
Contents
- Trouble getting pregnant
- Having trouble getting pregnant with second baby
- What is Unexplained infertility
- Good fertility health
- Infertility signs and symptoms
- Causes of infertility
- Infertility Prevention
- Infertility diagnosis
- Infertility treatment
- Female infertility
- Female infertility causes
- Disruption of ovarian function (presence or absence of ovulation (anovulation) and effects of ovarian “age”)
- Fallopian tube obstruction (whether fallopian tubes are open, blocked, damaged or swollen)
- Abnormal uterine contour (physical characteristics of the uterus)
- Uterine or cervical causes
- Other causes in women include:
- Smoking and female fertility
- Sexually transmitted infections (STIs)
- Types of Sexually transmitted infections (STIs)
- Risk factors for infertility in women
- Prevention of infertility in women
- Diagnosis of female infertility
- Female infertility causes
- Male infertility
Trouble getting pregnant
Trouble getting pregnant, difficulty conceiving is also known as infertility, which is usually defined as not being able to get pregnant after 12 months of unprotected sexual intercourse. A broader view of infertility includes not being able to carry a pregnancy to term. Finding out that you or your partner are unable to fall pregnant can be upsetting and difficult to deal with.
Because fertility in women is known to decline steadily with age, some health providers evaluate and treat women aged 35 years or older after just 6 months of unprotected sex. Women with infertility should consider making an appointment with a reproductive endocrinologist—a doctor who specializes in managing infertility. Reproductive endocrinologists may also be able to help women with recurrent pregnancy loss, defined as having two or more spontaneous miscarriages.
Pregnancy is the result of a process that has many steps.
To get pregnant:
- A woman’s body must release an egg from one of her ovaries (ovulation).
- A man’s sperm must join with the egg along the way (fertilize).
- The fertilized egg must go through a fallopian tube toward the uterus (womb).
- The fertilized egg must attach to the inside of the uterus (implantation).
Infertility may result from a problem with any or several of these steps.
Impaired fecundity (the ability to produce new offspring or fertility) is a condition related to infertility and refers to women who have difficulty getting pregnant or carrying a pregnancy to term.
- About 6% of married women aged 15 to 44 years in the United States are unable to get pregnant after one year of trying (infertility). Also, about 12% of women aged 15 to 44 years in the United States have difficulty getting pregnant or carrying a pregnancy to term, regardless of marital status (impaired fecundity).
- Infertility is not always a woman’s problem. Both men and women can contribute to infertility. Many couples struggle with infertility and seek help to become pregnant, but it is often thought of as only a woman’s condition. However, in about 35% of couples with infertility, a male factor is identified along with a female factor. In about 8% of couples with infertility, a male factor is the only identifiable cause.
- Almost 9% of men aged 25 to 44 years in the United States reported that they or their partner saw a doctor for advice, testing, or treatment for infertility during their lifetime.
For couples trying for a baby, it is normal to have feelings of uncertainty, disappointment and anxiety. It may affect a couple the same way or in different ways.
It is good to talk through any problems, and have both of you talk about how you feel.
If there are difficulties between you, talk to your doctor as a couple. Your doctor may refer you both to a counsellor if necessary.
There are many causes of infertility. For about 4 couples in 10 it will relate to a sperm problem. In another 4 couples in 10 there will be a female reproductive cause. Sometimes there is a combination of factors.
Infertility in women, your fertility may depend on:
- your age
- if you have any problems with your fallopian tubes
- if you have endometriosis or an ovulation problem
- any uterine fibroids
- pelvic inflammatory disease or sexually transmitted infections (STI).
Infertility in men may be affected by:
- problems with the tubes connected to the testes
- low sperm production
- high numbers of abnormal sperm
- genetic problems
- problems with sperm DNA.
Treatment for infertility is available and can bring hope to people wanting to have a baby, but it also has financial, physical and emotional costs. And success is not guaranteed.
Most experts suggest at least one year for women younger than age 35. However, for women aged 35 years or older, couples should see a health care provider after 6 months of trying unsuccessfully. A woman’s chances of having a baby decrease rapidly every year after the age of 30.
If you’re older than 40, your doctor may want to begin testing or treatment right away.
Your doctor may also want to begin testing or treatment right away if you or your partner has known fertility problems, or if you have a history of irregular or painful periods, pelvic inflammatory disease, repeated miscarriages, prior cancer treatment, or endometriosis.
Some health problems also increase the risk of infertility. So, couples with the following signs or symptoms should not delay seeing their health care provider when they are trying to become pregnant:
- Irregular periods or no menstrual periods.
- Very painful periods.
- Endometriosis.
- Pelvic inflammatory disease.
- You’ve had multiple miscarriages.
- You have known fertility problems.
- You’ve been diagnosed with endometriosis.
- You’ve undergone treatment for cancer
- Suspected male factor (i.e., history of testicular trauma, hernia surgery, chemotherapy, or infertility with another partner).
It is a good idea for any woman and her partner to talk to a health care provider before trying to get pregnant. They can help you get your body ready for a healthy baby, and can also answer questions on fertility and give tips on conceiving.
Having trouble getting pregnant with second baby
Secondary infertility is the inability to become pregnant or to carry a baby to term after previously giving birth to a baby. Secondary infertility shares many of the same causes of primary infertility.
Among the possible causes of secondary infertility are:
- Impaired sperm production, function or delivery in men
- Fallopian tube damage, ovulation disorders, endometriosis and uterine conditions in women
- Complications related to prior pregnancy or surgery
- Risk factor changes for you or your partner, such as age, weight and use of certain medications
If you have frequent, unprotected sex but don’t become pregnant — after a year if you’re younger than 35 or after six months if you’re 35 or older — talk to your health care provider.
Depending on the circumstances, both you and your partner might need medical evaluations. Your doctor can help determine whether there’s an issue that requires a specialist or treatment at a fertility clinic.
Secondary infertility can be surprising and stressful. Don’t try to cope alone. Seek support from your partner, family and friends as you talk to your health care provider about the next steps.
What is Unexplained infertility
Sometimes, the cause of infertility is never found. A combination of several minor factors in both partners could cause unexplained fertility problems. Although it’s frustrating to get no specific answer, this problem may correct itself with time. But, you shouldn’t delay treatment for infertility.
Good fertility health
Your age and your health can affect your chances of falling pregnant. Maintaining a healthy lifestyle may help you improve your fertility.
Age and fertility
When it comes to fertility, age matters. Many people today wait until they’re older to have children. But fertility declines over time, and you should consider this if you plan to have children later. Both women and men are most fertile in their early twenties.
In women, fertility declines more quickly with age. This decline becomes rapid after the age of 35. There are a number of reasons, but particularly the decline in the quality of the eggs released by the ovaries. Around one-third of couples in which the woman is over the age of 35 have fertility problems. This rises to two-thirds when the woman is over 40.
Women over 35 are also less likely to become pregnant as a result of fertility treatments, including IVF, and are more likely to have a miscarriage if they do become pregnant. Men’s fertility gradually declines from around the age of 40, but most men are able to father children into their 50s and beyond.
Avoid Sexually transmitted infections (STIs)
Sexually transmitted infections are sometimes called sexually transmitted diseases (STDs), such as chlamydia and gonorrhoea, can damage a woman’s fallopian tubes, which may make it more difficult to become pregnant. If you think you might have contracted an sexually transmitted infection (STI), go to your doctor or a sexual health clinic.
Sexually transmitted infections (STIs) are passed from one person to another through intimate physical contact – such as heavy petting – and from sexual activity including vaginal, oral, and anal sex. Sexually transmitted infections (STIs) are very common. In fact, the Centers for Disease Control and Prevention 1) estimates 20 million new infections occur every year in the United States. Sexually transmitted diseases (STDs) can mostly be prevented by not having sex. If you do have sex, you can lower your risk by using condoms and being in a sexual relationship with a partner who does not have an STD. Sexually transmitted infections (STIs) do not always cause symptoms, so it is possible to have an infection and not know it. That is why it is important to get tested if you are having sex. If you are diagnosed with an STD, know that all can be treated with medicine and some can be cured entirely.
There are dozens of sexually transmitted infections (STIs). Some sexually transmitted diseases (STDs), such as syphilis, gonorrhea, and chlamydia, are spread mainly by sexual contact. Other diseases, including Zika and Ebola, can be spread sexually but are more often spread through ways other than sex.
Be a healthy weight
Being underweight or overweight can lower your chances of conceiving. One cause of infertility is polycystic ovary syndrome (PCOS), which is made worse by being overweight or obese. Small reductions in weight can assist with fertility, so if you are above a healthy weight, weight management and physical activity is the first treatment option. Even a 5-10% loss of weight has been shown to greatly improve the chances of becoming pregnant 2). Nutrition and exercise will play an important role in weight management.
