
Contents
- Postpartum hemorrhage
- Postpartum hemorrhage causes
- Postpartum hemorrhage prevention
- Postpartum hemorrhage signs and symptoms
- Postpartum hemorrhage complications
- Postpartum hemorrhage diagnosis
- Postpartum hemorrhage treatment
Postpartum hemorrhage
Postpartum hemorrhage is heavy bleeding following the birth of a baby. The American College of Obstetricians and Gynecologists defines early postpartum hemorrhage as at least 1,000 mL total blood loss or loss of blood coinciding with signs and symptoms of hypovolemia within 24 hours after delivery of the fetus or intrapartum loss 1). The traditional definition of primary postpartum hemorrhage is the loss of 500 ml or more of blood from the genital tract within 24 hours of the birth of a baby. Primary postpartum hemorrhage may occur before delivery of the placenta and up to 24 hours after delivery of the fetus. Postpartum hemorrhage is the most common form of major obstetric hemorrhage and it occurs in up to 18 percent of births 2). Postpartum hemorrhage can be minor (500–1000 ml) or major (more than 1000 ml). Major could be divided to moderate (1000–2000 ml) or severe (more than 2000 ml). Annually, these preventable events are the cause of one-fourth of maternal deaths worldwide and 12% of maternal deaths in the United States 3).
Postpartum hemorrhage can be primary or secondary:
- Primary postpartum hemorrhage is when you lose 500 ml (a pint) or more of blood within the first 24 hours after the birth of your baby. Primary postpartum hemorrhage can be minor, where you lose 500–1000 ml (one or two pints), or major, where you lose more than 1000 ml (more than two pints).
- Secondary postpartum hemorrhage occurs when you have abnormal or heavy vaginal bleeding between 24 hours and 12 weeks after the birth.
About 1 to 5 percent of women have postpartum hemorrhage and it is more likely with a cesarean birth. Hemorrhage most commonly occurs after the placenta is delivered. The average amount of blood loss after the birth of a single baby in vaginal delivery is about 500 ml (or about a half of a quart). The average amount of blood loss for a cesarean birth is approximately 1,000 ml (or one quart). Most postpartum hemorrhage occurs right after delivery, but it can occur later as well.
Blood loss exceeding 1,000 mL is considered physiologically significant and can result in hemodynamic instability 4). Even with appropriate management, approximately 3 percent of vaginal deliveries will result in severe post-partum hemorrhage 5).
Complications from postpartum hemorrhage include orthostatic hypotension, anemia, and fatigue, which may make maternal care of the newborn more difficult. Post-partum anemia increases the risk of post-partum depression 6). Blood transfusion may be necessary and carries associated risks 7). In the most severe cases, hemorrhagic shock may lead to anterior pituitary ischemia with delay or failure of lactation (i.e., postpartum pituitary necrosis) 8). Occult myocardial ischemia, dilutional coagulopathy, and death also may occur 9). Delayed postpartum hemorrhage, bleeding after 24 hours as a result of sloughing of the placental eschar or retained placental fragments, also can occur 10).
Postpartum hemorrhage is one of the true surgical emergencies in obstetrics. The condition is best managed by an interprofessional team that also includes laboratory personnel and labor and delivery nurses.
The treatment and management of postpartum hemorrhage are focused on resuscitation of the patient while identifying and treating the specific cause. However, in many cases the cause is surgical. Maintaining hemodynamic stability of the patient is important to ensure continued perfusion to vital organs. Ample intravenous (IV) access should be obtained. Careful direct assessment of cumulative blood loss is important, and a focus should be on early initiation of protocols for the release of blood products and massive transfusion protocols. Rapid identification of the cause of postpartum hemorrhage and initiating treatment should be done simultaneously. To improve outcomes, the resuscitation should be done in an operating room setting as anesthesia assistance may be indicated for help with a difficult laceration repair, to correct uterine inversion, to help provide analgesia if needed for removal of retained products, or if surgical exploration is indicated.
Are some women more likely than others to have postpartum hemorrhage?
Yes. Things that make you more likely than others to have postpartum hemorrhage are called risk factors. Having a risk factor doesn’t mean for sure that you will have postpartum hemorrhage, but it may increase your chances. postpartum hemorrhage usually happens without warning. But talk to your health care provider about what you can do to help reduce your risk for having postpartum hemorrhage.
You’re more likely than other women to have postpartum hemorrhage if you’ve had it before. This is called having a history of postpartum hemorrhage. Asian and Hispanic women also are more likely than others to have postpartum hemorrhage. We don’t know why postpartum hemorrhage affects these groups of women more than others; researchers are working to learn more about it.
Several medical conditions are risk factors for postpartum hemorrhage. You may be more likely than other women to have postpartum hemorrhage if you have any of these conditions:
Conditions that affect the uterus
- Uterine atony. This is the most common cause of postpartum hemorrhage. It happens when the muscles in your uterus don’t contract (tighten) well after birth. Uterine contractions after birth help stop bleeding from the place in the uterus where the placenta breaks away. The placenta grows in your uterus and supplies the baby with food and oxygen through the umbilical cord. You may have uterine atony if your uterus is stretched or enlarged (also called distended) from giving birth to twins or a large baby (more than 8 pounds, 13 ounces). It also can happen if you’ve already had several children, you’re in labor for a long time or you have too much amniotic fluid. Amniotic fluid is the fluid that surrounds your baby in the womb.
- Uterine inversion. This is when the uterus turns inside out after birth.
- Uterine rupture. This is when the uterus tears during labor. It happens rarely. It may happen if you have a scar in the uterus from having a c-section in the past or if you’ve had other kinds of surgery on the uterus.
Conditions that affect the placenta
- Placental abruption. This is when the placenta separates from the wall of the uterus before birth. It can separate partially or completely.
- Placenta accreta, placenta increta or placenta percreta. These conditions happen when the placenta grows into the wall of the uterus too deeply.
- Placenta previa. This is when the placenta lies very low in the uterus and covers all or part of the cervix. The cervix is the opening to the uterus that sits at the top of the vagina.
- Retained placenta. This happens if you don’t pass the placenta within 30 to 60 minutes after you give birth. Even if you pass the placenta soon after birth, your provider checks the placenta to make sure it’s not missing any tissue. If tissue is missing and is not removed from the uterus right away, it may cause bleeding.
Conditions during labor and birth
- Having a C-section
- Getting general anesthesia. This is medicine that puts you to sleep so you don’t feel pain during surgery. If you have an emergency c-section, you may need general anesthesia.
- Taking medicines to induce labor. Providers often use a medicine called Pitocin to induce labor. Pitocin is the man-made form of oxytocin, a hormone your body makes to start contractions.
- Taking medicines to stop contractions during preterm labor. If you have preterm labor, your provider may give you medicines called tocolytics to slow or stop contractions.
