Contents
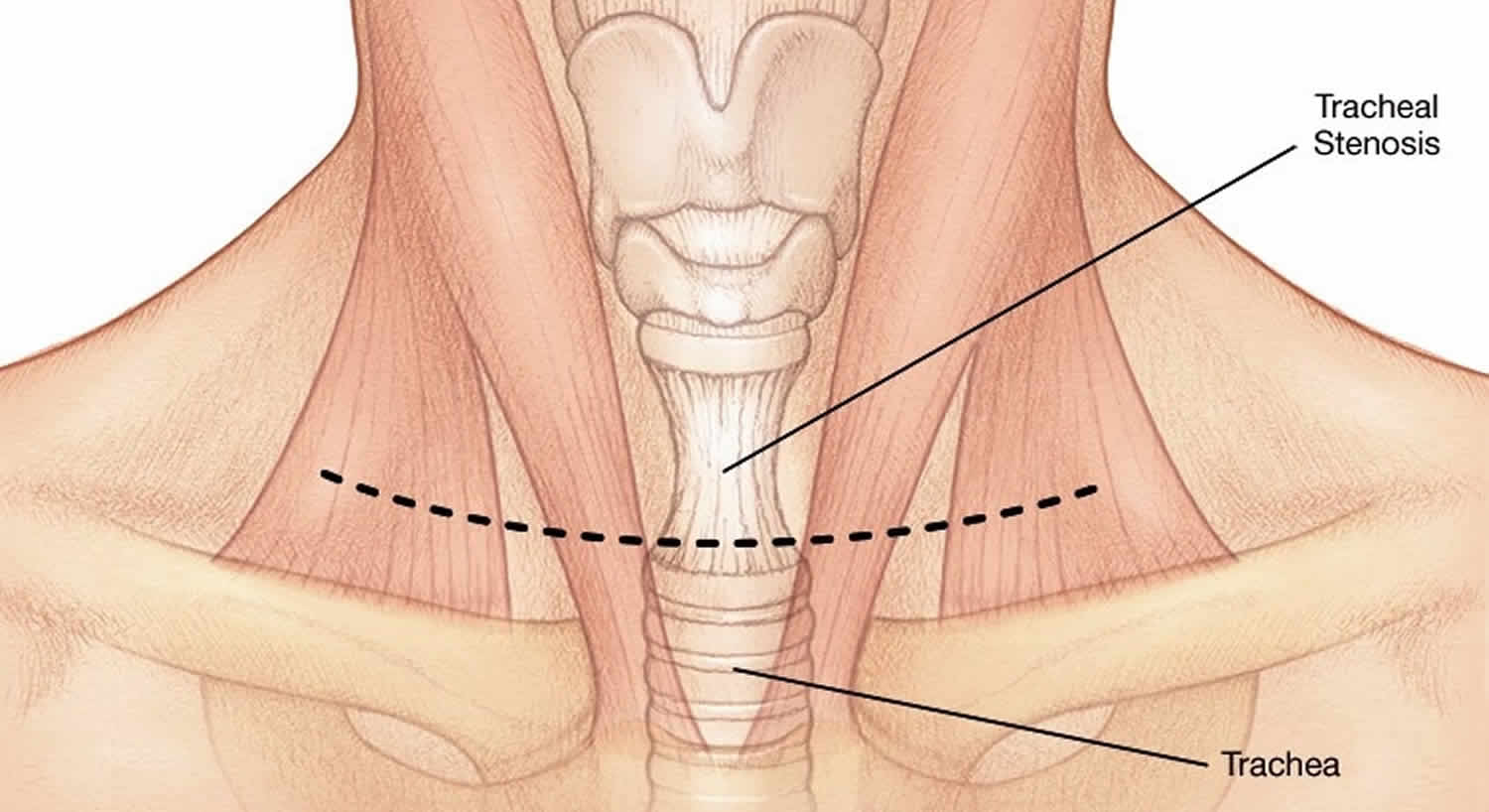
Tracheal stenosis
Tracheal stenosis is a narrowing or constriction of the cartilage that supports the windpipe (trachea) causing shortness of breath, cough, wheezing, and stridor. Tracheal stenosis can be present at birth (congenital) or caused by an injury. The most common cause of tracheal stenosis is prolonged intubation or tracheostomy, when a tube is used to assist with breathing via a mechanical ventilator. Tracheal stenosis can also be caused by inflammatory or immunologic diseases. Another cause is idiopathic tracheal stenosis, which occurs mostly in women for unknown reasons.