Research 3) shows that obesity is associated with increased production of androgens in adult women and during late female puberty or adolescence. Androgens are often called “male hormones” because males’ bodies make more of them than do women’s bodies, but both males and females need certain levels of androgens for normal health. Changes in hormone levels, including increases in androgens, can disrupt female reproductive cycles and lead to infertility.
In a research funded by the Reproductive Sciences Branch, investigators studied whether obesity prior to and during early puberty also increased androgen hormone production. Researchers compared androgen levels in normal-weight and obese girls between ages 8 and 14 years. Girls who were obese had higher androgen levels throughout puberty compared with normal-weight girls. The results of this study 4) demonstrate that childhood obesity affects normal hormone production and that these early hormone level changes could influence fertility later in life.
Drink sensibly
The government advises that for women planning a pregnancy, not drinking alcohol is the safest option. This is because no studies have found a safe level of alcohol consumption during pregnancy and many women don’t know exactly when they become pregnant.
Men who exceed 3 to 4 units of alcohol a day may damage their sperm.
Avoid Smoking
Cigarette smoking affects men and women’s fertility and reproductive hormones. Research has implicated cigarette smoking in lower fertility in women, specifically in delayed conception, but the reason that this occurs is unknown. In another analysis of data from the BioCycle Study 5), researchers examined the effect of cigarette smoking on women’s reproductive health. Researchers measured women’s reproductive hormones, including estradiol, progesterone, follicle-stimulating hormone (FSH), and luteinizing hormone (LH), across the menstrual cycle. The levels of these hormones, which vary during the menstrual cycle, are critical for a woman’s reproductive health. In the study, researchers found that smokers had abnormal increases in FSH and LH. High levels of these hormones are common during menopause and are associated with reduced fertility. This research points to a possible explanation for the adverse effect of smoking on women’s fertility and reproductive health 6).
Keep your testicles cool
A man’s testicles should be one or two degrees cooler than the rest of their body. Tight underwear, hot showers and hot baths can all raise the temperature of the testicles.
Avoid radiation and dangerous chemicals
Exposure to radiation and chemicals such as glycol solvents, found in some paints, can damage fertility.
Infertility signs and symptoms
The main symptom of infertility is not getting pregnant. There may be no other outward signs or symptoms. Sometimes, an infertile woman may have irregular or absent menstrual periods. A menstrual cycle that’s too long (35 days or more), too short (less than 21 days), irregular or absent can mean that you’re not ovulating. Rarely, an infertile man may have some signs of hormonal problems, such as changes in hair growth or sexual function.
However, most couples will eventually conceive, with or without treatment.
Causes of infertility
There are many causes of infertility.
Sometimes it is a problem with the woman, sometimes with the man, sometimes with both and sometimes there is no obvious reason for it.
All of the steps during ovulation and fertilization need to happen correctly in order to get pregnant. Sometimes the issues that cause infertility in couples are present at birth, and sometimes they develop later in life.
Infertility causes can affect one or both partners. In general:
- In about one-third of cases, there is an issue with the male.
- In about one-third of cases, there is an issue with the female.
- In the remaining cases, there are issues with both the male and female, or no cause can be identified.
For example, a woman may have:
- hormonal disorders
- damaged or blocked fallopian tubes
- endometriosis
- very thick cervical mucus.
A man may have:
- low sperm count
- poor sperm movement or shape
- no sperm released due to an obstruction, or ejaculation failure.
Age is an important factor. From the age of 32, a woman’s chances of conceiving start to decrease, and from age 35, the rate of that decrease speeds up. Men aged 35 are half as fertile as they were at the age of 25, and from the age of 55, their fertility declines dramatically.
Your weight will also affect your fertility. Both women and men who are overweight have changes to their hormones that make it harder for them to be fertile.
Smokers are more likely to be infertile than non-smokers.
The more alcohol men and women drink, the less likely is a successful pregnancy.
Some sexually transmitted infections such as chlamydia and gonorrhea can reduce fertility in both men and women.
Infertility Prevention
Some types of infertility aren’t preventable. But several strategies may increase your chances of pregnancy.
Couples
Have regular intercourse several times around the time of ovulation for the highest pregnancy rate. Having intercourse beginning at least 5 days before and until a day after ovulation improves your chances of getting pregnant. Ovulation usually occurs at the middle of the cycle — halfway between menstrual periods — for most women with menstrual cycles about 28 days apart.
Men
For men, although most types of infertility aren’t preventable, these strategies may help:
- Avoid drug and tobacco use and excessive alcohol consumption, which may contribute to male infertility.
- Avoid high temperatures, as this can affect sperm production and motility. Although this effect is usually temporary, avoid hot tubs and steam baths.
- Avoid exposure to industrial or environmental toxins, which can impact sperm production.
- Limit medications that may impact fertility, both prescription and nonprescription drugs. Talk with your doctor about any medications you take regularly, but don’t stop taking prescription medications without medical advice.
- Exercise moderately. Regular exercise may improve sperm quality and increase the chances for achieving a pregnancy.
Women
For women, a number of strategies may increase the chances of becoming pregnant:
- Quit smoking. Tobacco has multiple negative effects on fertility, not to mention your general health and the health of a fetus. If you smoke and are considering pregnancy, quit now.
- Avoid alcohol and street drugs. These substances may impair your ability to conceive and have a healthy pregnancy. Don’t drink alcohol or use recreational drugs, such as marijuana or cocaine.
- Limit caffeine. Women trying to get pregnant may want to limit caffeine intake. Ask your doctor for guidance on the safe use of caffeine.
- Exercise moderately. Regular exercise is important, but exercising so intensely that your periods are infrequent or absent can affect fertility.
- Avoid weight extremes. Being overweight or underweight can affect your hormone production and cause infertility.
Infertility diagnosis
You and your partner will both need investigations to work out what the cause may be. Sometimes, the problem lies with the woman. Sometimes with the man. Sometimes with both. And sometimes, no cause is ever found.
If your doctor suspects there is a reason you have not fallen pregnant, there are a number of tests that can be done to determine your fertility and that of your partner. Your doctor can refer you for these tests, which will usually happen in hospital or at a fertility clinic.
Before infertility testing, your doctor or clinic works to understand your sexual habits and may make recommendations based on these. In some infertile couples, no specific cause is found (unexplained infertility).
- Infertility evaluation can be expensive, and sometimes involves uncomfortable procedures. Many medical plans may not reimburse the cost of fertility treatment. Finally, there’s no guarantee — even after all the testing and counseling — that you’ll get pregnant.
Tests for men
Male fertility requires that the testicles produce enough healthy sperm, and that the sperm is ejaculated effectively into the woman’s vagina and travels to the egg. Tests for male infertility attempt to determine whether any of these processes are impaired.
You may have a general physical exam, including examination of your genitals. Specific fertility tests may include:
- Semen analysis. Your doctor may ask for one or more semen specimens. Semen is generally obtained by masturbating or by interrupting intercourse and ejaculating your semen into a clean container. A lab analyzes your semen specimen. In some cases, sperm may be tested for in the urine.
- Hormone testing. You may have a blood test to determine the level of testosterone and other male hormones.
- Genetic testing. Genetic testing may be done to determine whether there’s a genetic defect causing infertility.
- Testicular biopsy. In select cases, a testicular biopsy may be performed to identify abnormalities contributing to infertility and to retrieve sperm to use with assisted reproductive techniques, such as IVF.
- Imaging. In certain situations, imaging studies such as a brain MRI, bone mineral density scan, transrectal or scrotal ultrasound, or a test of the vas deferens (vasography) may be performed.
- Other specialty testing. In rare cases, other tests to evaluate the quality of the sperm may be performed, such as evaluating a semen specimen for DNA abnormalities.
Sperm test
In up to half of cases, fertility problems are due to the male partner. Sometimes a lack of sperm or sperm that are not moving properly can cause a failure to conceive.
Your doctor can arrange a sperm test. The male partner will be asked to produce a sperm sample and take it for analysis, probably at your local hospital or a pathology laboratory.
Tests for women
Fertility for women relies on the ovaries releasing healthy eggs. Her reproductive tract must allow an egg to pass into her fallopian tubes and join with sperm for fertilization. The fertilized egg must travel to the uterus and implant in the lining. Tests for female infertility attempt to determine whether any of these processes are impaired.
You may have a general physical exam, including a regular gynecological exam. Specific fertility tests may include:
- Ovulation testing. A blood test measures hormone levels to determine whether you’re ovulating.
- Hysterosalpingography. Hysterosalpingography evaluates the condition of your uterus and fallopian tubes and looks for blockages or other problems. X-ray contrast is injected into your uterus, and an X-ray is taken to determine if the cavity is normal and ensure the fluid spills out of your fallopian tubes.
- Ovarian reserve testing. This testing helps determine the quality and quantity of the eggs available for ovulation. This approach often begins with hormone testing early in the menstrual cycle.
- Other hormone testing. Other hormone tests check levels of ovulatory hormones, as well as pituitary hormones that control reproductive processes.