- Tearing (also called lacerations). This may happen if the tissues in your vagina or cervix are cut or torn during birth. The cervix is the opening to the uterus that sits at the top of the vagina. You may have tearing if you give birth to a large baby, your baby is born through the birth canal too quickly or you have an episiotomy that tears. An episiotomy is a cut made at the opening of the vagina to help let the baby out. Tearing also can happen if your provider uses tools, like forceps or a vacuum, to help move your baby through the birth canal during birth. Forceps look like big tongs. A vacuum is a soft plastic cup that attaches to your baby’s head. It uses suction to gently pull your baby as you push during birth.
- Having quick labor or being in labor a long time. Labor is different for every woman. If you’re giving birth for the first time, labor usually takes about 14 hours. If you’ve given birth before, it usually takes about 6 hours.
Other conditions
- Blood conditions, like von Willebrand disease or disseminated intravascular coagulation (also called DIC). These conditions can increase your risk of forming a hematoma. A hematoma happens when a blood vessel breaks causing a blood clot to form in tissue, an organ or another part of the body. After giving birth, some women develop a hematoma in the vaginal area or the vulva (the female genitalia outside of the body). Von Willebrand’s disease is a bleeding disorder that makes it hard for a person to stop bleeding. DIC causes blood clots to form in small blood vessels and can lead to serious bleeding. Certain pregnancy and childbirth complications (like placenta accreta), surgery, sepsis (blood infection) and cancer can cause DIC.
- Infection, like chorioamnionitis. This is an infection of the placenta and amniotic fluid.
- Intrahepatic cholestasis of pregnancy (also called ICP). This is the most common liver condition that happens during pregnancy.
- Obesity. Being obese means you have an excess amount of body fat. If you’re obese, your body mass index (also called BMI) is 30 or higher. BMI is a measure of body fat based on your height and weight.
- Preeclampsia or gestational hypertension. These are types of high blood pressure that only pregnant women can get. Preeclampsia is a condition that can happen after the 20th week of pregnancy or right after pregnancy. It’s when a pregnant woman has high blood pressure and signs that some of her organs, like her kidneys and liver, may not be working properly. Signs of preeclampsia include having protein in the urine, changes in vision and severe headache. Gestational hypertension is high blood pressure that starts after 20 weeks of pregnancy and goes away after you give birth. Some women with gestational hypertension have preeclampsia later in pregnancy.
What can be done during birth to reduce my chance of a primary postpartum hemorrhage?
If you have a vaginal birth, you should be offered an injection into your thigh just as the baby is born to help reduce blood loss. This injection helps the placenta to come away from the womb. Once your placenta has been delivered, you will be examined for any tears. If the tears are bleeding heavily, they will be stitched to reduce any further blood loss.
If you have a caesarean section, the same injection will be given and your placenta will be removed through the caesarean incision.
If you are known to be at high risk for postpartum hemorrhage, you may be given additional medications to help reduce the amount you may bleed.
Will I have another postpartum hemorrhage in my future births?
If you have had a birth that was complicated by a primary postpartum hemorrhage, there is an increased risk of postpartum hemorrhage in future births. This is why you will be advised to have your baby in a consultant-led maternity unit. During pregnancy you may be advised to take iron supplements to reduce the chance of becoming anaemic. You should discuss your birth options with your healthcare team.
When you are in the hospital and in labor, you may have blood tests and a drip may be inserted into your arm so that fluids and medication can be given if needed. You will be offered medication to help the placenta come away and reduce the risk of a postpartum hemorrhage.
What happens if I have a secondary postpartum hemorrhage?
Secondary postpartum hemorrhage is often associated with infection in the womb. Occasionally it may be associated with some placental tissue remaining in your womb. It usually occurs after you have left hospital. You should contact your midwife or doctor if your bleeding is getting heavier, if your lochia has an offensive smell or if you feel unwell. You may be given a course of antibiotics to treat an infection.
If the bleeding is heavy or continues, you may need to go to hospital for further tests. You may need antibiotics which will be given through a drip. Less commonly, you may need an operation to remove any small pieces of remaining placenta from your womb. You may need to stay in hospital for a few days.
Your baby can usually stay with you if you wish, and you can continue to breastfeed.
Postpartum hemorrhage causes
Once a baby is delivered, the uterus normally continues to contract (tightening of uterine muscles) and expels the placenta. After the placenta is delivered, these contractions help compress the bleeding vessels in the area where the placenta was attached. If the uterus does not contract strongly enough, called uterine atony, these blood vessels bleed freely and hemorrhage occurs. This is the most common cause of postpartum hemorrhage. If small pieces of the placenta remain attached, bleeding is also likely.
Some women are at greater risk for postpartum hemorrhage than others. Conditions that may increase the risk for postpartum hemorrhage include the following:
- Placental abruption. The early detachment of the placenta from the uterus.
- Placenta previa. The placenta covers or is near the cervical opening.
- Overdistended uterus. Excessive enlargement of the uterus due to too much amniotic fluid or a large baby, especially with birthweight over 4,000 grams (8.8 pounds).
- Multiple pregnancy. More than one placenta and overdistention of the uterus.
- Gestational hypertension or preeclampsia. High blood pressure of pregnancy.
- Having many previous births
- Prolonged labor
- Infection
- Obesity
- Medications to induce labor
- Medications to stop contractions (for preterm labor)
- Use of forceps or vacuum-assisted delivery
- General anesthesia
Postpartum hemorrhage may also be due to other factors including the following:
- Tear in the cervix or vaginal tissues
- Tear in a uterine blood vessel
- Bleeding into a concealed tissue area or space in the pelvis which develops into a hematoma, usually in the vulva or vaginal area
- Blood clotting disorders, such as disseminated intravascular coagulation
- Placenta accreta. The placenta is abnormally attached to the inside of the uterus (a condition that occurs in one in 2,500 births and is more common if the placenta is attached over a prior cesarean scar).
- Placenta increta. The placental tissues invade the muscle of the uterus.
- Placenta percreta. The placental tissues go all the way into the uterine muscle and may break through (rupture).
Although an uncommon event, uterine rupture can be life-threatening for the mother. Conditions that may increase the risk of uterine rupture include surgery to remove fibroid (benign) tumors and a prior cesarean scar. A prior scar on the uterus in the upper part of the fundus has a higher risk of uterine rupture compared with a horizontal scar in the lower uterine segment called a lower transverse incision. It can also occur before delivery and place the fetus at risk as well.
Uterine atony
Uterine atony is the most common cause of postpartum hemorrhage 11). Brisk blood flow after delivery of the placenta unresponsive to transabdominal massage should prompt immediate action including bimanual compression of the uterus and use of uterotonic medications. Massage is performed by placing one hand in the vagina and pushing against the body of the uterus while the other hand compresses the fundus from above through the abdominal wall (see Figure 2 below).
