to direct a hollow needle into the tumor to remove small pieces of tissue.
- In an approach that’s used less often, a rigid frame is attached to the head. An MRI or CT scan is used along with the frame to help the neurosurgeon guide a hollow needle into the tumor to remove small pieces of tissue. This also requires an incision in the scalp and a small hole in the skull.
The biopsy samples are then sent to a pathologist (a doctor specializing in diagnosis of diseases by lab tests). The pathologist looks at it under a microscope (and might do other lab tests) to determine if the tumor is benign or malignant (cancerous) and exactly what type of tumor it is. This helps determine the best course of treatment and the prognosis (outlook).
Craniotomy (surgical or open biopsy)
If imaging tests show the tumor can likely be treated with surgery, the neurosurgeon may not do a needle biopsy. Instead, he or she may do an operation called a craniotomy to remove all or most of the tumor. Removing most of the tumor is known as debulking.
Small samples of the tumor are looked at right away by the pathologist while the child is still in the operating room, to get a preliminary diagnosis. This can help guide treatment, including whether further surgery should be done at that time. A final diagnosis is made a within a few days in most cases.
Lab tests of biopsy specimens
Finding out which type of tumor a child has is very important in helping to determine their outlook (prognosis) and treatment options. But in recent years, doctors have found that changes in certain genes, chromosomes, or proteins within the tumor cells can also be important. Some tumors are now tested for these types of changes. For example:
- Gliomas that are found to have IDH1 or IDH2 gene mutations tend to have a better outlook than gliomas without these gene mutations.
- Oligodendrogliomas whose cells are missing parts of certain chromosomes (known as a 1p19q co-deletion) are much more likely to be helped by chemotherapy than patients whose tumors do not.
- In high-grade gliomas, MGMT promoter methylation is linked with better outcomes and a higher chance of responding to chemotherapy, so it can sometimes be used to help guide treatment.
- For medulloblastomas, changes in certain genes can be used to divide these tumors into groups, some of which have a better prognosis (outlook) than others.
Lumbar puncture (spinal tap)
This test is used mainly to look for signs of cancer in the cerebrospinal fluid (CSF), which is the liquid that bathes the brain and spinal cord. For this test, the doctor first numbs an area in the lower part of the back over the spine. The doctor may also recommend that the child be given something to make them sleep so the lumbar puncture can be done more easily and safely. A small, hollow needle is then placed between the bones of the spine to withdraw some of the fluid.
The fluid is looked at under a microscope for cancer cells. The CSF can also be tested for certain substances released by some germ cell tumors.
Lumbar punctures are often used if a tumor has already been diagnosed as a type that can commonly spread through the CSF (such as a medulloblastoma). Information from the spinal tap can influence treatment.
Bone marrow aspiration and biopsy
Because some tumors (especially medulloblastomas) can spread beyond the nervous system, in some instances the doctor may recommend looking at cells in your child’s bone marrow (the soft, inner part of certain bones) to see if tumor cells have spread there.
The bone marrow aspiration and biopsy are often done at the same time. The samples are usually taken from the back of the pelvic (hip) bone, but in some cases they may be taken from other bones.
For a bone marrow aspiration, the skin over the hip and the surface of the bone is cleaned and then numbed with local anesthetic. In most cases, the child is also given other medicines to make them drowsy or even asleep during the procedure. A thin, hollow needle is then inserted into the bone, and a syringe is used to suck out (aspirate) a small amount of liquid bone marrow.
A bone marrow biopsy is usually done just after the aspiration. A small piece of bone and marrow is removed with a slightly larger needle that is pushed down into the bone. Once the biopsy is done, pressure is applied to the site to help stop any bleeding.
The specimens are then looked at under a microscope for tumor cells.
Blood and urine tests
These lab tests are rarely used to diagnose brain and spinal cord tumors, but if your child has been sick for some time they may be done to check how well the liver, kidneys, and some other organs are working. This is especially important before any planned surgery.
If your child is getting chemotherapy, blood tests will be done routinely to check blood counts and to see if the treatment is affecting other parts of the body.