Congenital tracheal stenosis is often identified by characteristic wheezes and cyanosis in childhood, but asymptomatic progression to adulthood is rare 1). Patients characteristically present with stridor, complaints of dyspnea (shortness of breath), and trouble phonating, which lead to significant respiratory morbidity and may progress to acute airway compromise if not properly managed 2).
Congenital tracheal stenosis can be a result of:
- Complete tracheal rings: One or more rings of the cartilage that supports the trachea appear as O-shaped (instead of C-shaped) and constrict the airway.
- A tracheal cartilaginous sleeve: The cartilage in trachea forms a sleeve instead of independent rings. This malformation is makes it easy for the airway to become blocked.
Many patients require a more definitive surgical procedure called a tracheal resection and reconstruction. The goal of this operation is to remove the abnormal segment of trachea and to re-connect the two remaining ends together, allowing the patient to breathe comfortably again. Most commonly, this operation can be done through a neck incision that is well-tolerated. The operation is effective in resolving the problem in approximately 95% of patients, and it requires an approximately 5 day hospital stay.
What is the trachea
The principal organs of the respiratory system are the nose, pharynx, larynx, trachea, bronchi, and lungs (Figure 1). The airway from the nose through the larynx is often called the upper respiratory tract (that is, the respiratory organs in the head and neck), and the regions from the trachea through the lungs compose the lower respiratory tract (the respiratory organs of the thorax). During normal breathing, the airway is open and air passes freely through the nasal cavities (or oral cavity), pharynx, larynx, and trachea.
The trachea or “windpipe,” is a rigid tube about 12 cm (4.5 in.) long and 2.5 cm (1 in.) in diameter, that lies in front of the esophagus (Figure 1 and 2). The trachea is supported by 16 to 20 C-shaped rings of hyaline cartilage. The trachea is named for the corrugated texture imparted by these rings; you should be able to feel a few of these between your larynx and sternum. Like the wire spiral in a vacuum cleaner hose, the cartilage rings reinforce the trachea and keep it from collapsing when you inhale. The open part of the C faces posteriorly, where it is spanned by a smooth muscle, the trachealis (Figure 3). The gap in the C allows room for the esophagus to expand as swallowed food passes by. The trachealis muscles contract or relax to adjust airflow.
The lumen of the esophagus is normally closed because, unlike the airway, it has no skeletal support structures to hold it open. When the oral cavity is full of liquid or food, the soft palate is swung down (depressed) to close the oropharyngeal isthmus, thereby allowing manipulation of food and fluid in the oral cavity while breathing. When swallowing, the soft palate and parts of the larynx act as valves to ensure proper movement of food from the oral cavity into the esophagus. The soft palate elevates to open the oropharyngeal isthmus while at the same time sealing off the nasal part of the pharynx from the oral part. This prevents food and fluid from moving upward into the nasopharynx and nasal cavities. The epiglottis of the larynx closes the laryngeal inlet and much of the laryngeal cavity becomes occluded by opposition of the vocal folds and soft tissue folds superior to them. In addition, the larynx is pulled up and forward to facilitate the moving of food and fluid over and around the closed larynx and into the esophagus.
The neck contains the seven cervical vertebrae and associated muscles, parts of the alimentary and respiratory tracts and the thyroid gland. In the midline immediately anterior to the vertebrae is the pharynx, which continues as the cervical oesophagus (Figure 2). Anterior to these are the larynx and upper trachea with the thyroid gland. On each side of the organs, major vessels pass between the thorax and the head, accompanied by nerves and lymphatics.
The butterfly-shaped thyroid gland is located just inferior to the larynx (voice box). It is composed of right and left lateral lobes, one on either side of the trachea, that are connected by an isthmus anterior to the trachea (Figure 3).