Trauma
Lacerations and hematomas due to birth trauma can cause significant blood loss that can be lessened by hemostasis and timely repair. Episiotomy increases the risk of blood loss and anal sphincter tears; this procedure should be avoided unless urgent delivery is necessary and the perineum is thought to be a limiting factor 12).
Vaginal and vulvar hematomas can present as pain or as a change in vital signs disproportionate to the amount of blood loss. Small hematomas can be managed with ice packs, analgesia, and observation. Patients with persistent signs of volume loss despite fluid replacement, as well as those with large (greater than 3 to 4 cm) or enlarging hematomas, require incision and evacuation of the blood clot 13). The involved area should be irrigated and hemostasis achieved by ligating bleeding vessels, placing figure-of-eight sutures, and creating a layered closure, or by using any of these methods alone.
Uterine inversion is rare, occurring in only 0.04% of deliveries, and is a potential cause of postpartum hemorrhage 14). Active management of the third stage of labor (AMTSL) does not appear to increase the incidence of uterine inversion, but invasive placenta does 15). The contributions of other conditions such as fundal implantation of the placenta, fundal pressure, and undue cord traction are unclear 16). The inverted uterus usually appears as a bluish-gray mass protruding from the vagina. Patients with uterine inversion may have signs of shock without excess blood loss. If the placenta is attached, it should be left in place until after reduction to limit hemorrhage 17). Every attempt should be made to quickly replace the uterus. The Johnson method of reduction begins with grasping the protruding fundus with the palm of the hand, directing the fingers toward the posterior fornix 18). The uterus is returned to position by lifting it up through the pelvis and into the abdomen (see Figure 3 below). Once the uterus is reverted, uterotonic agents can promote uterine tone and prevent recurrence. If initial attempts to replace the uterus fail or contraction of the lower uterine segment (contraction ring) develops, the use of magnesium sulfate, terbutaline, nitroglycerin, or general anesthesia may allow sufficient uterine relaxation for manipulation 19).
Uterine rupture can cause intrapartum and postpartum hemorrhage 20). Although rare in an unscarred uterus, clinically significant uterine rupture occurs in 0.8% of vaginal births after cesarean delivery via low transverse uterine incision 21). Induction and augmentation increase the risk of uterine rupture, especially for patients with prior cesarean delivery 22). Before delivery, the primary sign of uterine rupture is fetal bradycardia 23).
Other signs and symptoms of uterine rupture are:
- Abdominal tenderness
- Circulatory collapse
- Elevation of presenting fetal part
- Fetal bradycardia (most common initial presenting sign)
- Increasing abdominal girth
- Loss of uterine contractions
- Maternal tachycardia
- Vaginal bleeding.
Retained tissue
Retained tissue (i.e., placenta, placental fragments, or blood clots) prevents the uterus from contracting enough to achieve optimal tone. Classic signs of placental separation include a small gush of blood, lengthening of the umbilical cord, and a slight rise of the uterus. The mean time from delivery to placental expulsion is eight to nine minutes.33 Longer intervals are associated with an increased risk of postpartum hemorrhage, with rates doubling after 10 minutes 24). Retained placenta (i.e., failure of the placenta to deliver within 30 minutes) occurs in less than 3% of vaginal deliveries 25). If the placenta is retained, consider manual removal using appropriate analgesia 26). Injecting the umbilical vein with saline and oxytocin does not clearly reduce the need for manual removal 27). If blunt dissection with the edge of the gloved hand does not reveal the tissue plane between the uterine wall and placenta, invasive placenta should be considered.
Invasive placenta (placenta accreta, increta, or percreta) can cause life-threatening postpartum hemorrhage 28). The incidence has increased with time, mirroring the increase in cesarean deliveries 29). In addition to prior cesarean delivery, other risk factors for invasive placenta include placenta previa, advanced maternal age, high parity, and previous invasive placenta 30). Treatment of invasive placenta can require hysterectomy or, in select cases, conservative management (i.e., leaving the placenta in place or giving weekly oral methotrexate) 31).
Coagulation defects
Coagulation defects can cause a hemorrhage or be the result of one. Coagulation defects should be suspected in patients who have not responded to the usual measures to treat postpartum hemorrhage or who are oozing from puncture sites. A coagulation defect should also be suspected if blood does not clot in bedside receptacles or red-top (no additives) laboratory collection tubes within five to 10 minutes. Coagulation defects may be congenital or acquired. Evaluation should include a platelet count and measurement of prothrombin time, partial thromboplastin time, fibrinogen level, fibrin split products, and quantitative d-dimer assay. Physicians should treat the underlying disease process, if known, and support intravascular volume, serially evaluate coagulation status, and replace appropriate blood components using an emergency release protocol to improve response time and decrease risk of dilutional coagulopathy 32).
Causes of disordered coagulation include 33):
- Acquired oagulation defect
- Amniotic fluid embolism
- Consumptive coagulation secondary to excessive bleeding of any origin
- Disseminated intravascular coagulation secondary to abruption
- Fetal demise
- HELLP (hemolysis, elevated liver enzyme levels, and low platelet levels) syndrome
- Placental abruption
- Preeclampsia with severe features
- Sepsis
- Use of anticoagulants such as aspirin or heparin
- Chronic or congenital oagulation defect
- Hemophilia
- Idiopathic thrombocytopenic purpura
- Thrombotic thrombocytopenic purpura
- Von Willebrand disease
Postpartum hemorrhage risk factors
Risk factors for primary postpartum hemorrhage
- Before the birth
- known placenta previa – when the placenta is located lower down near the neck of the womb
- suspected or proven placental abruption – when the placenta separates from the womb early
- carrying twins or triplets
- pre-eclampsia and/or high blood pressure
- having had a postpartum hemorrhage in a previous pregnancy
- having a BMI (body mass index) of more than 35
- anemia
- uterine fibroids
- blood clotting problems
- taking blood-thinning medication
- In labor
- delivery by cesarean section
- induction of labor
- delay in delivery of your placenta (retained afterbirth)
- perineal tear or episiotomy (a surgical cut to help delivery)
- forceps or ventouse delivery
- having a long labour (more than 12 hours)
- having a large baby (more than 4 kg or 9 lb)
- having your first baby if you are more than 40 years old
- having a raised temperature (fever) during labor
- needing a general anesthetic during delivery
However, 20% of postpartum hemorrhage occurs in women with no risk factors, so physicians must be prepared to manage this condition at every delivery 34).
Often there is very little that you can do about these risk factors. However, in some cases, steps can be taken to reduce the risk of having a postpartum hemorrhage and also to reduce the likelihood of needing a blood transfusion:
- If you are anemic during pregnancy, taking iron supplements may reduce the likelihood of needing a blood transfusion. Some women may also be offered iron supplements if they are at risk of anemia. If you are very anemic during pregnancy or find it difficult to take tablets, iron can be given intravenously (through a drip).