- Imaging tests. Pelvic ultrasound looks for uterine or fallopian tube disease. Sometimes a hysterosonography (his-tur-o-suh-NOG-ruh-fee) is used to see details inside the uterus that are not seen on a regular ultrasound.
Depending on your situation, rarely your testing may include:
- Hysteroscopy. Based on your symptoms, your doctor may request a hysteroscopy to look for uterine or fallopian tube disease. During hysteroscopy, your doctor inserts a thin, lighted device through your cervix into your uterus to view any potential abnormalities.
- Laparoscopy. This minimally invasive surgery involves making a small incision beneath your navel and inserting a thin viewing device to examine your fallopian tubes, ovaries and uterus. A laparoscopy may identify endometriosis, scarring, blockages or irregularities of the fallopian tubes, and problems with the ovaries and uterus.
- Genetic testing. Genetic testing helps determine whether there’s a genetic defect causing infertility.
Not everyone needs to have all, or even many, of these tests before the cause of infertility is found. You and your doctor will decide which tests you will have and when.
Blood tests to check ovulation
Levels of hormones in a woman’s blood are closely linked to ovulation, when the ovaries release an egg into the fallopian tubes. Hormone imbalances can cause ovulation problems, and a blood test can help determine whether this is happening.
Going through a phase of not having periods, or having irregular periods, are also signs of ovulation problems. The most common cause of ovulation problems is polycystic ovary syndrome.
Test for Sexually transmitted infections (STIs)
Chlamydia is the most common sexually transmitted infection STI in the US. It can cause pelvic inflammatory disease and fertility problems. Your doctor can refer you for a test for chlamydia. This can be a urine test or a swab from the urethra (the tube from which urine passes) or the neck of the cervix.
Ultrasound scan
An ultrasound scan can be carried out to check the woman’s ovaries, womb and fallopian tubes. In a transvaginal ultrasound scan a small ultrasound probe is placed in the vagina. This scan can help doctors check the health of your ovaries and womb.
Certain conditions that can affect the womb, such as endometriosis and fibroids, can prevent pregnancy from occurring. The scan can also check for blockages in your fallopian tubes (the tubes that connect the ovaries and the womb), which may be stopping eggs from travelling along the tubes and into the womb.
X-ray of fallopian tubes
This is called a ‘hysterosalpingogram’ (HSG). Opaque dye is injected through the cervix while you have an X-ray. The dye will help your doctors to see if there are any blockages in your fallopian tubes. Blockages can prevent eggs passing down the tubes to the womb, and stop pregnancy occurring.
Laparoscopy
If you have a known pelvic problem, such as pelvic inflammatory disease (PID) or endometriosis, laparoscopy (keyhole surgery) may be done. This involves making a small cut in your abdomen so a thin tube with a camera (laparoscope) can be used to examine your womb, fallopian tubes and ovaries.
Infertility treatment
Infertility treatment depends on:
- What’s causing the infertility
- How long you’ve been infertile
- Your age and your partner’s age
- Personal preferences
If you are infertile and want to have a child, there are many options. There are a number of fertility treatments that are available to both of you.
Some causes of infertility can’t be corrected.
You may increase your chance of falling pregnant if you know your most fertile days.
In cases where spontaneous pregnancy doesn’t happen, couples can often still achieve a pregnancy through use of assisted reproductive technology like in vitro fertilisation (IVF). Infertility treatment may involve significant financial, physical, psychological and time commitments.
Treatment for men
Men’s options can include treatment for general sexual problems or lack of healthy sperm. Treatment may include:
- Altering lifestyle factors. Improving lifestyle and behavioral factors can improve chances for pregnancy, including discontinuing select medications, reducing/eliminating harmful substances, improving frequency and timing of intercourse, establishing regular exercise, and optimizing other factors that may otherwise impair fertility.
- Medications. Certain medications may improve a man’s sperm count and likelihood for achieving a successful pregnancy. These medicines may increase testicular function, including sperm production and quality.
- Surgery. In select conditions, surgery may be able to reverse a sperm blockage and restore fertility. In other cases, surgically repairing a varicocele may improve overall chances for pregnancy.
- Sperm retrieval. These techniques obtain sperm when ejaculation is a problem or when no sperm are present in the ejaculated fluid. They may also be used in cases where assisted reproductive techniques are planned and sperm counts are low or otherwise abnormal.
Treatment for women
Although a woman may need just one or two therapies to restore fertility, it’s possible that several different types of treatment may be needed before she’s able to conceive.
- Stimulating ovulation with fertility drugs. Fertility drugs are the main treatment for women who are infertile due to ovulation disorders. These medications regulate or induce ovulation. Talk with your doctor about fertility drug options — including the benefits and risks of each type.
- Intrauterine insemination (IUI). During IUI, healthy sperm are placed directly in the uterus around the time the woman’s ovary releases one or more eggs to be fertilized. Depending on the reasons for infertility, the timing of IUI can be coordinated with your normal cycle or with fertility medications.
- Surgery to restore fertility. Uterine problems such as endometrial polyps, a uterine septum or intrauterine scar tissue can be treated with hysteroscopic surgery.
Ovulation induction
Ovulation induction is designed to stimulate the ovary to increase egg production. Ovulation induction uses tablets or injections over a period of time. Ultrasounds and blood tests are performed to determine the best time to trigger ovulation using a hormone called HCG. Once ovulation has been triggered, semen is introduced either by sexual intercourse or intra-uterine insemination when collected semen is placed directly into the uterus through the cervix.
Ovulation induction is not recommended for women who have a BMI greater than 35.
Clomiphene citrate
Clomiphene (Clomid) is a tablet that is the most common medication used in US for ovulation induction. It is often recommended as the first option for improving fertility in women with polycystic ovary syndrome (PCOS) who are infertile and do not ovulate.
Metformin
Metformin can be used for treating infertility in women with PCOS who don’t ovulate and who have no other reasons for infertility.
Gonadotrophins
Gonadotrophins are hormones involved in regulating ovulation such as:
- follicle–stimulating hormone (FSH)
- luteinsing hormone (LH)
- human chorionic gonadotrophin (hCG)
Surgery for improving fertility
Ovarian drilling
A surgical procedure that may increase ovulation in PCOS. It is a minimally invasive procedure where an incision is made in the abdomen under a general anaesthetic and via the laparoscope small holes are drilled in the surface of the ovary. Following ovarian drilling, ovulation is often restored for up to 6-12 months.
As surgery is a more intensive treatment than taking medication or lifestyle treatment, ovarian drilling is not commonly used and is mostly used after other lifestyle or medical treatment has not helped.
Tubal surgery with microsurgery to unblock tubes
It is rare these days because of assisted reproductive technologies (ART).
Hydrotubation
Putting dye through the fallopian tube either under anesthetic or during ultrasound.
Assisted reproductive technology (ART)
For women who have not been able to conceive naturally or by using medications or lifestyle treatment to improve their fertility, another option is assisted reproductive technology. This includes treatments such as in vitro fertilization (IVF). Referral to a fertility specialist is necessary for these treatments.
Assisted reproductive technology is any fertility treatment in which the egg and sperm are handled. An assisted reproductive technology health team includes physicians, psychologists, embryologists, lab technicians, nurses and allied health professionals who work together to help infertile couples achieve pregnancy.
In vitro fertilization (IVF) is the most common assisted reproductive technology technique. In vitro fertilization (IVF) involves stimulating and retrieving multiple mature eggs from a woman, fertilizing them with a man’s sperm in a dish in a lab, and implanting the embryos in the uterus three to five days after fertilization.
Other techniques are sometimes used in an IVF cycle, such as:
- Intracytoplasmic sperm injection. A single healthy sperm is injected directly into a mature egg. Intracytoplasmic sperm injection is often used when there is poor semen quality or quantity, or if fertilization attempts during prior IVF cycles failed.
- Assisted hatching. This technique assists the implantation of the embryo into the lining of the uterus by opening the outer covering of the embryo (hatching).
- Donor eggs or sperm. Most assisted reproductive technology is done using the woman’s own eggs and her partner’s sperm. However, if there are severe problems with either the eggs or sperm, you may choose to use eggs, sperm or embryos from a known or anonymous donor.
- Gestational carrier. Women who don’t have a functional uterus or for whom pregnancy poses a serious health risk might choose IVF using a gestational carrier. In this case, the couple’s embryo is placed in the uterus of the carrier for pregnancy.
Complications of treatment
Complications of infertility treatment may include:
- Multiple pregnancy. The most common complication of infertility treatment is a multiple pregnancy — twins, triplets or more. Generally, the greater the number of fetuses, the higher the risk of premature labor and delivery, as well as problems during pregnancy such as gestational diabetes. Babies born prematurely are at increased risk of health and developmental problems. Talk to your doctor about ways to prevent a multiple pregnancy before you begin treatment.