Brain tumor in children treatment
In putting together the most appropriate treatment plan for a child with a brain tumor, the neurosurgery team will need to know:
- Tumor location: This is determined by a brain scan, using one or more types of imaging such as CT or MRI. Because there are many vital structures in the brain, there are places a tumor can grow that are not appropriate for surgery. The neurosurgeon’s careful evaluation will determine the accessibility of the tumor and the safest approach.
- Brain tumor type: Looking at the tumor cells under a microscope can reveal the brain tumor type, and give doctors insight on how the tumor is likely to grow or spread.
- Brain tumor grade: The grade refers to how aggressive the tumor cells appear to be. The higher the grade, the more aggressive the tumor.
Treatment for childhood brain cancer may involve:
- Surgery
- Chemotherapy
- Radiotherapy
- Steroids may also be given to decrease the swelling caused by the tumor.
Your child may undergo some or all of these treatments, depending on their tumor type and grade, your child’s age, overall health and medical history, and your family preferences.
Types of doctors who help care for children with cancer:
- Pediatric oncologist: A doctor who specializes in cancers of children. (Pediatric means dealing with the health of children. Oncology means cancer.) They generally are board-certified, which means they’ve passed written national exams. They plan and direct cancer treatment. In a teaching hospital they serve as the doctor in charge. There might be more than one on the team, in which case they might rotate or switch places from one day to the next. They often work closely with physician assistants (PAs) and nurse practitioners (discussed in the next section).
- Pediatric hematologist: A doctor who specializes in diseases of the blood and blood-forming tissues of children (Hematology means blood disease.)
- Pediatric hematology or oncology fellow: A pediatrician training to become a hematologist or oncologist
- Pediatric resident: A doctor training to become a pediatrician. They are in teaching hospitals, usually spending a certain length of time on the hematology or oncology service
- Medical students: Although not yet doctors, third and fourth year medical students in teaching hospitals are assigned monthly rotations on the hematology or oncology services and help care for patients
- Radiologist: A doctor with special training in diagnosing diseases by reading x-rays and other types of imaging studies, like CT scans and MRIs
- Pediatric surgeon: A doctor who treats medical problems in children with surgery. Some surgeons specialize in different parts of the body. For example, thoracic surgeons operate on the chest.
- Neurosurgeon: A doctor who specializes in operations on the brain, spine, or other parts of the nervous system
- Neurologist: A doctor who treats problems of the nervous system
- Orthopedic surgeon: A surgeon who specializes in diseases and injuries of the bones
- Pathologist: A doctor who specializes in diagnosing and classifying diseases by lab tests, such as looking at tissue and cells under a microscope. The pathologist decides if a tumor is cancer, and, if it is, the exact cell type.
- Psychiatrist: A medical doctor who specializes in mental health and behavioral disorders. Psychiatrists prescribe medicines and can also provide counseling.
- Endocrinologist: A doctor who specializes in diseases related to the glands of the endocrine system, such as the thyroid, pancreas, and adrenal glands
- Gynecologist: A doctor who specializes in women’s health and the female reproductive system
- Anesthesiologist: A doctor who specializes in giving medicines or other agents that prevent or relieve pain, especially during surgery
Other doctors in the medical center and its clinics may play a part in caring for children and teens with cancer, depending on the diagnosis, treatment plan, or symptoms that develop during the course of treatment. All work closely with the basic cancer care team to coordinate care.
Surgery
Most brain tumors in infants and children require surgical removal, or at least a biopsy, as part of the treatment. The surgeon may recommend surgery to remove as much of the tumor as safely possible as a first step and to relieve intracranial pressure caused by the tumor. For low-grade or slow-growing tumors, surgery may be the only intervention necessary.
Follow-up care after surgery
The recovery process is different for each child. Children who received prompt diagnosis and treatment can do well after surgery.
Some pediatric patients may experience some temporary neurological deficits, such as muscle weakness. In most cases, this goes away shortly after surgery, unless there was substantial permanent damage before the child was diagnosed. Physical, occupational and speech therapy can help improve strength, function and speed of recovery.