- If you have had a previous caesarean section and the placenta attaches itself to the area of the previous scar, leading to placenta accreta/percreta (also known as morbidly adherent placenta), it may not come away easily after birth. This condition is uncommon but it can cause major hemorrhage. If this is suspected on your ultrasound scan, you may be offered additional scans. Your healthcare team will discuss your options with you and make a plan for your care.
Treating major hemorrhage may include having a blood transfusion (see below). If this worries you, or if you do not wish to receive blood or other blood products, you should talk to your healthcare team. It is important that your wishes are known well in advance and that they are written clearly in your notes.
Postpartum hemorrhage prevention
Identifying high-risk patients before delivery is one of the most important factors in preventing morbidity and mortality associated with postpartum hemorrhage. This allows for planning appropriate route and timing of delivery in the appropriate medical resource setting. Patients with previous cesarean delivery should have ultrasound evaluation antepartum to help determine appropriate route and place of delivery. Treatment of patients with anemia by either oral or parenteral iron supplementation should be considered, especially in patients with hematocrit less than 30%. Additionally, consideration for erythropoietin stimulating agents with hematology consultation should be undertaken in the high-risk patient, especially in those who do not accept a blood transfusion.
Standardized, multidisciplinary protocols have been used to help decrease severe maternal morbidity associated with postpartum hemorrhage that involves a focus on unit readiness, recognition and prevention, response, and reporting/systems learning. The nursing and anesthesia teams should be aware of the postpartum hemorrhage and available to assist. Simulation activities can be utilized in event training in postpartum hemorrhage and have been shown to improve outcomes.
Strategies for decreasing the morbidity and mortality associated with postpartum hemorrhage includes the choosing to deliver infants in women at high risk of postpartum hemorrhage at facilities with immediately available surgical, intensive care, and blood bank services.