- Ovarian hyperstimulation syndrome. Fertility medications to induce ovulation can cause ovarian hyperstimulation syndrome, in which the ovaries become swollen and painful. Symptoms may include mild abdominal pain, bloating and nausea that lasts about a week, or longer if you become pregnant. Rarely, a more severe form causes rapid weight gain and shortness of breath requiring emergency treatment.
- Bleeding or infection. As with any invasive procedure, there is a rare risk of bleeding or infection with assisted reproductive technology.
Coping and support
Coping with infertility can be extremely difficult because there are so many unknowns. The emotional burden on a couple is considerable. Taking these steps can help you cope:
- Be prepared. The uncertainty of infertility testing and treatments can be difficult and stressful. Ask your doctor to explain the steps, and prepare for each
- one.
Set limits. Decide before starting treatment which procedures, and how many, are emotionally and financially acceptable for you and your partner. Fertility treatments may be expensive and often are not covered by insurance companies, and a successful pregnancy often depends on repeated attempts. - Consider other options. Determine alternatives — adoption, donor sperm or egg, donor embryo, gestational carrier or adoption, or even having no children — as early as possible in the infertility evaluation. This may reduce anxiety during treatments and feelings of hopelessness if conception doesn’t occur.
- Seek support. Locate support groups or counseling services for help before and after treatment to help endure the process and ease the grief should treatment fail.
Managing emotional stress during treatment
Try these strategies to help manage emotional stress during treatment:
- Express yourself. Reach out to others rather than repressing guilt or anger.
- Stay in touch with loved ones. Talking to your partner, family and friends can be very beneficial. The best support often comes from loved ones and those closest to you.
- Reduce stress. Some studies have shown that couples experiencing psychological stress had poorer results with infertility treatment. Try to reduce stress in your life before trying to become pregnant.
- Exercise and eat a healthy diet. Keeping up a moderate exercise routine and a healthy diet can improve your outlook and keep you focused on living your life.
Managing emotional effects of the outcome
You’ll face the possibility of psychological challenges no matter your results:
- Not achieving pregnancy, or having a miscarriage. The emotional stress of not being able to have a baby can be devastating even on the most loving and affectionate relationships.
- Success. Even if fertility treatment is successful, it’s common to experience stress and fear of failure during pregnancy. If you have a history of depression or anxiety disorder, you’re at increased risk of these problems recurring in the months after your child’s birth.
- Multiple births. A successful pregnancy that results in multiple births introduces medical complexities and the likelihood of significant emotional stress both during pregnancy and after delivery.
Seek professional help if the emotional impact of the outcome of your fertility treatments becomes too heavy for you or your partner.
Female infertility
Doctors call infertility if a woman is not pregnant after 12 months or more of regular unprotected sex.
Infertility is common. Whether you are trying to fall pregnant for the first time, or are already parents who would like more children, infertility can be a stressful and frustrating experience for everyone involved.
Women need functioning ovaries, fallopian tubes and a uterus to get pregnant. Conditions affecting any one of these organs can contribute to female infertility. Some of these conditions are listed below and can be evaluated using a number of different tests. There is also plenty you can do to prevent infertility.
Female infertility causes
There are many causes of infertility.
Sometimes it is a problem with the woman, sometimes with the man, sometimes with both and sometimes there is no obvious reason for it (unexplained infertility).
Each of these factors is essential to become pregnant:
- You need to ovulate. To get pregnant, your ovaries must produce and release an egg, a process known as ovulation. Your doctor can help evaluate your menstrual cycles and confirm ovulation.
- Your partner needs sperm. For most couples, this isn’t a problem unless your partner has a history of illness or surgery. Your doctor can run some simple tests to evaluate the health of your partner’s sperm.
- You need to have regular intercourse. You need to have regular sexual intercourse during your fertile time. Your doctor can help you better understand when you’re most fertile.
- You need to have open fallopian tubes and a normal uterus. The egg and sperm meet in the fallopian tubes, and the embryo needs a healthy uterus in which to grow.
For pregnancy to occur, every step of the human reproduction process has to happen correctly. The steps in this process are:
- One of the two ovaries releases a mature egg.
- The egg is picked up by the fallopian tube.
- Sperm swim up the cervix, through the uterus and into the fallopian tube to reach the egg for fertilization.
- The fertilized egg travels down the fallopian tube to the uterus.
- The fertilized egg implants and grows in the uterus.
In women, a number of factors can disrupt this process at any step. Female infertility is caused by one or more of the factors below.
For example, a woman may have:
- hormonal disorders
- damaged or blocked fallopian tubes
- endometriosis
- very thick cervical mucus.
A man may have:
- low sperm count
- poor sperm movement or shape
- no sperm released due to an obstruction, or ejaculation failure.
Age is an important factor. From the age of 32, a woman’s chances of conceiving start to decrease, and from age 35, the rate of that decrease speeds up. Men aged 35 are half as fertile as they were at the age of 25, and from the age of 55, their fertility declines dramatically.
Your weight will also affect your fertility. Both women and men who are overweight have changes to their hormones that make it harder for them to be fertile.
Smokers are more likely to be infertile than non-smokers.
The more alcohol men and women drink, the less likely is a successful pregnancy.
Some sexually transmitted infections such as chlamydia and gonorrhea can reduce fertility in both men and women.
Disruption of ovarian function (presence or absence of ovulation (anovulation) and effects of ovarian “age”)
A woman’s menstrual cycle is, on average, 28 days long. Day 1 is defined as the first day of “full flow.” Regular predictable periods that occur every 24 to 32 days likely reflect ovulation. A woman with irregular periods is likely not ovulating.
Ovulation can be predicted by using an ovulation predictor kit and can be confirmed by a blood test to check the woman’s progesterone level on day 21 of her menstrual cycle. Although several tests exist to evaluate a woman’s ovarian function, no single test is a perfect predictor of fertility. The most commonly used markers of ovarian function include follicle stimulating hormone (FSH) value on day 3 to 5 of the menstrual cycle, anti-müllerian hormone value (AMH), and antral follicle count (AFC) using a transvaginal ultrasound.
Disruptions in ovarian function may be caused by several conditions and warrants an evaluation by a doctor.
When a woman doesn’t ovulate during a menstrual cycle, it’s called anovulation. Potential causes of anovulation include the following:
- Polycystic ovary syndrome (PCOS). PCOS is a condition that causes women to not ovulate, or to ovulate irregularly. Some women with PCOS have elevated levels of testosterone, which can cause acne and excess hair growth. PCOS is the most common cause of female infertility.
- Diminished ovarian reserve. Women are born with all of the eggs that they will ever have and a woman’s egg count decreases over time. Diminished ovarian reserve is a condition in which there are fewer eggs remaining in the ovaries than normal. The number of eggs a woman has declines naturally as a woman ages. It may also occur due to congenital, medical, surgical, or unexplained causes. Women with diminished ovarian reserve may be able to conceive naturally, but will produce fewer eggs in response to fertility treatments.
- Functional hypothalamic amenorrhea. Functional hypothalamic amenorrhea is a condition caused by excessive exercise, stress, or low body weight. It is sometimes associated with eating disorders such as anorexia.
- Improper function of the hypothalamus and pituitary glands. The hypothalamus and pituitary glands in the brain produce hormones that maintain normal ovarian function. Production of too much of the hormone prolactin by the pituitary gland (often as the result of a benign pituitary gland tumor), or improper function of the hypothalamus or pituitary gland, may cause a woman not to ovulate.
- Premature ovarian insufficiency (early menopause). Premature ovarian insufficiency, sometimes referred to as premature menopause, occurs when a woman’s ovaries stop working and menstruation ends before age 40. Although the cause is often unknown, certain factors are associated with early menopause, including immune system diseases, certain genetic conditions such as Turner syndrome or carriers of Fragile X syndrome, pelvic radiation therapy or chemotherapy treatment, and smoking. About 5% to10% of women with premature ovarian insufficiency conceive naturally and have a normal pregnancy.
- Menopause. Menopause is an age-appropriate decline in ovarian function that usually occurs around age 50. By definition, a woman in menopause has not had a period in one year. She may experience hot flashes, mood changes, difficulty sleeping, and other symptoms as well.
Fallopian tube obstruction (whether fallopian tubes are open, blocked, damaged or swollen)
Risk factors for blocked fallopian tubes (tubal occlusion) or pelvic adhesions can include a history of pelvic infection, history of ruptured appendicitis, history of gonorrhea or chlamydia, known endometriosis, or a history of abdominal surgery.
Tubal evaluation may be performed using an X-ray that is called a hysterosalpingogram or by chromopertubation in the operating room at time of laparoscopy, a surgical procedure in which a small incision is made and a viewing tube called a laparoscope is inserted.
- Hysterosalpingogram is an X-ray of the uterus and fallopian tubes. A radiologist injects dye into the uterus through the cervix and simultaneously takes X-ray pictures to see if the dye moves freely through fallopian tubes. This helps evaluate tubal caliber (diameter) and patency.