Figure 1. Trachea
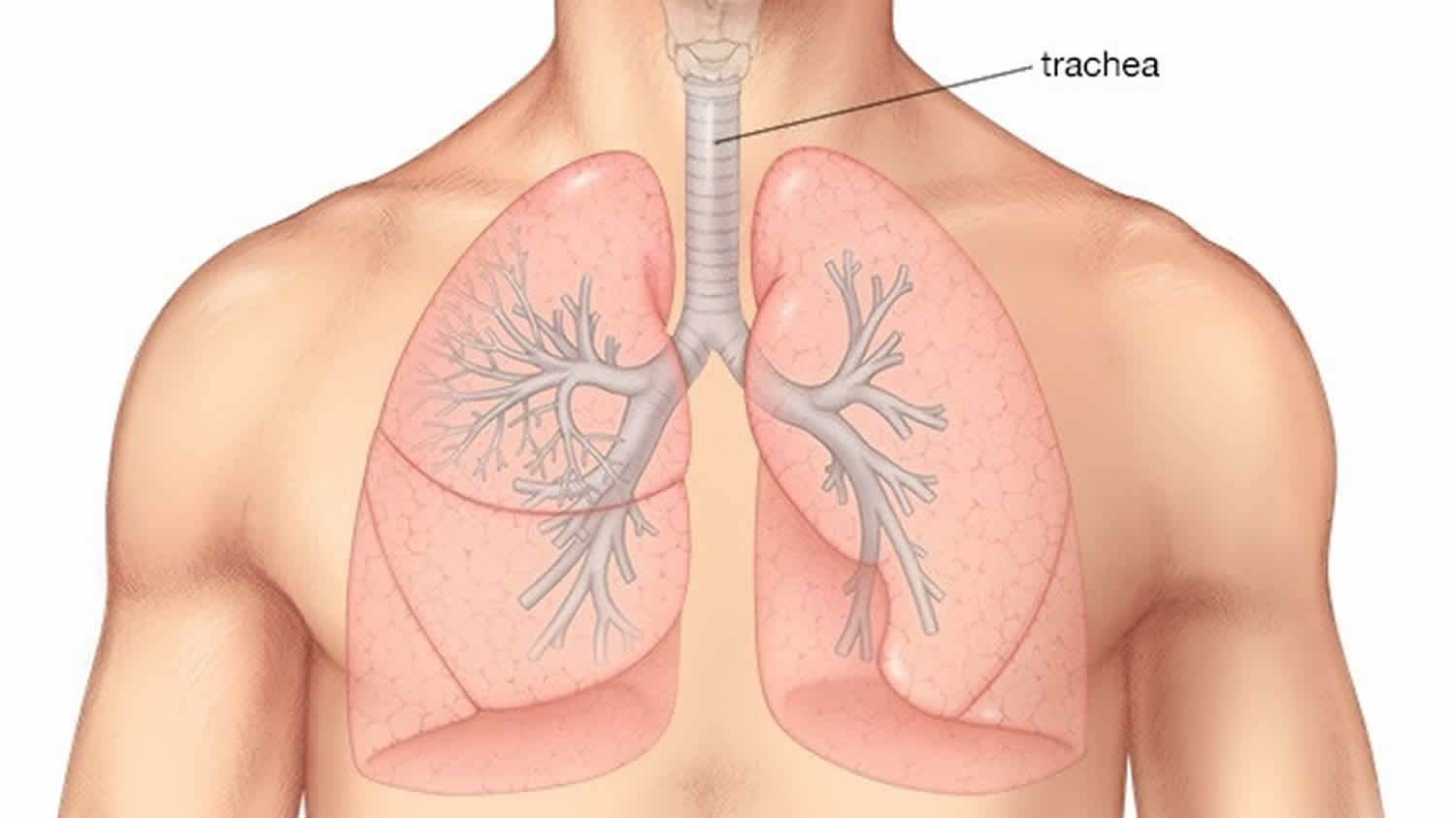
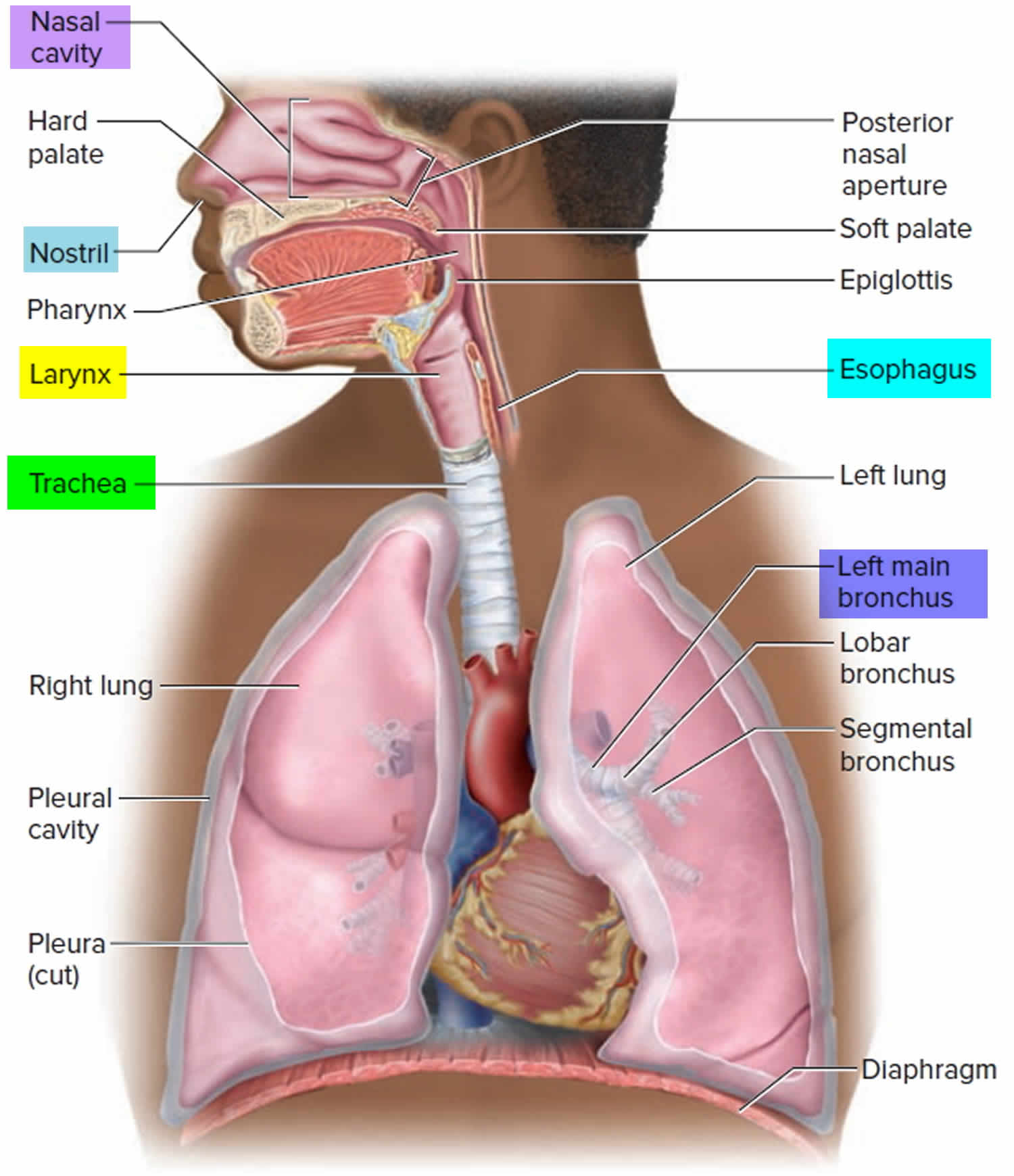
Figure 2. Trachea location
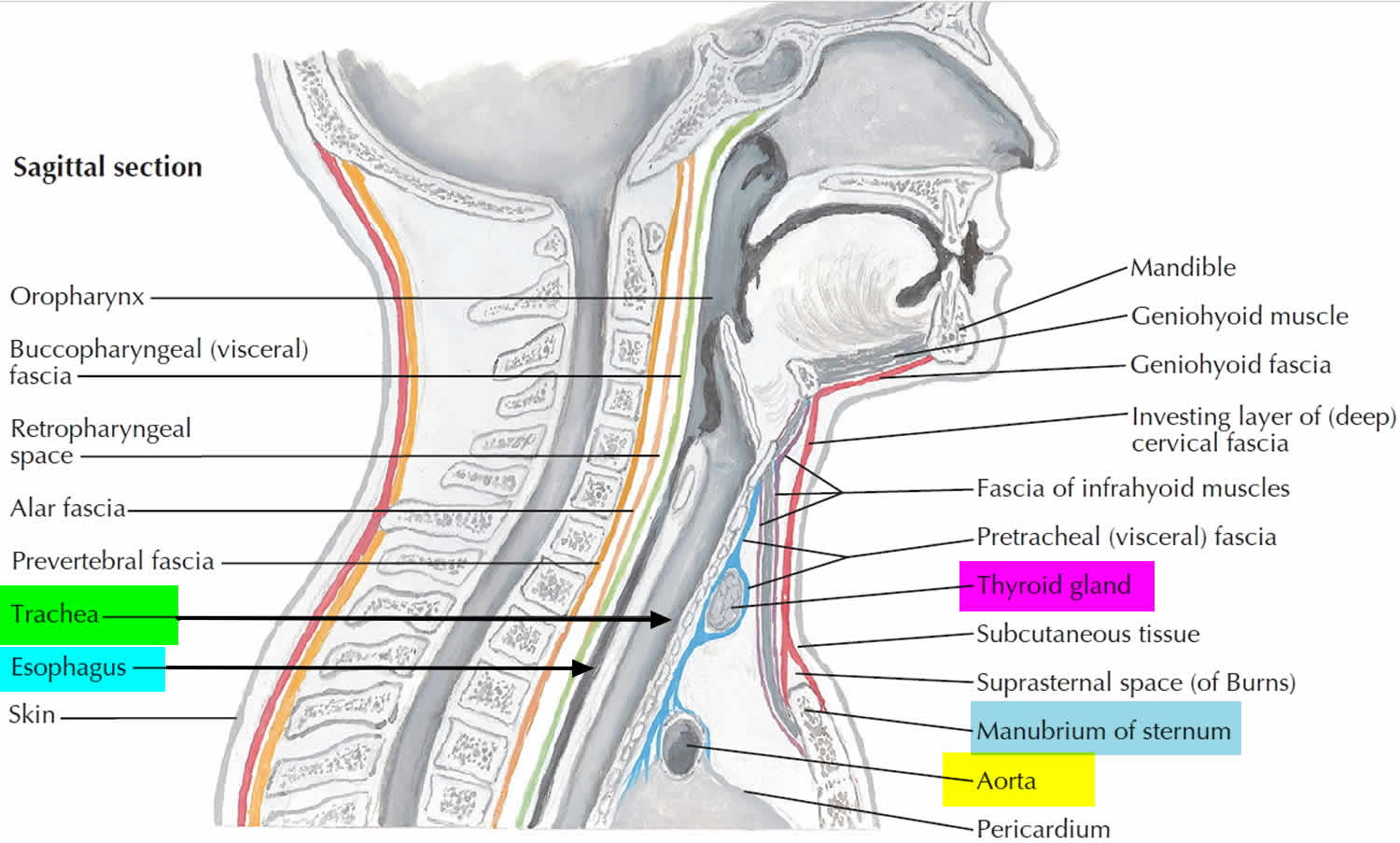
Figure 3. Trachea anatomy
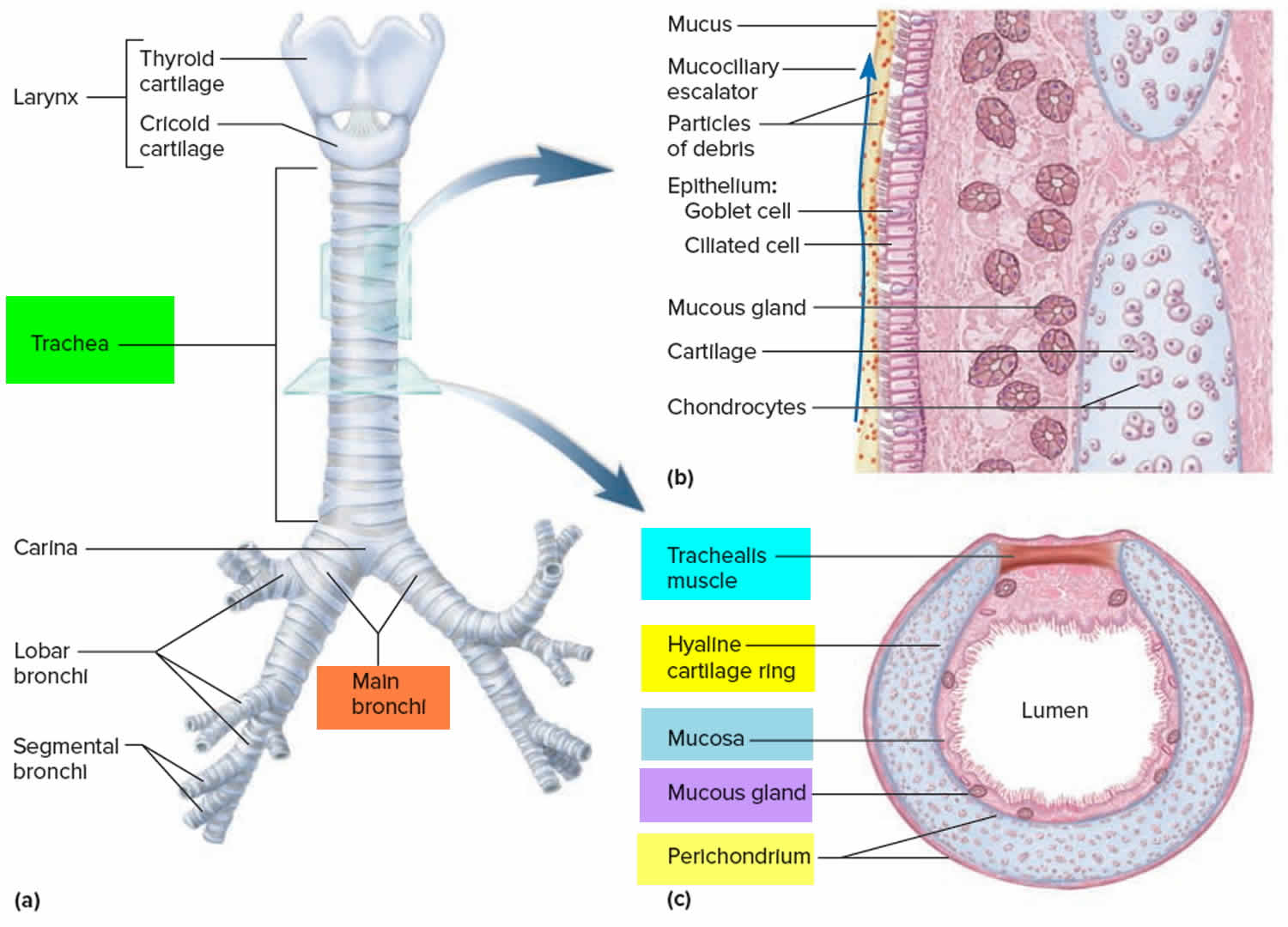
Footnote: (a) Anterior view. (b) Longitudinal section of the trachea showing the action of the mucociliary escalator. (c) Cross section of the trachea showing the C-shaped tracheal cartilage.
What is the function of the trachea?
The larynx is a cartilaginous chamber about 4 cm (1.5 in.) long (Figure 1). Its primary function is to keep food and drink out of the airway, but it evolved the additional role of sound production (phonation) in many animals; hence, we colloquially think of it as the “voice box.” The superior opening of the larynx is guarded by a flap of tissue called the epiglottis. At rest, the epiglottis stands almost vertically. During swallowing, however, extrinsic muscles of the larynx pull the larynx upward toward the epiglottis, the tongue pushes the epiglottis downward to meet it, and the epiglottis closes the airway and directs food and drink into the esophagus behind it.