The most effective strategy to prevent postpartum hemorrhage is active management of the third stage of labor (AMTSL) 35). Active management of the third stage of labor also reduces the risk of a postpartum maternal hemoglobin level lower than 9 g per dL (90 g per L) and the need for manual removal of the placenta 36). Components of this practice include: (1) administering oxytocin (Pitocin) with or soon after the delivery of the anterior shoulder; (2) controlled cord traction (Brandt-Andrews maneuver) to deliver the placenta; and (3) uterine massage after delivery of the placenta 37). Placental delivery can be achieved using the Brandt-Andrews maneuver, in which firm traction on the umbilical cord is applied with one hand while the other applies suprapubic counterpressure (see Figure 1) 38).
The individual components of active management of the third stage of labor have been evaluated and compared. Based on existing evidence, the most important component is administration of a uterotonic drug, preferably oxytocin 39). The number needed to treat to prevent one case of hemorrhage 500 mL or greater is 7 for oxytocin administered after delivery of the fetal anterior shoulder or after delivery of the neonate compared with placebo 40). The risk of postpartum hemorrhage is also reduced if oxytocin is administered after placental delivery instead of at the time of delivery of the anterior shoulder 41). Dosing instructions are provided in Table 1 below under medications.
An alternative to oxytocin is misoprostol (Cytotec), an inexpensive medication that does not require injection and is more effective than placebo in preventing postpartum hemorrhage 42). However, most studies have shown that oxytocin is superior to misoprostol 43). Misoprostol also causes more adverse effects than oxytocin—commonly nausea, diarrhea, and fever within three hours of birth 44).
The benefits of controlled cord traction and uterine massage in preventing postpartum hemorrhage are less clear, but these strategies may be helpful 45). Controlled cord traction does not prevent severe postpartum hemorrhage, but reduces the incidence of less severe blood loss (500 to 1,000 mL) and reduces the need for manual extraction of the placenta 46).
Figure 1. Brandt-Andrews maneuver
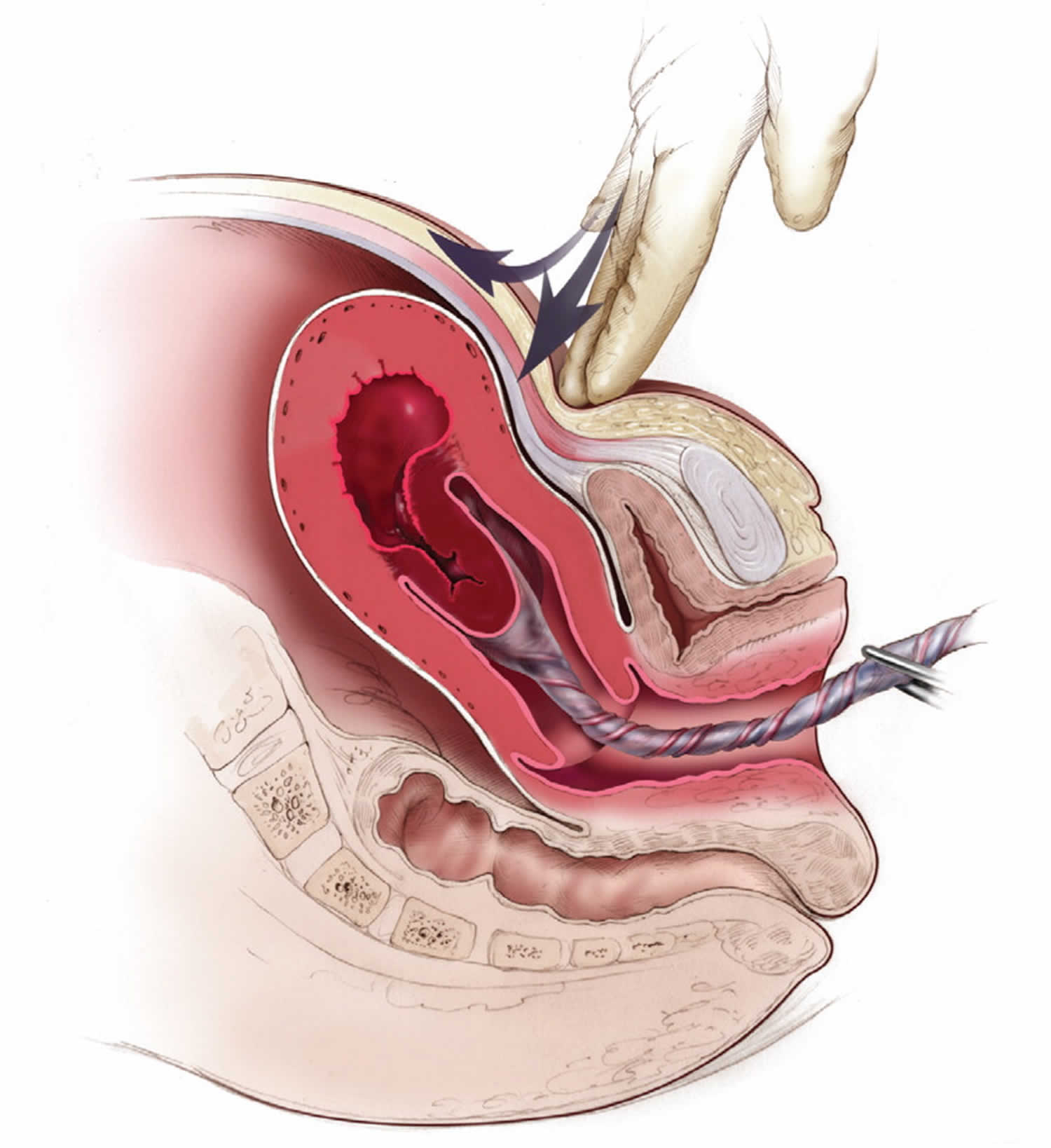
Figure 2. Bimanual uterine compression massage
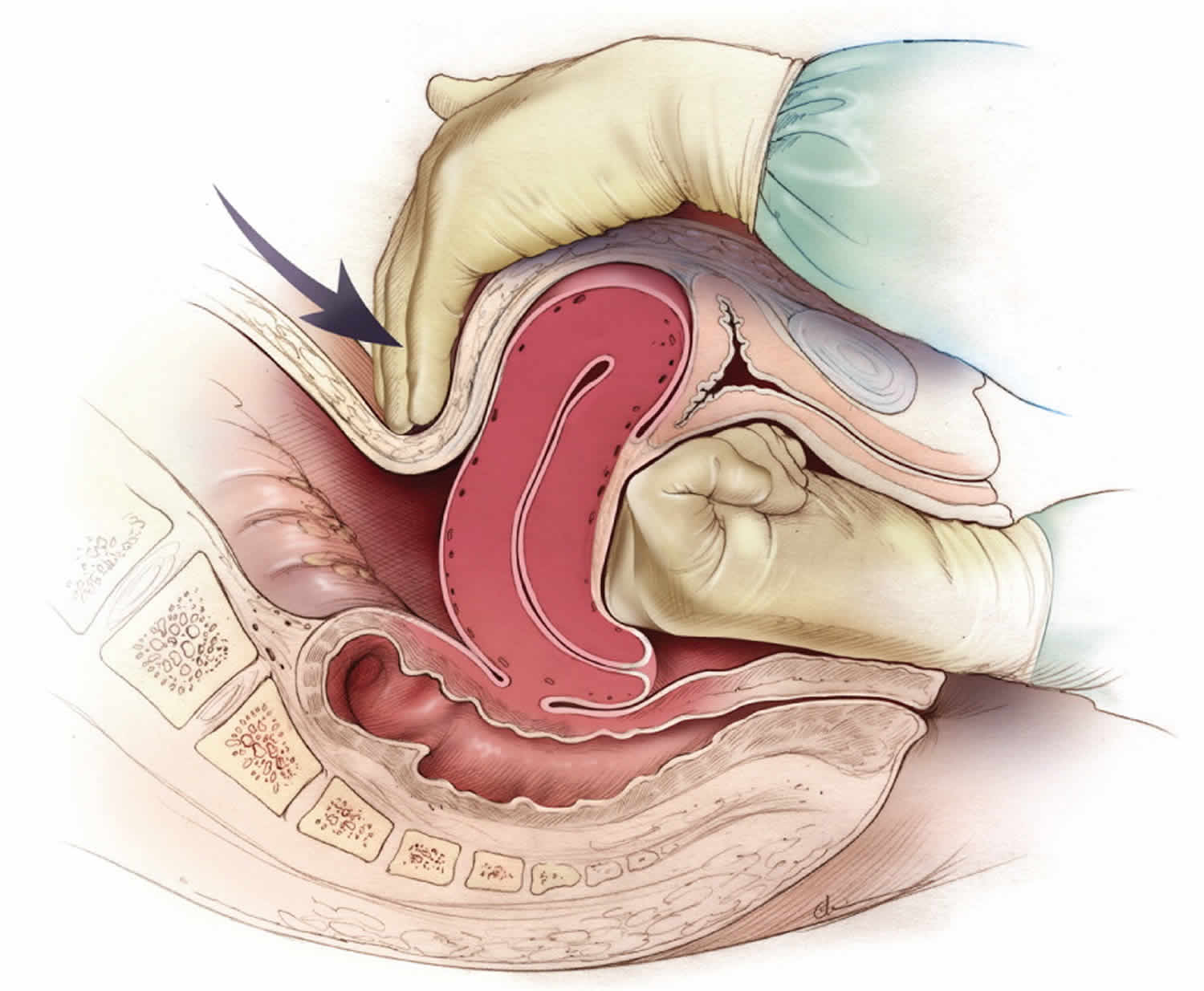
Footnote: Bimanual uterine compression massage. One hand is placed in the vagina and pushes against the body of the uterus while the other hand compresses the fundus from above through the abdominal wall. The posterior aspect of the uterus is massaged with the abdominal hand and the anterior aspect with the vaginal hand.
[Source 47) ]Figure 3. Reduction of uterine inversion (Johnson method)

Footnote: (A) The protruding fundus is grasped with fingers directed toward the posterior fornix. (B) The uterus is returned to position by pushing it through the pelvis and (C) into the abdomen with steady pressure toward the umbilicus.