- Chromopertubation is similar to an hysterosalpingogram but is done in the operating room at the time of a laparoscopy. Blue-colored dye is passed through the cervix into the uterus and spillage and tubal caliber (shape) is evaluated.
Abnormal uterine contour (physical characteristics of the uterus)
Depending on a woman’s symptoms, the uterus may be evaluated by transvaginal ultrasound to look for fibroids or other anatomic abnormalities. If suspicion exists that the fibroids may be entering the endometrial cavity, a sonohystogram or hysteroscopy may be performed to further evaluate the uterine environment.
Uterine or cervical causes
Several uterine or cervical causes can impact fertility by interfering with implantation or increasing the likelihood of a miscarriage:
- Benign polyps or tumors (fibroids or myomas) are common in the uterus. Some can block fallopian tubes or interfere with implantation, affecting fertility. However, many women who have fibroids or polyps do become pregnant.
- Endometriosis scarring or inflammation within the uterus can disrupt implantation.
Uterine abnormalities present from birth, such as an abnormally shaped uterus, can cause problems becoming or remaining pregnant. - Cervical stenosis, a narrowing of the cervix, can be caused by an inherited malformation or damage to the cervix.
- Sometimes the cervix can’t produce the best type of mucus to allow the sperm to travel through the cervix into the uterus.
Other causes in women include:
- Cancer and its treatment. Certain cancers — particularly female reproductive cancers — often severely impair female fertility. Both radiation and chemotherapy may affect fertility.
- Other conditions. Medical conditions associated with delayed puberty or the absence of menstruation (amenorrhea), such as celiac disease, poorly controlled diabetes and some autoimmune diseases such as lupus, can affect a woman’s fertility. Genetic abnormalities also can make conception and pregnancy less likely.
Smoking and female fertility
Smoking can cause problems for virtually all aspects of the reproductive system. Women who smoke are more likely to have difficulty conceiving, may not respond as well to treatment for infertility, experience earlier menopause and have an increased risk of cervical and vulval cancer. Smoking is associated with an increased risk of infertility, for both women attempting to become pregnant for the first time and women who have previously been pregnant.
Women who smoke also have a poorer response to in vitro fertilisation (IVF). Smokers will also have an increased risk of ectopic pregnancy and miscarriage. Smoking during pregnancy has been linked to a variety of health problems in the baby including premature birth, low birthweight, cot death (also known as sudden infant death syndrome or SIDS) and breathing problems in the first six months of life.
Sexually transmitted infections (STIs)
Sexually transmitted infections (STIs) are sometimes called sexually transmitted diseases (STDs) are infections that can be passed on during sex, and in some cases can be passed from a woman to her baby during pregnancy and childbirth. If left untreated, sexually transmitted infections (STIs) can cause serious problems for both mother and child. If you think you may have an sexually transmitted infection (STI), it’s important to see a doctor.
Sexually transmitted infections (STIs) are caused by micro-organisms such as bacteria, viruses and parasites. These organisms can pass between people in semen, blood or vaginal and other bodily fluids.
Many STIs can also be transmitted by close skin-to-skin contact (for example during foreplay or oral sex), through blood-to-blood contact, and by sharing needles and other equipment for intravenous drug use.
Types of Sexually transmitted infections (STIs)
There are many different types of STIs. The most common STIs in US are:
- chlamydia (a bacterial infection)
- gonorrhea (a bacterial infection)
- syphilis (a bacterial infection)
- genital herpes (a viral infection)
- genital warts/human papilloma virus (HPV) (a viral infection)
- hepatitis B (a viral infection)
- HIV (a viral infection)
- trichomoniasis (a parasite).
There are also a range of infections that, while not strictly classified as STIs, are sometimes linked with sexual activity, such as:
- hepatitis A (a viral infection)
- thrush (a Candida fungal infection)
- bacterial vaginosis (an imbalance of bacteria in the vagina)
- pubic lice or crabs (a parasite)
- scabies (a parasite)
- lymphogranuloma venereum (caused by some types of chlamydia)
- mycoplasma genitalium (a bacterial infection).
Symptoms of Sexually transmitted infections (STIs)
Many people with STIs have no symptoms. They may not know about it until it causes complications or a partner is diagnosed.
Other people get symptoms such as:
- sores or bumps on the genitals, mouth or rectal area
- pain when urinating
- unusual discharge from the penis or vagina
- unusual vaginal bleeding
- pain during sex
- sore, swollen lymph nodes, especially in the groin
- pain in the lower abdomen
- rash on the body, hands or feet.
If you have one or more of these symptoms it doesn’t necessarily mean you have an STI, but it would be wise to see your doctor for a check-up.
Can having an sexually transmitted infection (STI) affect my pregnancy?
Sexually transmitted infections (STIs) can affect your ability to become pregnant (your fertility), as well as your pregnancy. If you are pregnant, or wanting to become pregnant, tested for sexually transmitted infections (STIs) is recommended even if you have been tested in the past. If you have concerns about this, discuss this with your doctor.
Women who are pregnant can get the same STIs as women who are not pregnant. If you get infected with an sexually transmitted infection (STI) while pregnant, it can cause serious problems for you and your developing baby, so if you are worried this is a possibility, discuss getting a check done with your doctor.
If you do contract an STI while pregnant, getting early treatment can reduce the risks. Even if the STI can’t be cured, there are things that can be done to protect you and your baby.
How can Sexually transmitted infections (STIs) affect my baby?
Some STIs, such as syphilis and HIV, can infect a baby while it’s still in the mother’s womb. Others, such as chlamydia and genital herpes, can infect the baby as it is being delivered.
Sexually transmitted infections (STIs) can pose significant health risks to unborn babies. These include:
- premature birth
- low birth weight
- birth defects
- illness
- death.
Getting regular medical care during your pregnancy and discussing any concerns you may have of STIs with your doctor or midwife help reduce the risk of any problems caused by STIs during your pregnancy.
Diagnosis and treatment for Sexually transmitted infections (STIs)
Untreated STIs stay active in the body and may be passed on to sexual partners, or your baby, without you being aware. Therefore, it’s important to get tested if you think you may have an STI.
Having a test for STIs is simple. The type of test depends on the STI, but tests usually involve a providing a urine sample, a swab, a blood test, or a physical examination.
If the test shows you have an STI, you may need further tests and treatment. STIs caused by bacteria, like chlamydia, can usually be treated with antibiotics. Other STIs, such as those caused by viruses (for example herpes), can be managed to control symptoms, but are not always curable.
Tips for avoiding Sexually transmitted infections (STIs)
Other than not having sex with a partner that could potentially have an STI, condoms (used during penetrative sex) and dental dams (used during oral sex) offer the best protection from STIs.
Other ways to avoid STIs are:
- staying with one uninfected partner or not having many sexual partners
- avoiding sex with a new partner until you’ve both been tested for STIs
- getting vaccinated against HPV and hepatitis
- getting circumcised (if you are a man)
- not taking drugs or drinking excessive alcohol (often associated with risk-taking behaviour).
Risk factors for infertility in women
Female fertility is known to decline with:
- Age. More women are waiting until their 30s and 40s to have children. In fact, about 20% of women in the United States now have their first child after age 35. About one-third of couples in which the woman is older than 35 years have fertility problems. Aging not only decreases a woman’s chances of having a baby, but also increases her chances of miscarriage and of having a child with a genetic abnormality.
- Aging decreases a woman’s chances of having a baby in the following ways:
- She has a smaller number of eggs left.
- Her eggs are not as healthy.
- She is more likely to have health conditions that can cause fertility problems.
- She is more likely to have a miscarriage.
- Smoking.
- Excessive alcohol use.
- Being overweight. Among American women, an inactive lifestyle and being overweight may increase the risk of infertility. A man’s sperm count may also be affected if he is overweight.
- Being underweight. Women at risk of fertility problems include those with eating disorders, such as anorexia or bulimia, and women who follow a very low calorie or restrictive diet.
- Excessive physical or emotional stress that results in amenorrhea (absent periods).
Prevention of infertility in women
If you’re a woman thinking about getting pregnant soon or in the future, you may improve your chances of having normal fertility if you:
- Maintain a normal weight. Overweight and underweight women are at increased risk of ovulation disorders. If you need to lose weight, exercise moderately. Strenuous, intense exercise of more than five hours a week has been associated with decreased ovulation.
- Quit smoking. Tobacco has multiple negative effects on fertility, not to mention your general health and the health of a fetus. If you smoke and are considering pregnancy, quit now.
- Avoid alcohol. Heavy alcohol use may lead to decreased fertility. And any alcohol use can affect the health of a developing fetus. If you’re planning to become pregnant, avoid alcohol, and don’t drink alcohol while you’re pregnant.