The inner lining of the trachea is a pseudostratified columnar epithelium composed mainly of mucus-secreting goblet cells, ciliated cells, and short basal stem cells (Figure 3). The mucus traps inhaled particles, and the upward beating of the cilia drives the debris-laden mucus toward the pharynx, where it is swallowed. This mechanism of debris removal is called the mucociliary escalator. The connective tissue beneath the tracheal epithelium contains lymphatic nodules, mucous and serous glands, and the tracheal cartilages. The outermost layer of the trachea, called the adventitia, is fibrous connective tissue that blends into the adventitia of other organs of the mediastinum, especially the esophagus. At the level of the sternal angle, the trachea forks into the right and left main bronchi. The lowermost tracheal cartilage has an internal median ridge called the carina that directs the airflow to the right and left bronchus.
Tracheal stenosis causes
Tracheal stenosis can be present at birth (congenital). The cause of congenital tracheal stenosis is unknown.
Tracheal stenosis can also be acquired. It can develop when scar tissue forms in the trachea due to prolonged intubation or airway surgery. Intubation occurs when a tube is inserted into the trachea to help maintain breathing during a medical or surgical procedure.
Autoimmune diseases such as systemic lupus erythematosus, rheumatoid arthritis, vasculitis, sarcoidosis, and scleroderma, among others, can cause laryngotracheal stenosis 3). Infectious causes include bacterial tracheitis, viral papillomatosis, and tuberculosis. Neoplasm at the level of the larynx or trachea can also cause narrowing of the airway, with squamous cell carcinoma and adenoma being the most common malignancies in this setting.[2] Direct injury to the trachea by trauma, inhalation burns, or radiation are a few causes of traumatic laryngotracheal stenosis 4).
Tracheal stenosis symptoms
Symptoms of tracheal stenosis can be present shortly after birth or develop after an injury to the trachea. Symptoms include:
- noisy breathing (stridor)
- recurring pneumonia
- wheezing
- blue spells (cyanosis)
- paused in breathing (apnea)
- chest congestion
An upper respiratory infection can worsen the symptoms.
Tracheal stenosis diagnosis
Tracheal stenosis is diagnosed through a comprehensive aero-digestive evaluation that may include one or more of the following tests:
- Airway fluoroscopy
- Bronchoscopy
- CT with 3‐D reconstruction
- Echocardiogram
- Laryngoscopy
Tracheal stenosis treatment
Tracheal stenosis treatment depends on the severity of your child’s stenosis. Your child may outgrow the problem without intervention or, if the problem is severe, surgery may be required. Your child’s treatment plan may include:
Tracheal stenosis surgery
Doctors use minimally invasive techniques to treat tracheal stenosis. In some cases, tissue may be divided using a specialized knife and then dilated with a balloon. Lasers can be used to remove segmental portions of scar tissue.
Open surgery
Surgeons also use open surgery to treat tracheal stenosis. The most common open surgical procedures to treat tracheal stenosis are:
- Laryngotracheoplasty: Surgical repair of the stenosis, during which the narrowed diameter of the windpipe (trachea) is enlarged by inserting an elliptical piece of cartilage (taken from the child’s rib or ear, depending on the size of cartilage needed).
- Cricotracheal resection: A procedure in which the scar tissue and most of the ring-shaped cartilage of the larynx is cut out and the normal trachea is brought up to replace it.
- Segmental tracheal resection: A procedure where surgeons remove the defective tracheal segment and then repair the airway by suturing (attaching) the remaining ends back together.
- Slide tracheoplasty: A complex procedure to make the airway larger. During this surgery, the narrowed trachea is divided across the middle of the stenosis (the area where the airway is narrowed). A portion of the lower and upper tracheal segments are cut and then attached, resulting in an airway that is wider and shorter than before.
Tracheal stenosis surgery recovery
Johnson et al 5) analyzed 2014-2016 data from the American College of Surgeons (ACS) National Surgical Quality Improvement Program to determine perioperative outcomes for 126 patients who underwent tracheal resection or tracheoplasty. Such outcomes included length of stay, dehiscence, unplanned reintubations, unplanned surgeries, and 30-day readmission rates. The median length of stay was 7 days. Six patients (4.8%) developed wound infections, and three (2.4%) developed wound dehiscence. Five (4.0%) required unplanned reintubation, and 16 (13%) had an unplanned reoperation. The 30-day unplanned readmission rate was 16% (20/126).
References [ + ]





{kind=link}