[Source 48) ]Figure 4. Prevention and management of postpartum hemorrhage
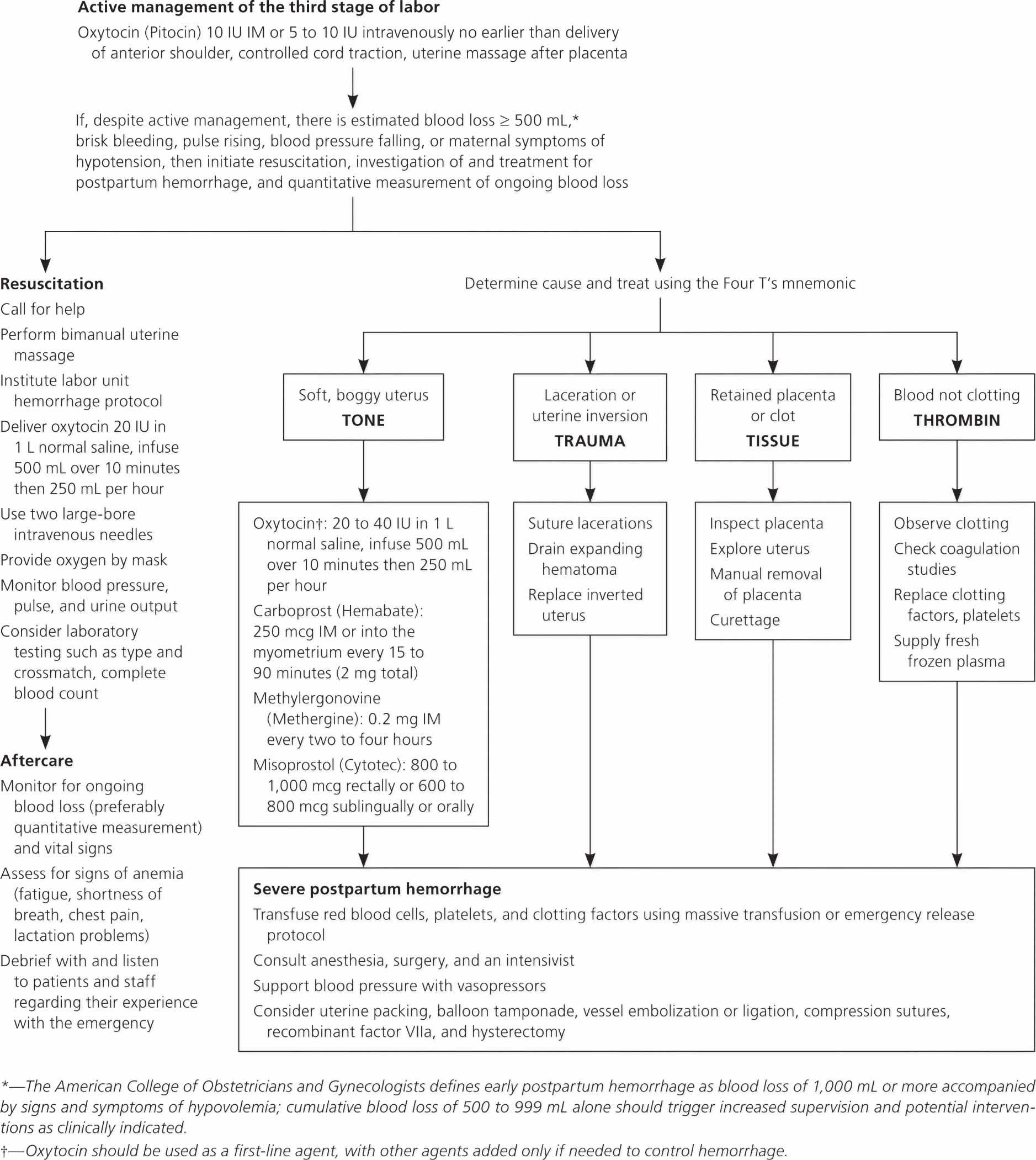
Footnote: Algorithm for the prevention and management of postpartum hemorrhage. Many of the steps involved in diagnosing and treating postpartum hemorrhage must be undertaken simultaneously. Steps in maternal resuscitation may differ based on the actual cause.
Abbreviations: IM = intramuscularly; PPH = postpartum hemorrhage.
[Source 49) ]Strategies to reduce morbidity and mortality from postpartum hemorrhage
- Readiness by every unit
- Have a hemorrhage cart with medications, supplies, checklist, and instruction cards immediately available
- Establish a response team and know who to call when help is needed
- Establish massive and emergency release transfusion protocols
- Institute unit education on protocols and run unit-based drills
- Recognition and prevention efforts for every patient
- Antenatal assessment
- Screen for and treat anemia antenatally
- Screen for sickle cell disease and thalassemia in women of African, Southeast Asian, or Mediterranean descent
- Obtain sonograms for women at high risk of invasive placenta
- Perform delivery in facility with blood bank and in-house surgical services if the patient has a high risk of hemorrhage
- Identify Jehovah’s Witnesses and other patients who decline blood products
- Antenatal assessment
- Intrapartum management
- Use active management of the third stage of labor in every delivery
- Avoid routine episiotomy
- Avoid instrumented deliveries, especially forceps
- Use perineal warm compresses
- Measure cumulative blood loss and track postpartum vital signs
- Response for every hemorrhage
- Use an emergency management plan with checklists
- Provide support program for patients, families, and staff
- Reporting and systems learning for every unit
- Establish a culture of huddles and postevent debriefs
- Complete a multidisciplinary review for systems issues
- Establish a perinatal quality improvement committee.
Postpartum hemorrhage signs and symptoms
The following are the most common symptoms of postpartum hemorrhage. However, each woman may experience symptoms differently. Symptoms may include:
- Uncontrolled bleeding
- Decreased blood pressure
- Increased heart rate
- Decrease in the red blood cell count (hematocrit)
- Swelling and pain in tissues in the vaginal and perineal area, if bleeding is due to a hematoma
The symptoms of postpartum hemorrhage may resemble other conditions or medical problems. Always consult your doctor for a diagnosis.
Excessive and rapid blood loss can cause a severe drop in the mother’s blood pressure and may lead to shock and death if not treated.
Postpartum hemorrhage complications
Complications of postpartum hemorrhage range from worsening of common postpartum symptoms such as fatigue and depressed mood, to death from cardiovascular collapse.
Complications of postpartum hemorrhage include 51):
- Anemia
- Anterior pituitary ischemia with delay or failure of lactation (i.e., Sheehan syndrome or postpartum pituitary necrosis)
- Blood transfusion
- Death
- Dilutional coagulopathy
- Fatigue
- Myocardial ischemia
- Orthostatic hypotension
- Postpartum depression
Postpartum hemorrhage diagnosis
In addition to a complete medical history and physical examination, postpartum hemorrhage diagnosis is usually based on symptoms, with laboratory tests often helping with the diagnosis. Tests used to diagnose postpartum hemorrhage may include:
- Estimation of blood loss (this may be done by counting the number of saturated pads, or by weighing of packs and sponges used to absorb blood; 1 milliliter of blood weighs approximately one gram)
- Pulse rate and blood pressure measurement
- Hematocrit (red blood cell count)
- Clotting factors in the blood
Postpartum hemorrhage treatment
The treatment and management of postpartum hemorrhage are focused on resuscitation of the patient while identifying and treating the specific cause 52). Transfer to an operating suite with anesthesia assistance may be indicated for help with a difficult laceration repair, to correct uterine inversion, to help provide analgesia if needed for removal of retained products, or if surgical exploration is indicated.
Specific treatment for postpartum hemorrhage will be determined by your doctor based on:
- Your pregnancy, overall health, and medical history
- Extent of the condition
- Your tolerance for specific medications, procedures, or therapies
- Expectations for the course of the condition
- Your opinion or preference
The aim of treatment of postpartum hemorrhage is to find and stop the cause of the bleeding as quickly as possible.