- Reduce stress. Some studies have shown that couples experiencing psychological stress had poorer results with infertility treatment. If you can, find a way to reduce stress in your life before trying to become pregnant.
- Limit caffeine. Research suggests that limiting caffeine intake to less than 200 milligrams a day shouldn’t affect your ability to get pregnant. That’s about one to two cups of 6 to 8 ounces of coffee per day.
Diagnosis of female infertility
If you’ve been unable to conceive within a reasonable period of time, seek help from your doctor for evaluation and treatment of infertility.
Fertility tests may include:
- Ovulation testing. An at-home, over-the-counter ovulation prediction kit detects the surge in luteinizing hormone (LH) that occurs before ovulation. A blood test for progesterone — a hormone produced after ovulation — can also document that you’re ovulating. Other hormone levels, such as prolactin, also may be checked.
- Hysterosalpingography. During hysterosalpingography (his-tur-o-sal-ping-GOG-ruh-fee), X-ray contrast is injected into your uterus and an X-ray is taken to detect abnormalities in the uterine cavity. The test also determines whether the fluid passes out of the uterus and spills out of your fallopian tubes. If abnormalities are found, you’ll likely need further evaluation. In a few women, the test itself can improve fertility, possibly by flushing out and opening the fallopian tubes.
- Ovarian reserve testing. This testing helps determine the quality and quantity of eggs available for ovulation. Women at risk of a depleted egg supply — including women older than 35 — may have this series of blood and imaging tests.
- Other hormone testing. Other hormone tests check levels of ovulatory hormones as well as thyroid and pituitary hormones that control reproductive processes.
- Imaging tests. A pelvic ultrasound looks for uterine or fallopian tube disease. Sometimes a hysterosonography (his-tur-o-suh-NOG-ruh-fee) is used to see details inside the uterus that can’t be seen on a regular ultrasound.
Depending on your situation, rarely your testing may include:
- Other imaging tests. Depending on your symptoms, your doctor may request a hysteroscopy to look for uterine or fallopian tube disease.
- Laparoscopy. This minimally invasive surgery involves making a small incision beneath your navel and inserting a thin viewing device to examine your fallopian tubes, ovaries and uterus. A laparoscopy may identify endometriosis, scarring, blockages or irregularities of the fallopian tubes, and problems with the ovaries and uterus.
- Genetic testing. Genetic testing helps determine whether there’s a genetic defect causing infertility.
Treatment of female infertility
Infertility treatment depends on the cause, your age, how long you’ve been infertile and personal preferences. Because infertility is a complex disorder, treatment involves significant financial, physical, psychological and time commitments.
Although some women need just one or two therapies to restore fertility, it’s possible that several different types of treatment may be needed.
Treatments can either attempt to restore fertility through medication or surgery, or help you get pregnant with sophisticated techniques.
Fertility restoration: Stimulating ovulation with fertility drugs
Fertility drugs regulate or stimulate ovulation. Fertility drugs are the main treatment for women who are infertile due to ovulation disorders.
Fertility drugs generally work like the natural hormones — follicle-stimulating hormone (FSH) and luteinizing hormone (LH) — to trigger ovulation. They’re also used in women who ovulate to try to stimulate a better egg or an extra egg or eggs. Fertility drugs may include:
- Clomiphene citrate. Clomiphene (Clomid) is taken by mouth and stimulates ovulation by causing the pituitary gland to release more FSH and LH, which stimulate the growth of an ovarian follicle containing an egg.
- Gonadotropins. Instead of stimulating the pituitary gland to release more hormones, these injected treatments stimulate the ovary directly to produce multiple eggs. Gonadotropin medications include human menopausal gonadotropin or hMG (Menopur) and FSH (Gonal-F, Follistim AQ, Bravelle).
- Another gonadotropin, human chorionic gonadotropin (Ovidrel, Pregnyl), is used to mature the eggs and trigger their release at the time of ovulation. Concerns exist that there’s a higher risk of conceiving multiples and having a premature delivery with gonadotropin use.
- Metformin. Metformin (Glucophage, others) is used when insulin resistance is a known or suspected cause of infertility, usually in women with a diagnosis of PCOS. Metformin helps improve insulin resistance, which can improve the likelihood of ovulation.
- Letrozole. Letrozole (Femara) belongs to a class of drugs known as aromatase inhibitors and works in a similar fashion to clomiphene. Letrozole may induce ovulation. However, the effect this medication has on early pregnancy isn’t yet known, so it isn’t used for ovulation induction as frequently as others.
- Bromocriptine. Bromocriptine (Cycloset), a dopamine agonist, may be used when ovulation problems are caused by excess production of prolactin (hyperprolactinemia) by the pituitary gland.
Risks of fertility drugs
Using fertility drugs carries some risks, such as:
- Pregnancy with multiples. Oral medications carry a fairly low risk of multiples (less than 10 percent) and mostly a risk of twins. Your chances increase up to 30 percent with injectable medications. Injectable fertility medications also carry the major risk of triplets or more (higher order multiple pregnancy).
Generally, the more fetuses you’re carrying, the greater the risk of premature labor, low birth weight and later developmental problems. Sometimes adjusting medications can lower the risk of multiples, if too many follicles develop.
- Ovarian hyperstimulation syndrome (OHSS). Injecting fertility drugs to induce ovulation can cause OHSS, which causes swollen and painful ovaries. Signs and symptoms usually go away without treatment, and include mild abdominal pain, bloating, nausea, vomiting and diarrhea.
If you become pregnant, however, your symptoms might last several weeks. Rarely, it’s possible to develop a more-severe form of OHSS that can also cause rapid weight gain, enlarged painful ovaries, fluid in the abdomen and shortness of breath.
- Long-term risks of ovarian tumors. Most studies of women using fertility drugs suggest that there are few if any long-term risks. However, a few studies suggest that women taking fertility drugs for 12 or more months without a successful pregnancy may be at increased risk of borderline ovarian tumors later in life.
Women who never have pregnancies have an increased risk of ovarian tumors, so it may be related to the underlying problem rather than the treatment. Since success rates are typically higher in the first few treatment cycles, re-evaluating medication use every few months and concentrating on the treatments that have the most success appear to be appropriate.
Fertility restoration: Surgery
Several surgical procedures can correct problems or otherwise improve female fertility. However, surgical treatments for fertility are rare these days due to the success of other treatments. They include:
- Laparoscopic or hysteroscopic surgery. These surgeries can remove or correct abnormalities to help improve your chances of getting pregnant. Surgery might involve correcting an abnormal uterine shape, removing endometrial polyps and some types of fibroids that misshape the uterine cavity, or removing pelvic or uterine adhesions.
- Tubal surgeries. If your fallopian tubes are blocked or filled with fluid (hydrosalpinx), your doctor may recommend laparoscopic surgery to remove adhesions, dilate a tube or create a new tubal opening. This surgery is rare, as pregnancy rates are usually better with IVF. For hydrosalpinx, removal of your tubes (salpingectomy) or blocking the tubes close to the uterus can improve your chances of pregnancy with IVF.
Reproductive assistance
The most commonly used methods of reproductive assistance include:
- Intrauterine insemination (IUI). During IUI, millions of healthy sperm are placed inside the uterus close to the time of ovulation.
- Assisted reproductive technology. This involves retrieving mature eggs from a woman, fertilizing them with a man’s sperm in a dish in a lab, then transferring the embryos into the uterus after fertilization. IVF is the most effective assisted reproductive technology. An IVF cycle takes several weeks and requires frequent blood tests and daily hormone injections.
Coping and support
Dealing with female infertility can be physically and emotionally exhausting. To cope with the ups and downs of infertility testing and treatment, consider these strategies:
- Be prepared. The uncertainty of infertility testing and treatments can be difficult and stressful. Ask your doctor to explain the steps for your therapy to help you and your partner prepare. Understanding the process may help reduce your anxiety.
- Seek support. Although infertility can be a deeply personal issue, reach out to your partner, close family members or friends, or a professional for support. Many online support groups allow you to maintain your anonymity while you discuss issues related to infertility.
- Exercise and eat a healthy diet. Keeping up a moderate exercise routine and eating healthy foods can improve your outlook and keep you focused on living your life despite fertility problems.
- Consider other options. Determine alternatives — adoption, donor sperm or egg, or even having no children — as early as possible in the infertility treatment process. This can reduce anxiety during treatments and disappointment if conception doesn’t occur.
Male infertility
Male infertility is due to low sperm production, abnormal sperm function or blockages that prevent the delivery of sperm. Illnesses, injuries, chronic health problems, lifestyle choices and other factors can play a role in causing male infertility.
Not being able to conceive a child can be stressful and frustrating, but a number of male infertility treatments are available.
Symptoms of male infertility
The main sign of male infertility is the inability to conceive a child. There may be no other obvious signs or symptoms. In some cases, however, an underlying problem such as an inherited disorder, hormonal imbalance, dilated veins around the testicle, or a condition that blocks the passage of sperm causes signs and symptoms.