Regular post-operative follow-up visits with the child’s neurosurgeon are also important to monitor neurological function and side effects from treatment, and to guard against recurrence of the tumor.
Radiation Therapy
This therapy focuses beams of high-energy radiation on the tumor tissue and a small amount of surrounding tissue. Some tumors, such as medulloblastoma, require additional radiation to the entire brain and spinal cord. Radiation is used very cautiously in infants and toddlers due to their growing brains.
Chemotherapy
Chemotherapy is used for many types of brain tumors including aggressive, high-grade tumors. Chemotherapy can be administered as pills (orally), intravenously (IV, by vein), injected directly into the cerebrospinal fluid, or injected directly into the cavity left after surgical removal of a brain tumor.
Brain tumor in children survival prognosis
How well a child does depends on many things, including the type of tumor. In general, about 3 out of 4 children survive at least 5 years after being diagnosed.
Long-term brain and nervous system problems may result from the tumor itself or from treatment. Children may have problems with attention, focus, or memory. They may also have problems processing information, planning, insight, or initiative or desire to do things.
Children younger than age 7, especially younger than age 3, seem to be at greatest risk of these complications.
Parents need to make sure that children receive support services at home and at school.
Brain tumor in children survival rates
Survival rates are a way to get a general idea of the outlook (prognosis) for people with a certain type of tumor. They tell you what portion of people with the same type of tumor are still alive a certain amount of time (usually 5 years) after they were diagnosed. They can’t tell you what will happen, but they may help give you a better understanding about how likely it is that treatment will be successful. Some people will want to know about survival rates, and some people won’t. If you don’t want to know, you don’t have to.
The 5-year survival rate is the percentage of children who live at least 5 years after their cancer is diagnosed. For example, a 5-year survival rate of 80% means that an estimated 80 out of 100 children who have that type of tumor are still alive 5 years after being diagnosed. Of course, many children live much longer than 5 years (and many are cured).
Survival rates don’t tell the whole story. Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they can’t predict what will happen in any child’s case. There are some limitations to keep in mind:
- The numbers below are among the most current available. But to get 5-year survival rates, doctors have to look at children who were treated at least 5 years ago. As treatments improve over time, children who are now being diagnosed with brain or spinal cord tumors may have a better outlook than these statistics show.
- The outlook for children with brain or spinal cord tumors varies by the type of tumor. But many other factors can also affect a child’s outlook, such as their age, the location and size of the tumor, and how well the tumor responds to treatment. The outlook for each child is specific to their circumstances.
Your child’s doctor can tell you how the survival rates below may apply, as he or she is familiar with your child’s situation.
The numbers below come from the Central Brain Tumor Registry of the United States 1) and are based on children aged 14 or younger who were treated between 2000 and 2014. There are some important points to note about these numbers:
- These numbers are for some of the more common types of tumors. Numbers are not readily available for all types of tumors that occur in children, often because they are rare or are hard to classify.
- In some cases, the numbers include a wide range of different types of tumors that can have different outlooks. For example, the survival rate for embryonal tumors below includes medulloblastomas, as well as other types of tumors. Medulloblastomas tend to have a better outlook than the other embryonal tumors. Therefore the actual survival rate for medulloblastomas would be expected to be higher than the number below, while the number for other embryonal tumors would likely be lower.
Table 1. Survival rates for more common brain and spinal cord tumors in children
| Type of Tumor | 5-Year Survival Rate |
| Pilocytic astrocytoma | About 95% |
| Diffuse astrocytoma | About 80% to 85% |
| Anaplastic astrocytoma | About 25% |
| Glioblastoma | About 20% |
| Oligodendroglioma | About 90% |
| Ependymoma/anaplastic ependymoma | About 75% |
| Embryonal tumors (includes medulloblastoma) | About 60% to 65% |
Footnotes: Remember, these survival rates are only estimates – they can’t predict what will happen with any child. We understand that these statistics can be confusing and may lead you to have more questions. Talk to your child’s doctor to better understand your specific situation.
[Source 2) ]References [ + ]





{kind=link}