Treatment depends on what’s causing your bleeding. It may include:
- Getting fluids, medicine (like Pitocin to stimulate uterine contractions) or having a blood transfusion (having new blood put into your body). You get these treatments through a needle into your vein (also called intravenous or IV), or you may get some directly in the uterus.
- Having surgery, like a hysterectomy or a laparotomy. A hysterectomy is when your provider removes your uterus. You usually only need a hysterectomy if other treatments don’t work. A laparotomy is when your provider opens your belly to check for the source of bleeding and stops the bleeding.
- Massaging the uterus by hand (to stimulate contractions). Your provider can massage the uterus to help it contract, lessen bleeding and help the body pass blood clots.
- Getting oxygen by wearing an oxygen mask
- Removing any remaining pieces of the placenta from the uterus, packing the uterus with gauze, a special balloon or sponges, or using medical tools or stitches to help stop bleeding from blood vessels.
- Examination of the uterus and other pelvic tissues
- Bakri balloon or a Foley catheter to compress the bleeding inside the uterus. Packing the uterus with sponges and sterile materials may be used if a Bakri balloon or Foley catheter is not available.
- Embolization of the blood vessels that supply the uterus. In this procedure, a provider uses special tests to find the bleeding blood vessel and injects material into the vessel to stop the bleeding. It’s used in special cases and may prevent you from needing a hysterectomy.
- Tying-off of bleeding blood vessels using uterine compression sutures
- Laparotomy. Surgery to open the abdomen to find the cause of the bleeding.
- Hysterectomy. Surgical removal of the uterus; in most cases, this is a last resort.
Replacing lost blood and fluids is important in treating postpartum hemorrhage. Intravenous (IV) fluids, blood, and blood products may be given rapidly to prevent shock. The mother may also receive oxygen by mask.
Postpartum hemorrhage can be quite serious. However, quickly detecting and treating the cause of bleeding can often lead to a full recovery.
If you have had your baby at home or in a midwifery-led unit, your midwife will call for assistance and arrange your transfer to hospital.
If you give birth in hospital, your midwife will push the emergency bell to call other members of staff into the room to help. It can happen quickly and people rushing into the room may be frightening for you and your birth partner. Your midwife will tell you and your partner what is happening and why.
You may feel dizzy, light-headed, faint or nauseous. In the majority of cases (whether you are at home, in a midwifery-led unit or in hospital), heavy bleeding will settle with the simple measures listed below.
The midwife or doctor may:
- massage your womb through your abdomen, and sometimes vaginally, to encourage it to contract
- give a second injection into your thigh (or a first, if you did not have one at the time of the birth) to help your womb contract
- put a catheter (tube) into your bladder to empty it as this may help the womb contract
- put a drip into your arm to give you some warm fluids after taking some blood for testing
- check to make sure that all of the placenta has come out. If there are any missing pieces still inside your womb, you may have to have them removed; this is usually done in an operating room under anesthetic
- examine you to see whether any stitches are required.
Your blood pressure, temperature and pulse will be checked regularly and you will stay on the labour ward until the bleeding has settled. You can breastfeed if you wish.
Postpartum hemorrhage treatment
If the postpartum hemorrhage is due to uterine atony, treatment modalities include medical management with uterotonic agents, uterine tamponade, pelvic artery embolization, and surgical management.
Medical management with uterotonic and pharmacologic agents is typically the first step if uterine atony is identified. While oxytocin is given routinely by most institutions at the time of delivery (see prevention), additional uterotonic medications may be given with bimanual massage in an initial response to hemorrhage. Uterotonic agents include oxytocin, ergot alkaloids, and prostaglandins.
If bimanual massage and uterotonic medications are not sufficient to control hemorrhage, uterine tamponade may be considered. An intrauterine balloon tamponade system can be used, typically by filling an intrauterine balloon with 250 to 500 mL of normal saline. If there is not an intrauterine balloon readily available, the uterus may be packed with gauze, or multiple large Foley catheters may be placed concurrently. It is important to keep an accurate count of anything placed in the uterus to prevent retained foreign body.
Uterine artery embolization may be considered in the stable patient with persistent bleeding. Fluoroscopy is used to identify and occlude bleeding vessels. While the unstable patient is not a candidate for this modality, it has the benefit of uterine conservation and possible future fertility.
Exploratory laparotomy is typically indicated in the setting where less invasive measures for postpartum hemorrhage have failed or if the suspected reason for postpartum hemorrhage such as morbidly adherent placenta, demands it. A midline vertical abdominal incision should be considered to maximize exposure; however, if the patient had a cesarean delivery, the existing incision may be utilized. Vascular ligation sutures may be attempted to decrease pulse pressure at the uterus. Bilateral uterine artery ligation (O’Leary sutures) sutures may be placed as well as bilateral utero-ovarian ligament ligation sutures. Ligation of the internal iliac arteries may also be performed however as this entails a retroperitoneal approach, it is rarely used. Uterine compression sutures may also be used as a treatment for atony. The B-Lynch suture technique, the most commonly performed of the compression sutures, physically compresses the uterus looping from the cervix to the fundus. The definitive treatment for postpartum hemorrhage is a hysterectomy. A peripartum hysterectomy is associated not only with permanent sterility but also increased surgical risk with higher risk of bladder and ureteral injury. Supracervical hysterectomy may be performed alternately as a faster surgery with potentially fewer complicated risks.
If the postpartum hemorrhage has a cause other than atony, the treatment modality should be specifically tailored to the cause. Genital tract lacerations should be repaired or pressure/packing used. Retained products of conception should be removed manually or by dilation and curettage procedure. Hematomas can be managed by observation alone or may need fluoroscopy/embolization or surgical intervention if needed. If the uterine inversion is the cause of postpartum hemorrhage, steady pressure with the fist is used to replace the uterus to correct position. Uterine relaxants such as a halogenated anesthetic, terbutaline, magnesium sulfate, or nitroglycerine can be used during uterine repositioning, with oxytocin and other uterotonics given once the uterus is in normal anatomical position. Occasionally surgical correction of inversion must be undertaken via laparotomy. If a coagulation deficit exists, blood factor and product replacement may be used to correct the deficit.
Postpartum hemorrhage medications
Commonly used uterotonic include:
- Oxytocin: A hormone naturally produced by the posterior pituitary works rapidly to cause uterine contraction with no contraindications and minimal side effects.
- Methylergonovine: Semi-synthetic ergot alkaloid. Works rapidly for sustained uterine contraction. Contraindicated in patients with hypertension.
- Carboprost (also known as 15-methyl prostaglandin F2α): Synthetic prostaglandin analogue of prostaglandin. Contraindicated in severe hepatic, renal, and cardiovascular disease, may cause bronchospasm in asthmatics.
- Misoprostol: Prostaglandin E1 analogue. More delayed onset than above medications.