Although most men with male infertility do not notice symptoms other than inability to conceive a child, signs and symptoms associated with male infertility include:
- Problems with sexual function — for example, difficulty with ejaculation or small volumes of fluid ejaculated, reduced sexual desire or difficulty maintaining an erection (erectile dysfunction)
- Pain, swelling or a lump in the testicle area
- Recurrent respiratory infections
- Inability to smell
- Abnormal breast growth (gynecomastia)
- Decreased facial or body hair or other signs of a chromosomal or hormonal abnormality
- Having a lower than normal sperm count (fewer than 15 million sperm per milliliter of semen or a total sperm count of less than 39 million per ejaculate)
Male infertility causes
Male fertility is a complex process. To get your partner pregnant, the following must occur:
- You must produce healthy sperm. Initially, this involves the growth and formation of the male reproductive organs during puberty. At least one of your testicles must be functioning correctly, and your body must produce testosterone and other hormones to trigger and maintain sperm production.
- Sperm have to be carried into the semen. Once sperm are produced in the testicles, delicate tubes transport them until they mix with semen and are ejaculated out of the penis.
- There needs to be enough sperm in the semen. If the number of sperm in your semen (sperm count) is low, it decreases the odds that one of your sperm will fertilize your partner’s egg. A low sperm count is fewer than 15 million sperm per milliliter of semen or fewer than 39 million per ejaculate.
- Sperm must be functional and able to move. If the movement (motility) or function of your sperm is abnormal, the sperm may not be able to reach or penetrate your partner’s egg.
Infertility in men can be caused by different factors and is typically evaluated by a semen analysis. When a semen analysis is performed, the number of sperm (concentration), motility (movement), and morphology (shape) are assessed by a specialist. A slightly abnormal semen analysis does not mean that a man is necessarily infertile. Instead, a semen analysis helps determine if and how male factors are contributing to infertility.
Smoking and male fertility
Research has shown that male smokers have lower sperm quality and count than non-smokers. Smoking can also lead to male erectile dysfunction. Two of the main chemicals in cigarettes are nicotine and carbon monoxide, which narrow the arteries and reduce the blood flow through the body, affecting the blood flow to the penis.
By quitting smoking you reduce the risk of impotence and improve your sperm quality, and are less likely to have delays in falling pregnant or experience infertility.
Disruption of testicular or ejaculatory function
Abnormal sperm production or function due to undescended testicles, genetic defects, health problems such as diabetes or infections such as chlamydia, gonorrhea, mumps or HIV. Enlarged veins in the testes (varicocele) can also affect the quality of sperm.
Problems with the delivery of sperm due to sexual problems, such as premature ejaculation; certain genetic diseases, such as cystic fibrosis; structural problems, such as a blockage in the testicle; or damage or injury to the reproductive organs.
- Varicoceles, a condition in which the veins on a man’s testicles are large and cause them to overheat. The heat may affect the number or shape of the sperm.
- Trauma to the testes may affect sperm production and result in lower number of sperm.
- Unhealthy habits such as heavy alcohol use, smoking, anabolic steroid use, and illicit drug use.
- Use of certain medications and supplements. Testosterone replacement therapy, long-term anabolic steroid use, cancer medications (chemotherapy), certain antifungal medications, some ulcer drugs and certain other medications can impair sperm production and decrease male fertility.
- Cancer treatment involving the use of certain types of chemotherapy, radiation, or surgery to remove one or both testicles
- Medical conditions such as diabetes, cystic fibrosis, certain types of autoimmune disorders, and certain types of infections may cause testicular failure.
- Infection. Some infections can interfere with sperm production or sperm health or can cause scarring that blocks the passage of sperm. These include inflammation of the epididymis (epididymitis) or testicles (orchitis) and some sexually transmitted infections, including gonorrhea or HIV. Although some infections can result in permanent testicular damage, most often sperm can still be retrieved.
- Ejaculation issues. Retrograde ejaculation occurs when semen enters the bladder during orgasm instead of emerging out the tip of the penis. Various health conditions can cause retrograde ejaculation, including diabetes, spinal injuries, medications, and surgery of the bladder, prostate or urethra. Some men with spinal cord injuries or certain diseases can’t ejaculate semen, even though they still produce sperm. Often in these cases sperm can still be retrieved for use in assisted reproductive techniques.
- Antibodies that attack sperm. Anti-sperm antibodies are immune system cells that mistakenly identify sperm as harmful invaders and attempt to eliminate them.
- Tumors. Cancers and nonmalignant tumors can affect the male reproductive organs directly, through the glands that release hormones related to reproduction, such as the pituitary gland, or through unknown causes. In some cases, surgery, radiation or chemotherapy to treat tumors can affect male fertility.
- Undescended testicles. In some males, during fetal development one or both testicles fail to descend from the abdomen into the sac that normally contains the testicles (scrotum). Decreased fertility is more likely in men who have had this condition.
- Hormone imbalances. Infertility can result from disorders of the testicles themselves or an abnormality affecting other hormonal systems including the hypothalamus, pituitary, thyroid and adrenal glands. Low testosterone (male hypogonadism) and other hormonal problems have a number of possible underlying causes.
- Defects of tubules that transport sperm. Many different tubes carry sperm. They can be blocked due to various causes, including inadvertent injury from surgery, prior infections, trauma or abnormal development, such as with cystic fibrosis or similar inherited conditions. Blockage can occur at any level, including within the testicle, in the tubes that drain the testicle, in the epididymis, in the vas deferens, near the ejaculatory ducts or in the urethra.
- Chromosome defects. Inherited disorders such as Klinefelter’s syndrome — in which a male is born with two X chromosomes and one Y chromosome (instead of one X and one Y) — cause abnormal development of the male reproductive organs. Other genetic syndromes associated with infertility include cystic fibrosis, Kallmann’s syndrome and Kartagener’s syndrome.
- Problems with sexual intercourse. These can include trouble keeping or maintaining an erection sufficient for sex (erectile dysfunction), premature ejaculation, painful intercourse, anatomical abnormalities such as having a urethral opening beneath the penis (hypospadias), or psychological or relationship problems that interfere with sex.
- Celiac disease. A digestive disorder caused by sensitivity to gluten, celiac disease can cause male infertility. Fertility may improve after adopting a gluten-free diet.
- Prior surgeries. Certain surgeries may prevent you from having sperm in your ejaculate, including vasectomy, inguinal hernia repairs, scrotal or testicular surgeries, prostate surgeries, and large abdominal surgeries performed for testicular and rectal cancers, among others. In most cases, surgery can be performed to either reverse these blockage or to retrieve sperm directly from the epididymis and testicles.
Hormonal disorders
- Improper function of the hypothalamus or pituitary glands. The hypothalamus and pituitary glands in the brain produce hormones that maintain normal testicular function. Production of too much prolactin, a hormone made by the pituitary gland (often due to the presence of a benign pituitary gland tumor), or other conditions that damage or impair the function of the hypothalamus or the pituitary gland may result in low or no sperm production.
- These conditions may include benign and malignant (cancerous) pituitary tumors, congenital adrenal hyperplasia, exposure to too much estrogen, exposure to too much testosterone, Cushing’s syndrome, and chronic use of medications called glucocorticoids.
Genetic disorders
Genetic conditions such as a Klinefelter’s syndrome, Y-chromosome microdeletion, myotonic dystrophy, and other, less common genetic disorders may cause no sperm to be produced, or low numbers of sperm to be produced.
Some other causes of male infertility include:
- Illicit drug use. Anabolic steroids taken to stimulate muscle strength and growth can cause the testicles to shrink and sperm production to decrease. Use of cocaine or marijuana may temporarily reduce the number and quality of your sperm as well.
- Alcohol use. Drinking alcohol can lower testosterone levels, cause erectile dysfunction and decrease sperm production. Liver disease caused by excessive drinking also may lead to fertility problems.
- Tobacco smoking. Men who smoke may have a lower sperm count than do those who don’t smoke. Secondhand smoke also may affect male fertility.
- Emotional stress. Stress can interfere with certain hormones needed to produce sperm. Severe or prolonged emotional stress, including problems with fertility, can affect your sperm count.
- Weight. Obesity can impair fertility in several ways, including directly impacting sperm themselves as well as by causing hormone changes that reduce male fertility.
Certain occupations including welding or those involving prolonged sitting, such as truck driving, may be associated with a risk of infertility. However, the research to support these links is mixed.
Risk factors for infertility in men
- Age. Although advanced age plays a much more important role in predicting female infertility, couples in which the male partner is 40 years old or older are more likely to report difficulty conceiving.
- Being overweight or obese.
- Smoking.
- Excessive alcohol use.
- Use of marijuana.
- Exposure to testosterone. This may occur when a doctor prescribes testosterone injections, implants, or topical gel for low testosterone, or when a man takes testosterone or similar medications illicitly for the purposes of increasing their muscle mass.