Oxytocin is the most effective treatment for postpartum hemorrhage, even if already used for labor induction or augmentation or as part of active management of the third stage of labor (AMTSL) 53). The choice of a second-line uterotonic should be based on patient-specific factors such as hypertension, asthma, or use of protease inhibitors. Although it is not a uterotonic, tranexamic acid (Cyklokapron) may reduce mortality due to bleeding from postpartum hemorrhage (but not overall mortality) when given within the first three hours and may be considered as an adjuvant therapy 54). Table 1 outlines dosages, cautions, contraindications, and common adverse effects of uterotonic medications and tranexamic acid 55).
Table 1. Medications used for Prevention and Treatment of Postpartum Hemorrhage
| Medication | Dosage | Prevention | Treatment | Contraindications and cautions | Mechanism of action | Adverse effects | Cost* |
|---|---|---|---|---|---|---|---|
| First-line agent | |||||||
| Oxytocin (Pitocin) | Prevention: 10 IU IM or 5 to 10 IU IV bolus | + | + | Overdose or prolonged use can cause water intoxication | Stimulates the upper segment of the myometrium to contract rhythmically, constricting spiral arteries and decreasing blood flow through the uterus | Rare | $1 ($13) for 10 units of injectable solution |
| Treatment: 20 to 40 IU in 1 L normal saline, infuse 500 mL over 10 minutes then 250 mL per hour | Possible hypotension with IV use following cesarean delivery | ||||||
| Second-line agents | |||||||
| Carboprost (Hemabate), a prostaglandin F2-alpha analogue | 250 mcg IM or into myometrium, repeated every 15 to 90 minutes for a total dose of 2 mg | – | + | Avoid in patients with asthma or significant renal, hepatic, or cardiac disease | Improves uterine contractility by increasing the number of oxytocin receptors and causes vasoconstriction | Nausea, vomiting, and diarrhea | NA ($270) for 250 mcg of injectable solution |
| Methylergonovine (Methergine) | 0.2 mg IM, repeat every two to four hours | – | + | Avoid in hypertensive disorders of pregnancy, including chronic hypertension | Causes vasoconstriction and contracts smooth muscles and upper and lower Segments of the uterus tetanically | Nausea, vomiting, and increased blood pressure | $9 (NA) for 0.2 mg of injectable solution |
| Use with caution in patients with human immunodeficiency virus infection who are receiving protease inhibitors | |||||||
| Misoprostol (Cytotec),† a prostaglandin E1 analogue | Prevention: 600 mcg orally Treatment: 800 to 1,000 mcg rectally or 600 to 800 mcg sublingually or orally | Use only when oxytocin is not available | + | Use with caution in patients with cardiovascular disease | Causes generalized smooth muscle contraction | Nausea, vomiting, diarrhea, pyrexia, and shivering | $1 ($5) per 200-mcg tablet |
| Tranexamic acid (Cyklokapron)† | 1 g intravenously over 10 minutes, may be repeated after 30 minutes | – | + | Use within three hours of onset of bleeding
Use with caution in patients with renal impairment and with other clotting factors such as prothrombin complex concentrate |
Inhibits breakdown of fibrin and fibrinogen by plasmin | May increase risk of thrombosis and cause visual defects | $24 ($50) |
Footnotes:
*—Estimated retail price. Generic price listed first; brand price listed in parentheses.
†—Misoprostol is not approved by the U.S. Food and Drug Administration (FDA) for use in prevention or treatment of postpartum hemorrhage.
Abbreviations: IM = intramuscularly; IV = intravenous; NA = not available.
[Source 56) ]What happens if I continue to bleed very heavily?
If heavy bleeding continues and you have lost more than 1000 ml (two pints) of blood, a team of senior hospital staff will be involved in your care.
Medications may be given as an injection or via the back passage to help stop the bleeding. You will be given oxygen via a facemask and a second drip for extra intravenous fluids. You may be given a blood transfusion or medication to help your blood to clot.
If the bleeding continues, you may be taken to the operating theatre to find the cause of the hemorrhage. You will need an anaesthetic for this. Your partner will be kept informed about how you are and what is happening, and your baby will be cared for.
There are several procedures your doctors might use to control the bleeding:
- A ‘balloon’ may be inserted into your womb to put pressure on the bleeding blood vessels. This is usually removed the following day.
- An abdominal operation (laparotomy) may be performed to stop the bleeding.
- Very occasionally, a hysterectomy (removal of the womb) is necessary to control the heavy bleeding.
- In some situations, a procedure called uterine artery embolization may be performed to help stop the bleeding. This procedure is done by a specially trained radiologist (X-ray doctor). It involves injecting small particles via a thin tube (catheter) under X-ray guidance to block the blood supply to the womb.
Once your bleeding is under control, you will either be transferred back to the labour ward or you may be transferred to an intensive care or high-dependency unit. You will be monitored closely until you are well enough to go to the postnatal ward.
Ongoing or Severe Hemorrhage
Significant blood loss from any cause requires immediate resuscitation measures using an interdisciplinary, stage-based team approach. Physicians should perform a primary maternal survey and institute care based on American Heart Association standards and an assessment of blood loss 57). Patients should be given oxygen, ventilated as needed, and provided intravenous fluid and blood replacement with normal saline or other crystalloid fluids administered through two large-bore intravenous needles. Fluid replacement volume should initially be given as a bolus infusion and subsequently adjusted based on frequent reevaluation of the patient’s vital signs and symptoms. The use of O negative blood may be needed while waiting for type-specific blood.
Elevating the patient’s legs will improve venous return. Draining the bladder with a Foley catheter may improve uterine atony and will allow monitoring of urine output. Massive transfusion protocols to decrease the risk of dilutional coagulopathy and other postpartum hemorrhage complications have been established. These protocols typically recommend the use of four units of fresh frozen plasma and one unit of platelets for every four to six units of packed red blood cells used 58).
Uterus-conserving treatments include uterine packing (plain gauze or gauze soaked with vasopressin, chitosan, or carboprost [Hemabate]), artery ligation, uterine artery embolization, B-lynch compression sutures, and balloon tamponade 59). Balloon tamponade (in which direct pressure is applied to potential bleeding sites via a balloon that is inserted through the vagina and cervix and inflated with sterile water or saline), uterine packing, aortic compression, and nonpneumatic antishock garments may be used to limit bleeding while definitive treatment or transport is arranged 60). Hysterectomy is the definitive treatment in women with severe, intractable hemorrhage.
Follow-up of postpartum hemorrhage includes monitoring for ongoing blood loss and vital signs, assessing for signs of anemia (fatigue, shortness of breath, chest pain, or lactation problems), and debriefing with patients and staff. Many patients experience acute and posttraumatic stress disorders after a traumatic delivery. Individual, trauma-focused cognitive behavior therapy can be offered to reduce acute traumatic stress symptoms 61).
References [ + ]





{kind=link}