- Exposure to radiation.
- Frequent exposure of the testes to high temperatures, such as that which may occur in men confined to a wheelchair, or through frequent sauna or hot tub use can raise the core body temperature and may affect sperm production.
- Exposure to certain medications such as anabolic steroids, flutamide, cyproterone, bicalutamide, spironolactone, ketoconazole, antibiotics, antihypertensives, cimetidine or others, can also affect fertility.
- Exposure to environmental toxins including exposure to pesticides, lead, cadmium, or mercury.
- Damage related to cancer and its treatment, including radiation or chemotherapy. Treatment for cancer can impair sperm production, sometimes severely.
Complications of male infertility
Infertility can be stressful for both you and your partner. Complications of male infertility can include:
- Surgery or other procedures to treat an underlying cause of low sperm count or other reproductive problems
- Expensive and involved reproductive techniques
- Stress and relationship difficulties related to the inability to have a child
Prevention of male infertility
Many types of male infertility aren’t preventable. However, you can avoid some known causes of male infertility. For example:
- Don’t smoke.
- Limit or abstain from alcohol.
- Steer clear of illicit drugs.
- Keep the weight off.
- Don’t get a vasectomy.
- Avoid things that lead to prolonged heat for the testicles.
- Reduce stress.
- Avoid exposure to pesticides, heavy metals and other toxins.
Diagnosis of male infertility
Many infertile couples have more than one cause of infertility, so it’s likely you will both need to see a doctor. It might take a number of tests to determine the cause of infertility. In some cases, a cause is never identified.
Infertility tests can be expensive and might not be covered by insurance — find out what your medical plan covers ahead of time.
Diagnosing male infertility problems usually involves:
- General physical examination and medical history. This includes examining your genitals and asking questions about any inherited conditions, chronic health problems, illnesses, injuries or surgeries that could affect fertility. Your doctor might also ask about your sexual habits and about your sexual development during puberty.
- Semen analysis. You can provide a semen sample by masturbating and ejaculating into a special container at the doctor’s office or by using a special condom to collect semen during intercourse. Your semen is then sent to a laboratory to measure the number of sperm present and look for any abnormalities in the shape (morphology) and movement (motility) of the sperm. The lab will also check your semen for signs of problems such as infections. Often sperm counts fluctuate significantly from one specimen to the next. In most cases, several semen analysis tests are done over a period of time to ensure accurate results. If your sperm analysis is normal, your doctor will likely recommend thorough testing of your female partner before conducting any more male infertility tests.
Your doctor might recommend additional tests to help identify the cause of your infertility. These can include:
- Scrotal ultrasound. This test uses high-frequency sound waves to produce images inside your body. A scrotal ultrasound can help your doctor see if there is a varicocele or other problems in the testicles and supporting structures.
- Hormone testing. Hormones produced by the pituitary gland, hypothalamus and testicles play a key role in sexual development and sperm production. Abnormalities in other hormonal or organ systems might also contribute to infertility. A blood test measures the level of testosterone and other hormones.
- Post-ejaculation urinalysis. Sperm in your urine can indicate your sperm are traveling backward into the bladder instead of out your penis during ejaculation (retrograde ejaculation).
- Genetic tests. When sperm concentration is extremely low, there could be a genetic cause. A blood test can reveal whether there are subtle changes in the Y chromosome — signs of a genetic abnormality. Genetic testing might be ordered to diagnose various congenital or inherited syndromes.
- Testicular biopsy. This test involves removing samples from the testicle with a needle. If the results of the testicular biopsy show that sperm production is normal your problem is likely caused by a blockage or another problem with sperm transport. However, this test is not commonly used to diagnose the cause of infertility.
- Specialized sperm function tests. A number of tests can be used to check how well your sperm survive after ejaculation, how well they can penetrate an egg, and whether there’s any problem attaching to the egg. Generally, these tests are rarely performed and often do not significantly change recommendations for treatment.
- Transrectal ultrasound. A small, lubricated wand is inserted into your rectum. It allows your doctor to check your prostate, and look for blockages of the tubes that carry semen (ejaculatory ducts and seminal vesicles).
Treatment of male infertility
Often, an exact cause of infertility can’t be identified. Even if an exact cause isn’t clear, your doctor might be able to recommend treatments or procedures that will result in conception.
In cases of infertility, the female partner is also recommended to be checked. This can help to determine if she will require any specific treatments or if proceeding with assisted reproductive techniques is appropriate.
Treatments for male infertility include:
- Surgery. For example, a varicocele can often be surgically corrected or an obstructed vas deferens repaired. Prior vasectomies can be reversed. In cases where no sperm are present in the ejaculate, sperm can often be retrieved directly from the testicles or epididymis using sperm retrieval techniques.
- Treating infections. Antibiotic treatment might cure an infection of the reproductive tract, but doesn’t always restore fertility.
- Treatments for sexual intercourse problems. Medication or counseling can help improve fertility in conditions such as erectile dysfunction or premature ejaculation.
- Hormone treatments and medications. Your doctor might recommend hormone replacement or medications in cases where infertility is caused by high or low levels of certain hormones or problems with the way the body uses hormones.
- Assisted reproductive technology (ART). ART treatments involve obtaining sperm through normal ejaculation, surgical extraction or from donor individuals, depending on your specific case and wishes. The sperm are then inserted into the female genital tract, or used to perform in vitro fertilization or intracytoplasmic sperm injection.
When treatment for male infertility doesn’t work
In rare cases, male fertility problems can’t be treated, and it’s impossible for a man to father a child. Your doctor might suggest that you and your partner consider using sperm from a donor or adopting a child.
Lifestyle and home remedies for male infertility
There are a few steps you can take at home to increase your chances of achieving pregnancy:
- Increase frequency of sex. Having sexual intercourse every day or every other day beginning at least 4 days before ovulation increases your chances of getting your partner pregnant.
- Have sex when fertilization is possible. A woman is likely to become pregnant during ovulation — which occurs in the middle of the menstrual cycle, between periods. This will ensure that sperm, which can live several days, are present when conception is possible.
- Avoid the use of lubricants. Products such as Astroglide or K-Y jelly, lotions, and saliva might impair sperm movement and function. Ask your doctor about sperm-safe lubricants.
Alternative medicine for male infertility
Evidence is still limited on whether — or how much — herbs or supplements might help increase male fertility. None of these supplements treats a specific underlying cause of infertility, such as a sperm duct defect or chromosomal disorder. Some supplements might help only if you have a deficiency.
Supplements with studies showing potential benefits on improving sperm count or quality include:
- Alpha-lipoic acid
- Anthocyanins
- L-arginine
- Astaxanthin
- Beta-carotene
- Biotin
- L-acetyl carnitine
- L-carnitine
- Cobalamin
- Co-enzyme Q10
- Ethylcysteine
- Folic acid
- Glutathione
- Inositol
- Lycopene
- Magnesium
- N-acetyl cysteine
- Pentoxifylline
- Phosphodiesterase-5 inhibitors
- Polyunsaturated fatty acids
- Selenium
- Vitamins A, C, D and E
- Zinc
Talk with your doctor before taking dietary supplements to review the risks and benefits of this therapy, as some supplements taken in high doses (megadoses) or for extended periods of time might be harmful.
Coping and support
Coping with infertility can be difficult. It’s an issue of the unknown — you can’t predict how long it will last or what the outcome will be. Infertility isn’t necessarily solved with hard work. The emotional burden on a couple is considerable, and plans for coping can help.
Planning for emotional turmoil
- Set limits. Decide in advance how many and what kind of procedures are emotionally and financially acceptable for you and your partner and determine a final limit. Fertility treatments can be expensive and often aren’t covered by insurance.ul pregnancy often depends on repeated attempts. Some couples become so focused on treatment that they continue with fertility procedures until they are emotionally and financially drained.
- Consider other options. Determine alternatives — adoption or donor sperm or egg — as early as possible in the fertility process. This can reduce anxiety during treatments and feelings of hopelessness if conception doesn’t occur.
- Talk about your feelings. Locate support groups or counseling services for help before and after treatment to help endure the process and ease the grief if treatment fails.
Managing emotional stress during treatment
- Practice stress-reduction techniques. Examples include yoga, meditation and massage therapy.
- Consider going to counseling. Counseling such as cognitive behavioral therapy, which uses methods that include relaxation training and stress management, might help relieve stress.
- Express yourself. Reach out to others rather than holding in feelings of guilt or anger.
- Stay in touch with loved ones. Talking to your partner, family and friends can be helpful.
References [ + ]
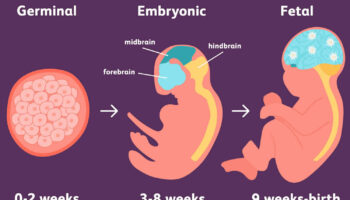

{kind=link}